On 21 January 2017, the crew of an Airbus A320 aircraft, registered VH-VNC (VNC), prepared to conduct Tigerair flight 491 (TT491) from Cairns to Brisbane, Queensland. The flight crew consisted of a training captain and a first officer under supervision. The first officer was in the role of pilot flying for the sector and the captain was pilot monitoring.[1]
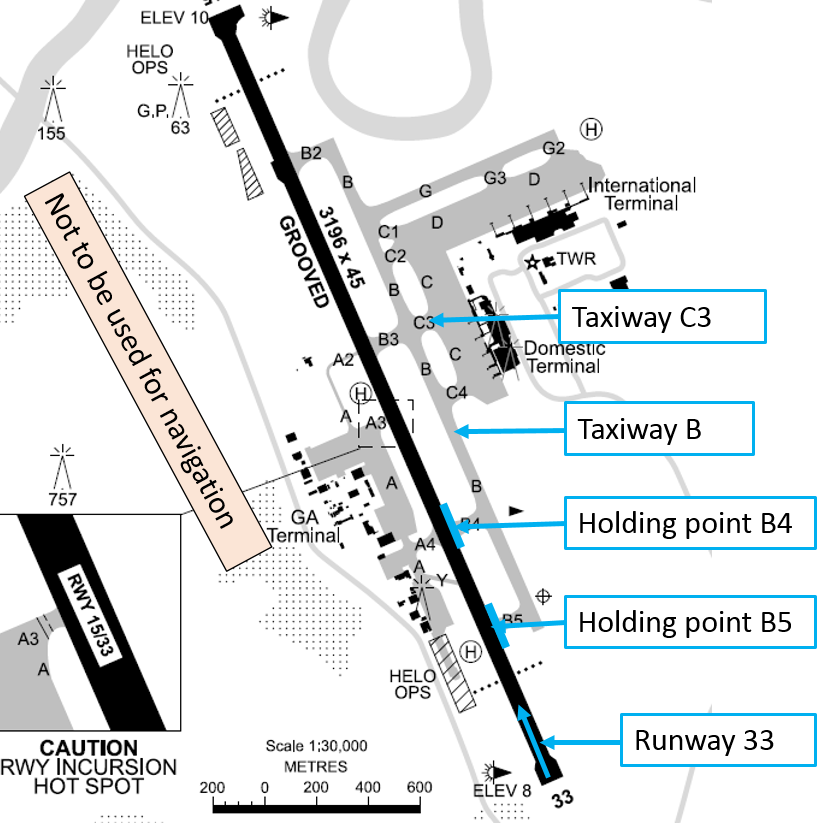
The flight crew conducted a take-off and departure briefing based on the environmental conditions and runway in use, expecting to commence the take-off roll from the B5 taxiway intersection (Figure 1). They entered the take-off data into the iPad application and loaded the data into the flight management guidance computer.
At about 1511 Eastern Standard Time (EST), the surface movement controller (SMC) cleared the flight crew of a de Havilland DHC-8 (DHC-8) aircraft that had been parked on an adjacent bay to VNC, to taxi using taxiway C3 (and B) to holding point B4. About 30 seconds later, the SMC cleared the flight crew of VNC to taxi using taxiway C3 (onto taxiway B) to holding point B5, which was the clearance they had expected. The crew had briefed each other on that taxi route.
Figure 1: Cairns Airport diagram extract
Source: Airservices Australia – annotated by ATSB
VNC then taxied behind the DHC-8 along taxiway B. As the DHC-8 turned onto the runway at B4, the first officer of VNC inadvertently also taxied to holding point B4. After completing the ‘above the line’ pre-take-off checks (see Pre-take-off checks), at about 1515, the captain of VNC advised the aerodrome controller (ADC) that they were ready for take-off. The ADC cleared VNC to line up on the runway and, as the first officer taxied the aircraft onto the runway, the flight crew completed the ‘below the line’ pre-take-off checks.
About 1 minute later, the ADC cleared VNC for take-off. Immediately after the captain read back the take-off clearance, the ADC advised the crew that they were lined up at the B4 (not B5) intersection. The crew did not respond, so the ADC cancelled the take-off clearance and instructed them to hold position. The captain then confirmed that they needed to commence the take-off from B5. The ADC cleared them to turn around on the runway, exit using B4 and taxi to B5. The aircraft subsequently took off from the B5 intersection and the flight continued without incident.
There was a 403 m difference in available runway length, between the B4 and B5 taxiway intersections.
Pre-take-off checks
The pre-take-off checklist consisted of two parts: ‘above the line’ and ‘below the line’. The crew complete the first part (above the line) before reporting ready for take-off, and the second part (below the line) after the aircraft enters the runway.
Tower comment
The captain contacted the Tower controller after the flight to thank the controller for intervening and was advised that there had been a similar incident the previous day. The ATSB could find no record of any similar occurrences at Cairns Airport.
Safety analysis
Following the DHC-8
As the DHC-8 taxied immediately ahead of VNC, the flight crew may have been distracted by following the DHC-8 to B4. Although VNC had pushed back first, the DHC-8 flight crew had received their taxi clearance and commenced taxiing before VNC. There was no specific instruction to the flight crew of VNC to follow the DHC-8.
Cabin readiness
As the first officer turned the aircraft onto taxiway B4, the captain’s attention was on communicating with the cabin crew and observing their positions on the cabin video.
One of the items on the pre-take-off checklist (above the line) is ‘cabin ready’. The captain, as pilot monitoring, temporarily handed over responsibility for ATC communications to the first officer (as pilot flying), while they confirmed the status of the cabin. Because the captain had not heard the initial indication that the cabin was ready, they looked at the cabin video to check the cabin crew were seated and called the cabin crew on the interphone, who confirmed that the cabin was secure for take-off.
The captain then took back responsibility for ATC communications and returned their focus to cockpit activities. As the captain was busy liaising with the cabin crew as the aircraft turned onto B4, the likelihood that they would notice that the aircraft was approaching the runway on the incorrect taxiway was reduced.
Training flight
The first officer had completed 11 sectors and was under the supervision of the training captain. The first officer assessed their workload at the time as moderate. This was the first officer’s second flight into Cairns since joining the operator. The captain also commented that runway 33 was not the usual runway in use at Cairns (due to the prevailing winds). A lack of familiarity with the runway may have reduced the flight crew’s ability to detect the incorrect runway position when the aircraft was lined up on the runway.
The captain commented that the first officer was taxiing slightly faster than optimal coming up to the holding point. The captain may have been focused on monitoring the progress of the aircraft to ensure the aircraft stopped before the holding line, which may have distracted them from noticing the B4 taxiway sign (to the left of the taxiway).
Normally, the pilot flying would have completed the flight controls check earlier in the taxi and well before the holding point, but the first officer completed checking the controls as the aircraft approached the turn onto B4. The captain commented that the checks were all completed correctly and in the correct order, but slightly later than normal due to the relative inexperience of the pilot flying.
Pre-take-off checklist
The relevant ‘below the line’ check to confirm that the aircraft was prepared to take-off on the correct runway, was for the pilot flying to state ‘runway 33 confirm’, then the pilot monitoring to respond ‘runway 33 confirm’. While this checklist item provided confirmation of the runway, reference to an intersection was not part of the verbal check/response.
The first officer commented that confirming the intersection as well as the runway during the pre-take-off checks may prevent a similar incident occurring.
Potential overrun
The aircraft operator reviewed the ramifications of a departure from the B4 intersection with B5 performance take-off data. Initial calculations showed that in the event of a rejected take-off, either with all engines operating or one engine inoperative, would have resulted in a runway overrun.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The first officer taxied the aircraft to the runway holding point B4 instead of B5 and may have been distracted by following the DHC-8, which taxied immediately ahead of them and took off from the runway intersection with taxiway B4.
The captain was communicating with cabin crew and looking at the cabin video as the aircraft turned onto taxiway B4, which probably distracted them from verifying that they had turned into the correct taxiway.
Neither member of the flight crew recalled seeing the B4 holding point sign (to the left of the aircraft) at any time.
The first officer was under training and had only been to Cairns once previously, and runway 33 was not the usual runway in use. Lack of familiarity with runway 33 may have reduced the flight crew’s ability to detect the incorrect runway position when the aircraft was lined up on the runway.
The air traffic controller saw the aircraft at the incorrect intersection after clearing it for take-off and alerted the crew.
There was potential for a runway overrun in a rejected take-off situation if the aircraft had commenced the take-off run from the B4 intersection.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following safety action in response to this occurrence.
Aircraft operator
As a result of this occurrence, Tigerair has advised the ATSB that they are taking the following safety actions:
Safety awareness
Tigerair has distributed a Flight Training Notice to alert training and checking crew on both the A320 and B737 fleets to the event. Tigerair Safety will be publishing the event in their next Safety Spotlight newsletter.
Safety message
This incident highlights the importance of confirming that an aircraft is lined up for take-off at the correct intersection, or position on the runway, as well as the correct runway. Confirmation of runway heading is done by checking the aircraft’s magnetic heading with the runway direction once the aircraft is lined up on the runway. The intersection should be checked before the aircraft enters the runway.
Although this incident involved the use of an incorrect intersection rather than a wrong runway, a study conducted by the US Federal Aviation Administration in 2007, Wrong Runway Departures, outlines some relevant and important points. A class 2 electronic flight bag, which shows the aircraft’s location on a moving map display, is a technological enhancement described in the study as a safety enhancement to mitigate the risk of aircraft taking off from a wrong runway. The study identified a number of factors that contributed to aircraft taking off from an incorrect runway including:
a similar layout, with one taxiway leading to an area with multiple runway thresholds located in close proximity to one another
a short distance between the airport terminal and the runway
a complex airport design
the use of a runway as a taxiway
a single runway that uses intersection departures.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
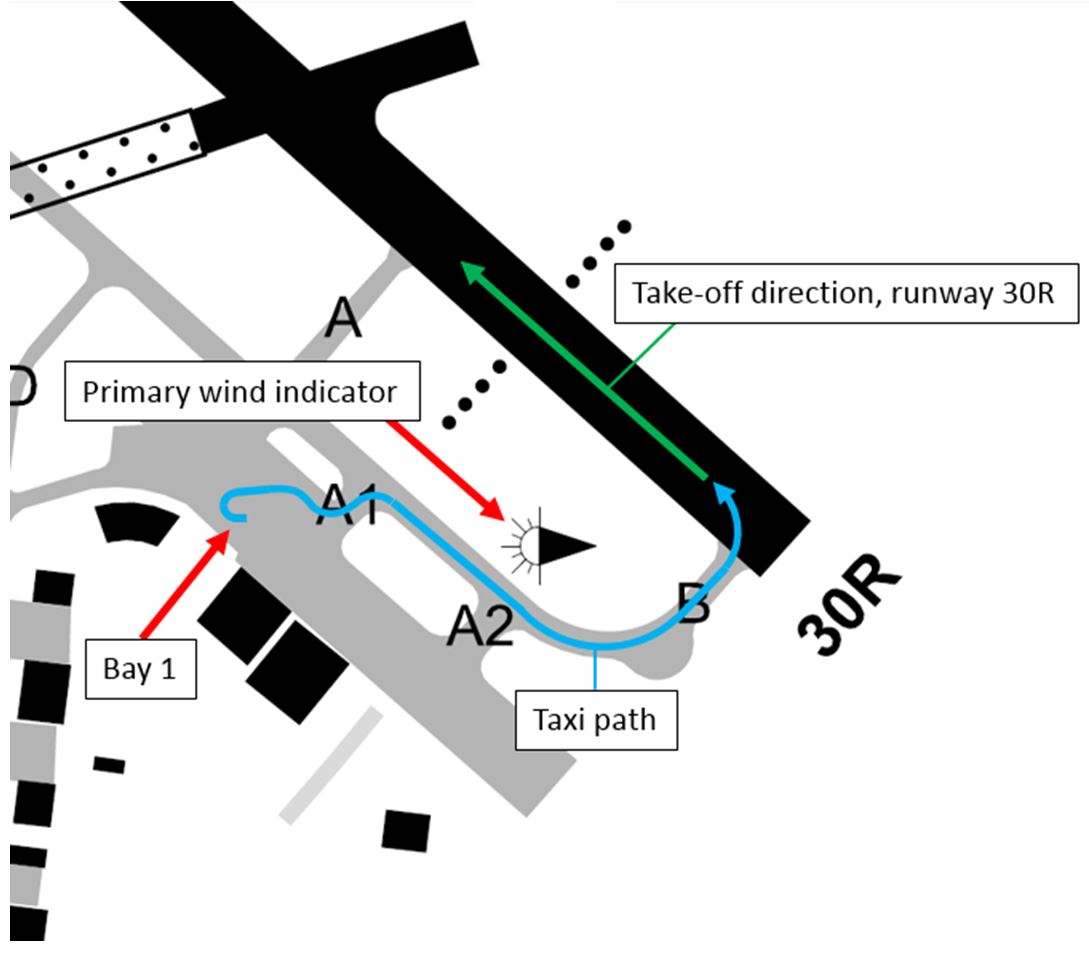
On 19 August 2016, a JetGo Australia Embraer EMB-135LR, registered VH-JTG (JTG), operated scheduled passenger flight JG65 from Tamworth, New South Wales (NSW), to Brisbane, Queensland (Qld). At 2104 Eastern Standard Time (EST), the aircraft began to taxi from parking bay 1 to runway 30 right (30R) with the taxiway and runway lights not activated (Figure 1). At 2107, the captain taxied the aircraft onto the runway and immediately began the take-off run. During the take-off run, at a speed of about 70 knots, the first officer detected the runway lights were not illuminated and activated them using the pilot activated lighting (PAL) (Figure 2). The flight crew continued the take-off.
Figure 1: Taxi path overview (both incidents)
Source: Airservices Australia, modified by ATSB
Figure 2: Take-off run of JTG on 19 August showing runway lights not activated (left) and then activated (right)
Source: Airport Operator
On 28 August 2016, the same aircraft operated scheduled passenger flight JG65 from Tamworth to Brisbane. At 1937, the aircraft began to taxi from parking bay 1 to runway 30R. As the aircraft taxied, the runway and taxiway lights extinguished (Figure 3). The flight crew continued to taxi, lined up on runway 30R and selected the aircraft landing lights on. At 1940, 48 seconds after lining up, the aircraft began the take-off run and departed runway 30R with the runway lights not activated.
No persons were injured, and the aircraft was not damaged in the incidents.
Figure 3: JTG taxiing on 28 August with runway lights illuminated (left) and then extinguished (right)
Source: Airport Operator
Runway and taxiway lighting
The taxiway and runway lighting at Tamworth Airport was controlled by a PAL system combined with an aerodrome frequency response unit (AFRU), known as AFRU + PAL. To activate the lights, pilots were required to transmit a sequence of three transmissions on the common traffic advisory frequency (CTAF). Each transmission was to have a maximum duration of 1 second with the break between transmissions being a maximum of 1 second. On receipt of the appropriate transmission sequence, the airport lights were activated and the AFRU broadcast the automatic message: ‘Tamworth Airport CTAF, runway lighting on’ on the Tamworth CTAF.
Once the AFRU + PAL system was activated, the airport lighting remained on for 30 minutes. If it was reactivated during this period, the lighting would remain on for 30 minutes from the time of reactivation. 10 minutes prior to the end of the 30-minute activation period, the primary wind indicator (windsock) lights commence flashing to warn users that the airport lighting is about to extinguish (Figure 4). In addition, an automated message ‘Tamworth Airport CTAF, lights 10 minutes remaining’ was broadcast on the CTAF to advise 10 minutes of runway lighting remaining.
Figure 4: Flashing primary wind indicator showing the windsock illuminated when the runway lights were active (left) and not illuminated (right)
Source: Airport Operator
On 19 August, at 2039, the AFRU broadcast ‘Tamworth Airport CTAF, lights 10 minutes remaining’, the lights then extinguished at 2049. At 2107, during the take-off run of JTG, the first officer broadcast an AFRU + PAL activation sequence on the Tamworth CTAF and the runway lights illuminated.
On 28 August, at 1928, the AFRU broadcast ‘Tamworth Airport CTAF, lights 10 minutes remaining’, the lights then extinguished at 1938. At 2007, an AFRU + PAL activation sequence was broadcast by another aircraft and the runway lights illuminated.
There was no indication that the AFRU + PAL system was malfunctioning on the nights of the incidents.
Captain comments
The same pilot was operating as captain of JTG during both incidents. The captain provided the following comments:
The captain did not notice that the runway lights were extinguished during either incident and were not aware until notified after each incident.
The taxiway lights at Tamworth are of the recessed centreline type. The taxi from bay 1 to runway 30R is over a rise. Therefore, only three to four taxiway lights are normally visible from the point at which you turn onto the taxiway. The captain remarked that the raised type taxiway side lights found at other airports are more easily visible.
Wind information for pre-flight planning is obtained through the flight crew electronic flight bag or automatic weather information service (AWIS). Therefore, they will only observe the windsock as a back-up, if it is available and close.
During turn-around between flights, the flight crew do not wear headsets and will not hear the 10 minutes remaining broadcast if it occurs during this time.
The responsibility for ensuring the airport lighting would be active was not assigned to either flight crewmember. There was no procedure for ensuring the airport lighting would be illuminated for the departure.
Both incidents occurred at the end of long duty days, so fatigue may have been a factor.
First officer comments – 19 August
The first officer of the 19 August incident provided the following comments:
The tiller in the Embraer 135 is located on the captain’s side. Therefore, the first officer always acts as pilot monitoring[1] (PM) during taxi. The taxi from bay 1 to runway 30R is short and a period of intense workload. During this time, the first officer did not look outside the cockpit.
The first officer did not look outside of the cockpit until the aircraft began moving during the take-off run. Once they looked outside, they immediately felt that something was not right. About five seconds later, the first officer detected that the runway lights were not illuminated.
The first officer was PM for this flight. As PM, they were able to quickly activate the PAL and resolve the issue, and did not consider aborting the take-off.
The first officer used the take-off data card for wind information and did not look at the windsock prior to departure.
First officer comments – 28 August
The first officer of the 28 August incident provided the following comments:
The first officer did not notice that the runway lights were extinguished and was not aware until notified after the incident.
The primary wind indicator at Tamworth is situated so that it is illuminated by light from the adjacent apron lighting and a red obstacle light is located above the windsock. On subsequent flights to Tamworth, the first officer has observed that this gives the appearance of the windsock being illuminated when the runway lighting is extinguished (Figure 4).
Aircraft lighting
The Embraer 135 is fitted with three landing lights and two taxi lights. The combination of these lights provides a substantial amount of illumination in front of the aircraft.
The taxi lights are used from the beginning of taxi until after departure. Prior to commencing the take-off run, the landing lights are also selected on. The landing lights provide considerably more illumination than the taxi lights.
All flight crew described the aircraft lighting as extremely effective at illuminating the runway ahead of the aircraft and reported no controllability issues during the take-off runs.
Parking apron lighting
Prior to both incidents, the aircraft parked at bay 1 for the embarkation of passengers (Figure 5). This bay is substantially lit by apron floodlights. These lights are not part of the PAL system and remain illuminated when the PAL system extinguishes the runway and taxiway lights.
All three flight crew commented that the apron lighting degraded night-vision and the short taxi from bay 1 to runway 30R did not allow time for eyes to adjust to the dark surrounds of the runway.
Figure 5: JTG parked at bay 1
Source: Airport Operator
Environmental conditions
Last light[2] on 19 August 2016 occurred at 1757, three hours and ten minutes before the take-off. At 2017, the moon was 19 degrees above the horizon and about 99 per cent visible. There was a clear sky.
Last light on 28 August 2016 occurred at 1802, one hour and 38 minutes before the take-off. The moon was below the horizon and the sky was clear.
ATSB comment
Two different PAL systems exist at Australian airports, PAL and AFRU + PAL. The activation sequence for each system is different.
CTAF recordings for the period surrounding each incident showed multiple unsuccessful attempts by other aircraft to activate the AFRU + PAL using the sequence of transmissions for a PAL system.
While this did not contribute to the incidents, pilots are reminded to be familiar with the identification and use of the different systems.
Safety Analysis
The illumination provided by the aircraft taxi and landing lights made it difficult to detect that the PAL was not activated. Due to the rise on the taxiway, the crew would only have been able to see a few lights ahead of the aircraft, and these would have been illuminated by the aircraft lights. Adding to this, both crew did not have an expectation that the lights may have been extinguished as the cues available did not assist. The auditory 10-minute PAL extinguishing warning could not be heard without headphones, and the windsock flashing light warning was not noticed as the crew obtained wind information using the flight crew electronic flight bag or AWIS.
As the company standard operating procedures did not assign a task of ensuring the runway lights were selected on to a specific role prior to taxi, there was also no procedural prompt to the crew.
The short taxi with a high workload further reduced the chance of detection.
Findings
The crew did not activate the airport lighting and did not detect that the lighting was off prior to the take-off run.
Available lighting from the aircraft taxi and landing lights, a lack of crew expectation, a short taxi with high workload, and no assigned role or procedure to check for runway lighting resulted in the crew not detecting the lack of runway lights.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to these occurrences.
Aircraft operator
As a result of these incidents, the aircraft operator has advised the ATSB that they are taking the following safety actions:
Changes to procedures
When activating the aircraft taxi lights the pilots must ensure that they confirm the status of the PAL.
When conducting night operations at an unmanned airport, the pilots must activate the PAL or AFRU + PAL by keying the microphone on the appropriate frequency unless the aircraft immediately ahead has already done so. For example, if the aircraft 10 minutes ahead has turned the lights on it will not be necessary to activate the lights again as the lights will normally remain on for a period of 30 to 60 minutes depending upon the installation.
If no traffic is evident then the pilots must activate the PAL prior to taxi for departure and within 15 nm of the aerodrome and whilst above the lowest safe altitude for arrival.
Safety message
These incidents demonstrate the impact workload stress can have on operations. The short taxi created a high workload situation which impacted on the flight crews’ ability to detect the extinguished runway lighting.
The incident on the 28 August also highlights the hazards associated with change blindness, inattention blindness and expectation bias.
Change blindness occurs when a person does not notice that something is different about the visual environment relative to before the change. Research has shown that in some cases, quite dramatic changes are not detected, particularly if changes occur when the observer is not looking at the relevant part of the visual environment at the time. In this incident the flight crew did not detect the runway lights extinguish during taxi prior to departure.
The Transport Canada article Deadly Omissions includes further information on change blindness, inattention blindness and expectation bias.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
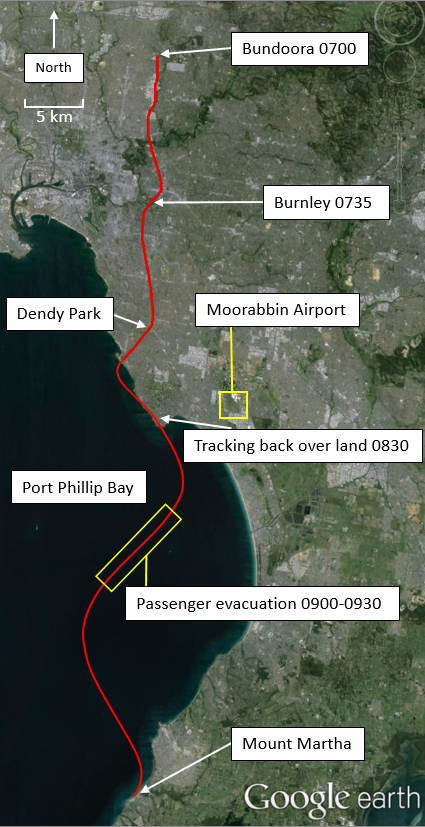
On 21 May 2016, the pilot of a Kavanagh Balloons E-240, registered VH-VBM (VBM), planned to conduct a one-hour scenic flight from Bundoora, Victoria (Vic.) with nine passengers. Prior to commencing the flight, the pilot obtained the relevant weather forecasts and observations. The wind was from the north to north-west at 5 to 10 kt. The pilot therefore assessed the balloon would track in a southerly direction and nominated potential landing sites at Burnley and Dendy Park in Brighton (Figure 1).
Figure 1: Approximate track of VH-VBM and relevant locations[1]
Source: Google earth, annotated by ATSB
At about 0700 Eastern Standard Time (EST), the balloon departed Bundoora in company with five other balloons. About 35 minutes later, the balloon arrived overhead Burnley. The pilot of VBM elected to continue to Dendy Park, along with another balloon from the same operator, to extend the flight to one hour. At that time, the pilots of four other balloons, which had been operating in company with VBM, elected to climb into a more westerly wind to track to Moorabbin Airport, Vic.
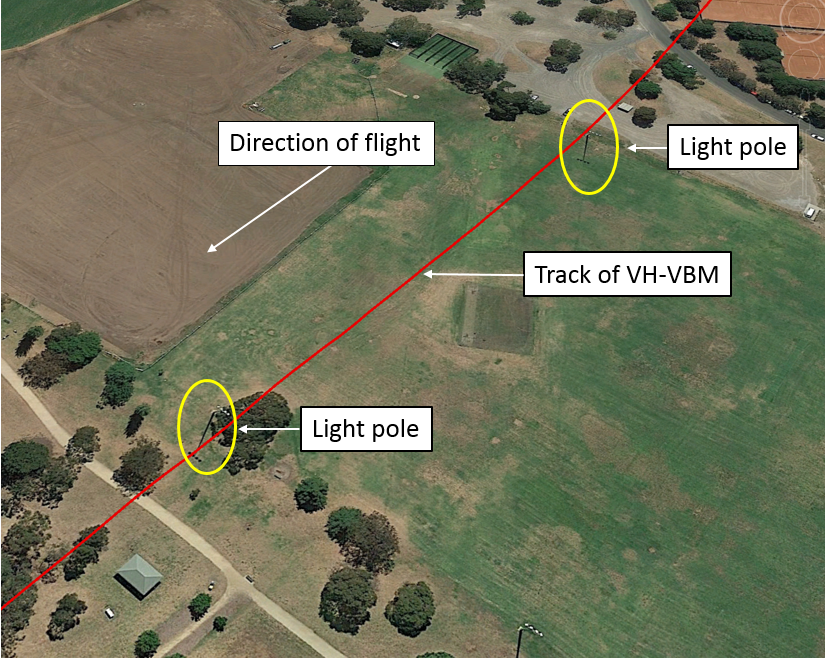
At about 0800, the balloon in company with VBM landed safely at Dendy Park. The wind speed was about 10 kt as VBM approached Dendy Park. As the balloon descended to land, the pilot sighted a light pole directly in the balloon’s path (Figure 2). The pilot then lit the balloon’s burners to climb over the pole, however, a second light pole stood directly in the balloon’s path on the far side of the available landing area. Due to the balloon’s height and the wind, the pilot assessed that the balloon may collide with the second pole if the pilot attempted a landing and therefore elected not to land in the park.
Figure 2: Dendy Park showing light poles
Source: Google earth, annotated by ATSB
The pilot then attempted to land in a golf course beyond the park, but the balloon did not track towards a safe landing area. The balloon continued at low level over parkland, however, the pilot also assessed this area to be unsafe for landing.
At about 0820, the balloon crossed the coast and tracked out over Port Phillip Bay. The pilot commenced a climb into a more westerly wind to track towards land. At about 0825, the pilot contacted air traffic control (ATC) and requested a clearance to climb to 5,000 ft. About 90 seconds later, the pilot advised that they were now at 4,000 ft and may require emergency assistance. At that time, the pilot stated that the balloon had an estimated 30 minutes of fuel remaining.
At about 0830, the balloon tracked back over land. The pilot advised ATC that in the 5 minutes it would then take to descend and land, the balloon would track back over water. The pilot elected to descend to conserve fuel and prepared for a water landing. The pilot briefed the passengers and descended about 1 km from shore. The pilot then enacted the company emergency procedures. Air traffic control recordings showed that at 0841, when asked by ATC if it was their ‘intention to ditch the balloon at the moment’, the pilot confirmed that it was.
At about 0845, the pilot established contact with the crew of a nearby vessel. The pilot coordinated with the crew of the vessel to arrange the evacuation of passengers. The passengers evacuated one or two at a time onto the vessel over the next 30 minutes (Figure 3).
After evacuating the passengers, the pilot conducted a climb to about 2,000 ft back into more favourable winds and subsequently landed safely at Mount Martha, Vic. (Figure 1).
The pilot and passengers were uninjured, and the balloon was not damaged.
Figure 3: Evacuation of passengers from VBM to vessel
Source: ABC News
Pilot comments
The pilot provided the following comments:
The ground crew assisting the balloon which landed before VBM, were available to assist the landing at Dendy Park. The pilot felt that a successful landing could not be assured even with the assistance of ground crew.
The company emergency procedures for conducting a water landing were available and clear. This greatly reduced stress and ensured the pilot and passengers were well prepared for a possible water landing.
It was not their sole intention to ditch the balloon. Ditching was one possible scenario and the pilot was preparing the balloon and passengers for that situation should it eventuate.
If they encountered similar weather conditions in future, the pilot would launch from further east. The north-easterly surface wind experienced was not forecast. In the future, the pilot would look for indicators of this wind prior to selection of a launch site.
Landing in a 10 kt wind is normally manageable, however, the light pole was in the balloon’s path (at Dendy Park).
At the time the emergency was declared, the estimated endurance was 30 minutes. Once the passengers had been evacuated the balloon endurance was greatly increased.[2]
Carriage of life jackets
No life jackets were carried on board VBM for this flight.
As the planned flight, including the expected departure and approach paths, did not include an over water component, there was no requirement to carry life jackets based on Civil Aviation Order 20.11.
Civil Aviation Safety Authority (CASA) comments
CASA provided the following comments:
While the evacuation was conducted in an appropriate manner, the locality of a suitable vessel with competent crew may have had a significant positive effect on the safe rescue, which under the circumstances, was a fortunate rather than a well-planned emergency procedure.
The company’s operations manual requires that, as soon as the balloon crosses the coastline, the ground crew be contacted and an emergency telephone call made. Immediately after this, a MAYDAY[3] is to be declared. This did not occur until the balloon was 1km out over the bay. As the pilot did not did not make a PAN or MAYDAY call as required, ATC did not have notice to apply the appropriate degree of severity to the incident. This was confirmed by Victoria Police during their incident debrief where it was highlighted that there was no communication or coordination between ATC and ground-based emergency services.
Safety message
This incident provides a good example of the value of effective emergency procedures. Despite having completed thorough pre-flight planning and preparation including weather and field selection, a number of factors combined to create a difficult situation for the pilot. Thorough emergency procedures along with regular training greatly reduced workload in the incident and assisted the pilot in achieving a safe outcome.
Declaring an emergency early, through the use of standard phrases such as ‘MAYDAY’ is vital in clearly communicating a requirement for emergency assistance or advising of an emergency situation. This enables ATC to provide assistance and coordinate emergency services without delay. The Airservices Australia safety bulletin What happens when I declare an emergency? provides further information on the actions taken by ATC once an emergency is declared.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 4 December 2015, a Scoot Boeing 787-9 aircraft, registered in Singapore as 9V-OJC (OJC) was operating a scheduled passenger flight from Changi International Airport, Singapore, to Perth International Airport, Western Australia. At about 1743 Western Standard time, OJC commenced an instrument landing system (ILS) approach to runway 21 at Perth.
During the approach, the aircraft’s autopilot flight director system (AFDS) entered a degraded mode, and presented the crew with information that they erroneously believed represented the glideslope. The crew followed the displayed information, which resulted in a descent below the designed approach path and the subsequent activation of the aircraft’s enhanced ground proximity warning system. The crew conducted a go-around, and completed an uneventful approach and landing.
What the ATSB found
During the approach, a disturbance of the ILS glideslope signal occurred, likely due to an aircraft taxiing for take‑off on runway 21, resulting in OJC capturing the ILS glideslope prematurely. Because of this, the AFDS entered a degraded mode, presenting the crew with information extrapolated from a previous position, rather than updated glideslope information.
While taking actions to reset the AFDS, the crew continued descending as per the presented information, without identifying cues that indicated the information was unreliable. This resulted in an abnormally high rate of descent, leading to a descent below the designed approach path, and activation of the aircraft’s enhanced ground proximity warning system.
The flight crew were likely experiencing higher than normal workload, due to a combination of the high speed approach and troubleshooting the unexpected glideslope indications. This reduced the effectiveness of cockpit communication and delayed correction of the aircraft’s low altitude.
What's been done as a result
The aircraft operator advised they communicated the essential elements of this event and associated AFDS implications (including primary flight display and head-up display indications) to the pilot group. Pilots have been reminded to monitor the basic flight instruments and relevant check heights during the approach, in addition to the aircraft calculated guidance.
Stabilised approach criteria and associated callouts and actions have also been emphasised. In addition, the importance of energy management and use of the HUD to monitor appropriate descent path information has been highlighted.
Safety message
Flight crew are reminded that when conducting an ILS approach in visual conditions, ILS signal paths are not protected by air traffic control, and may be subject to interference. The aircraft’s flight path needs to be constantly monitored to ensure that guidance presented to the flight crew is valid. Constant monitoring will also ensure that early action can be taken to correct any deviation from the approach path.
Safety issues and action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Scoot
As a result of this occurrence, Scoot has advised the ATSB that they communicated the essential elements of this event and the associated autopilot flight director system implications and primary flight display and head-up display (HUD) indications to the pilot group. Pilots have been reminded to monitor the basic flight instruments and relevant check heights during the approach, alongside the aircraft calculated parameters. Stabilised approach criteria and associated callouts and actions have also been emphasised, and the importance of energy management and use of the HUD to monitor appropriate descent path information have been highlighted.
This communication assisted the captain in the event on 20 April 2016 in identifying the glideslope disruption shortly after it occurred.
Context
Personnel information
Both the captain and the first officer held all licences, medical certificates and training required to operate the aircraft at the time of the incident. There was also a second officer on the flight deck who was completing an observation flight as part of his 787 training.
Both the captain and first officer had previously operated the Boeing 777 aircraft, and completed the conversion training to the Boeing 787 aircraft within six months of this occurrence.
The captain had over 18,000 total flying hours, with over 15,000 hours as pilot in command (PIC) at the time of the occurrence, including 373 hours on the Boeing 787, 338 hours of which were as PIC.
The first officer had over 5,300 hours total flying hours, with 152 on the Boeing 787, including 62 as pilot in command under supervision.
Evidence collected about the pilot rosters and sleep patterns prior to the occurrence indicated that fatigue was not likely to have been a contributing factor in this incident.
Instrument landing system signal interference
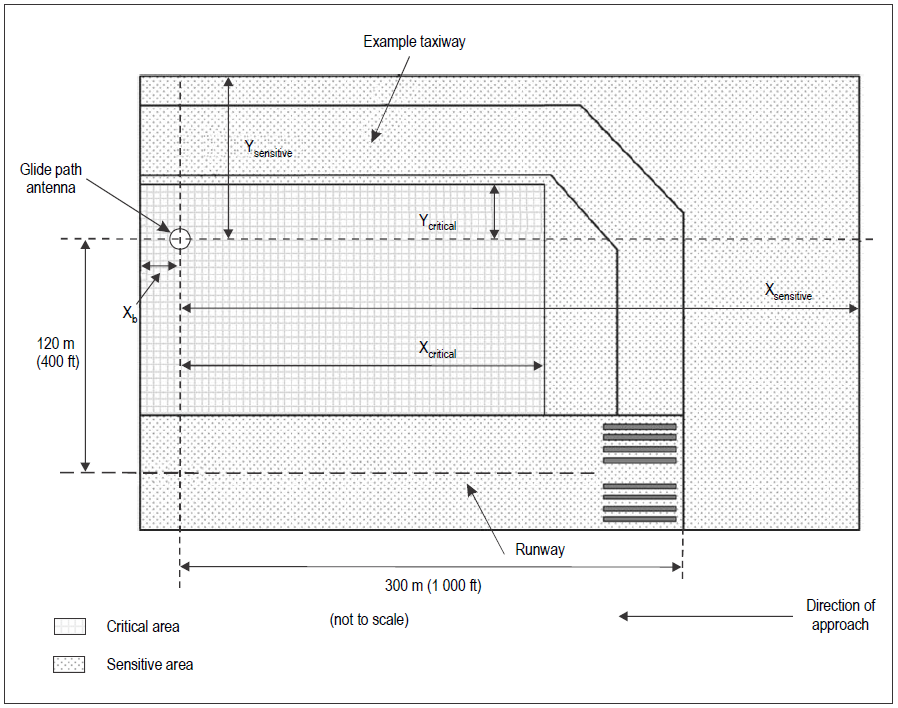
In certain conditions, the integrity of an instrument landing system (ILS) is not protected, and signal disturbances may be experienced, even while the flight crew are conducting an instrument approach. Pilots may experience ILS beam bends and other interference in circumstances where the critical or sensitive areas of the ILS are not protected.
Disturbances to ILS localiser and glideslope courses may be caused by fixed structures, such as buildings (static distortion), or moving vehicles or aircraft (dynamic distortion). The total ILS course distortion is determined by the summation of static and dynamic distortion, and this is used to define critical areas near each localiser and glideslope antenna. [7] The critical area is surrounded by a sensitive area. These areas will differ for each approach. Figure 2 shows an example of the critical and sensitive areas around an ILS antenna.
Figure 2: Example of glide path critical and sensitive area dimensions
Source: International Civil Aviation Organisation Annex 10 (2018)
Different levels of protection of the critical or sensitive areas of the ILS are provided by ATC depending on the:
type of approach being conducted
position of the aircraft on the approach
weather conditions at the time.
For low-visibility approaches, when the cloud ceiling is at or below 600 ft, or the visibility is less than 2,000 m, no aircraft or vehicle is permitted to enter the critical areas when an arriving aircraft is within the outer marker, or 4 NM (7.4 km) from the threshold if there is no outer marker. The sensitive area will only be protected if the cloud ceiling or visibility is below that required to conduct a Category 1 ILS approach.
Flight crew are requested to inform ATC if they are conducting an autoland or coupled approach. This does not, however, ensure the critical area will be protected. When the cloud ceiling is above 600 ft, or the visibility is greater than 2,000 m, neither the ILS critical or sensitive areas are protected. When an area is protected, all aircraft will be held at a holding point which is outside of the protected area.
While the weather conditions were suitable for the flight crew to conduct a visual approach, it was not standard practice to assign visual approaches to foreign carriers, unless specifically requested by the pilot, and only after the pilot reported having the runway in sight. In this case, the flight crew had the runway in sight, but had not reported this to the controller while they were continuing with the instrument approach, nor were they required to.
Around the time of the glideslope disruption experienced by OJC, a Boeing 737 taxied from Terminal 1 and took off on Runway 21 (Figure 3). The ATSB assessed that the movement of that aircraft likely caused the signal disruption.
Figure 3: Perth Airport runway 21 showing location of glide path antenna, holding points and path of taxiing aircraft prior to take-off.
Image shows the holding points for runway 21 at Perth. Between the holding points is the critical area which may be disrupted by an aircraft or vehicle movement. The red arrow shows where the 737 taxied onto the runway, likely causing a disturbance to the glideslope.
Source: Google, annotated by the ATSB.
Approach speeds
As OJC descended, ATC requested the aircraft maintain a higher than usual speed (280 kt) to maintain separation with other aircraft. The Scoot operations manual advised flight crew that their speed should be reduced to below 250 kt by 5,000 ft, subject to ATC requirements.
An Airservices Australia safety bulletin current at the time of the occurrence (2015), stated
Standard Terminal Area Arrival Speeds (STAAS) were introduced to improve safety and efficiency by bringing more predictability to arrival sequences at Brisbane, Sydney, Melbourne and Perth airports.
The STAAS speeds for an aircraft arriving were:
250 kt at or below 10,000 ft
230 kt between 20 NM and either 10 NM or the initial approach fix, unless otherwise specified on the approach chart
Between 185–160 kt between either 10 NM or the initial approach fix and 5 NM
Between 150–160 kt within 5 NM of the runway threshold.
On the Runway 21 ILS approach chart (Figure 1), the published maximum speed was 185 kt at the initial approach fix (HAIGH) and 160 kt from 5 NM. Guidance to pilots in the Airservices Australia Aeronautical Information Publication identified that:
Aircraft are expected to continue at previously specified speeds, commence speed reduction prior to the next promulgated speed and be at the speed by the specified point.
ATC may vary the published speeds where required for traffic management.
Air traffic control provided the following instructions to the flight crew:
At 1740:16, passing 20 NM, the crew were instructed to descend to 4,000 ft and reduce speed from 280 kt to desired speed
At 1741:34, passing 14.75 NM, the crew were instructed to descend to 2,500 ft and were cleared for the ILS approach
At 1742:22, around 11 NM, the crew were instructed to commence speed reduction for the approach
At 1742:55, around 9 NM, the aircraft was instructed to reduce speed to 170 kt
At 1743:32, around 7 NM, the crew were instructed to reduce to minimum speed, as the traffic ahead had slowed.
The speed change instructions were issued as the aircraft was descending and setting up to capture the localiser and glideslope for the approach, and during the early stage of the approach. As per the controller instructions, the crew were requested to reduce over 110 kt of speed in under four minutes. The flight crew reduced the speed from 280 kt to just below 200 kt in this time, having flown approximately 18 NM.
Guidance from the Flight Safety Foundation (2009) suggested deceleration on a 3° glideslope is difficult for an aircraft in a clean configuration (gear and flaps up), and can be around 10-20 kt per nautical mile with approach flaps and landing gear down. Additional deceleration can be achieved with deployment of speed brakes.
Head-up display
The head-up display (HUD) is one of the major differences between the Boeing 777 and 787 aircraft. Pilots completing a conversion course between the aircraft must complete training on HUD use, and are required to maintain currency in its use. Both pilots had completed this training.
Gibb, Grey and Scharff (2010) explain:
A head-up display projects aircraft status information to pilots to minimise their head-down time and allow more time to view the external scene outside the aircraft.
They note that the HUD is:
designed to remedy the problems associated with pilots shifting lens accommodation as they changed their gaze from close cockpit displays to far outside environmental objects.
While generally beneficial for flight crew in maintaining situational awareness, one issue which can arise with HUD use is that pilots cannot focus on both the HUD information and the outside environment simultaneously, and attention may become focused on one to the expense of the other (Crawford and Neal 2006, Nichol 2015). Wickens et al (2013) identified research showing that pilots using a HUD may be slower at identifying and responding to an unexpected event than when shifting focus between a scan of the primary flight display and the outside environment.
Additionally, as HUD displays are monochromatic, the way standard alerts displayed on the primary flight appear in colours such as green, amber and red are changed for display on the HUD (FAA, 2010). Nichol (2015) stated:
This results in the removal of a layer of information normally provided by colour coding. While the use of identical symbology and similar layout mitigates this somewhat, lack of colour is nevertheless something that pilots will take some time to adjust to.
Communication
At the time of the localiser and glideslope capture, the first officer was the pilot flying and the captain was the pilot monitoring.
In the sequence of events provided by the operator, the captain noted the aircraft was getting low, and instructed the first officer to stop the descent. The first officer reportedly did not take action at this time, as he was assessing the cautions displayed on the PFD and EICAS.
The Captain then took over flying duties from the first officer and arrested the descent. At this time, the first officer called for a go-around either two or three times. After the aural glideslope alert was sounded, the captain increased engine power and commenced the go-around. Flight data indicates that this occurred just prior to 1745.
The flight crew identified later that some standard procedural calls on the approach had been omitted during the first approach.
The approach controller coordinated handover of OJC with the tower controller between 1743 and 1744, advising that he had instructed the flight crew to reduce to minimum speed, and that there was minimum spacing between OJC and the previous aircraft. The flight crew were then instructed to change to the tower frequency. Thirty seconds later, the tower controller called the approach controller to say that the aircraft looked low. The approach controller advised that communication with the aircraft had already been transferred to the tower controller.
At 1745, prior to the go-around call from the crew, the tower controller instructed the flight crew of OJC to check altitude. At this point the crew had commenced the go-around.
Related occurrences
Subsequent Scoot occurrence
On 20 April 2016, another Scoot Boeing 787-9, registered 9V-OJD, also experienced a glideslope anomaly on the runway 21 ILS approach to Perth Airport.
In this occurrence, the flight crew observed a fluctuation of the glideslope indications, which was followed by an unusual pitch-down of the aircraft and an abnormally high rate of descent of about 1,400 fpm. The flight crew recognised the abnormal flight director commands as being the result of a glideslope disturbance, due to safety information released by the operator to their crew following the 4 December 2015 event. The autopilot was disconnected and the aircraft hand-flown to regain and maintain the appropriate flight path. The glideslope signal returned to normal function a short time later and the remainder of the approach and landing were uneventful. Following the landing, air traffic control informed the flight crew that an aircraft had departed from Runway 21 while the Boeing 787 was conducting the approach.
Both the ATSB and Boeing analysed the aircraft flight data and determined the event to be similar to the occurrence on 4 December 2015.
Other similar occurrences
A search of the ATSB database showed a number of similar occurrences had been reported to the ATSB in the five years from the start of 2015 to the end of 2019. These occurred across Australia, including on Runway 21 at Perth Airport. In most of these events, it was identified that an aircraft was taxiing, or taking off during the time of the glideslope or localiser interruption.
On 12 February 2017, a Boeing 747-47UF (freighter) aircraft was operating from Honolulu, United States to Sydney, Australia. The captain was the pilot monitoring (PM), and the first officer was the pilot flying (PF) . Shortly after the turn onto the final approach, the PF called ‘glideslope captured’ and the aircraft started to descend. However, the PM’s primary flight display was still showing the aircraft below the glideslope.
The PM crosschecked the PF’s display and noticed the glideslope was captured, then checked their own display and noticed there was a failure flag displayed for the glideslope. The PM again crosschecked the PF’s display, noticed there was a failure flag for the PF’s glideslope, and instructed the PF to disconnect the autopilot and stop the descent. During this process, a minimum safe altitude-warning alert appeared for the air traffic controller, who instructed the flight crew to conduct a go-around. At the time the 747 intercepted the localiser, another aircraft was on the taxiway within the ILS critical area.
The aircraft’s descent below the approach path glideslope occurred in daylight visual conditions following a disturbance to the glideslope signal. This analysis will examine the likely source of the glideslope disturbance, subsequent autopilot operation, and factors that contributed to the abnormal descent profile.
Glideslope disturbance
The glideslope signal disturbance occurred at about the same time that a Boeing 737 aircraft taxied and departed on runway 21. As the movement of that aircraft was in the vicinity of the ILS critical area, it was likely that this aircraft’s proximity to the antenna as it entered and lined up on the runway caused the interference to the glideslope signal.
As this event occurred in day visual flight rules conditions, and 9V-OJC was outside the outer marker of the approach when the disruption occurred there was no requirement for air traffic control to protect the ILS critical area. While weather conditions did not require the conduct of an instrument approach, it was normal for all international aircraft arriving at Perth to be sequenced via the prevailing runway instrument approach.
Approach flight path
The glideslope signal disturbance caused the autopilot flight director system (AFDS) to capture the glideslope prematurely. When an anomaly between the aircraft’s expected and actual flight paths was detected, the system by design entered into a degraded mode of operation.
The speed of the aircraft was high (206 kt) at the time the aircraft entered the degraded mode. As the descent rate required to maintain the designed glideslope is directly proportional to the speed of the aircraft, the calculated descent rate at that point in time was also relatively high. In the degraded mode, the AFDS maintained the aircraft in an attitude-stabilising mode, and in this case, with a higher-than-required descent rate. As the speed of the aircraft reduced, the difference between the required and actual descent rate increased.
A review of the recorded data indicated that glideslope mode failure indications appeared on both the primary flight displays and the head-up displays, however the flight crew did not recall seeing this initially. In addition, an ‘AUTOPILOT’ caution message should have been displayed on the engine-indicating and crew‑alerting system, but again the crew did not see this at the time. As they did not notice any warnings, the crew continued to descend as per the displayed flight director information. The crew reported they only observed the indications after hearing the aural ‘GLIDESLOPE’ caution.
Recorded flight data indicated that the crew manually disconnected the autopilot, and deselected and reselected the flight directors after the autopilot entered the degraded mode, when the aircraft was at 2,150 ft. The flight crew did not recall these actions, likely due to the workload at the time.
The actions of disconnecting the autopilot and re-selecting the flight directors re-set the AFDS, resulting in localiser (LOC) and vertical speed (V/S) modes becoming active with the glideslope (G/S) mode armed. However, as the aircraft’s flight path was diverging below the glideslope, the glideslope approach mode did not become active.
Based on analysis of the recorded flight data, it appears that, following autopilot disconnect and re-selection of the flight directors, the flight crew did not confirm the activation of the glideslope approach mode. As the aircraft was diverging below the glideslope in V/S mode, the glideslope mode remained in the armed (white) mode and not the active (green) mode. Consequently, rather than providing guidance to maintain the glideslope, the flight directors were providing guidance to maintain the descent rate approximate to that which existed when the modes were reselected.
This led to a descent rate about 1,000 feet per minute higher than was required for the approach, and in excess of the permitted rate of descent to comply with the operator’s stabilised approach procedures. Based on the flight path flown, it appears likely the flight crew misinterpreted the flight director commands as guidance to maintain the glideslope.
Workload
Periods of high workload are a normal function of the various stages of a flight, particularly during take-off, approach and landing. Workload during these periods is managed by following standard operating procedures and effective communication and teamwork, both between the pilots and with air traffic control.
While pilots are trained to operate under a range of conditions, familiarity and recency with an aircraft type can affect a pilot’s ability to manage these high-workload situations. The pilot flying had experience on the Boeing 777, but had only been operating on the Boeing 787 for a few months, and was likely still developing expertise specific to this aircraft type.
The Boeing 787 was also the first aircraft where the pilot flying had experienced using a head-up display. While head-up displays have been identified to be preferred by pilots over traditional head-down displays, they are known to have a potential inattentional blindness effect, meaning that pilots may inadvertently focus on one piece of information to the detriment of others (Gibb, Grey and Scarff, 2010).
The high-speed descent clearance given to the crew of OJC, while not unusual, was continued below the operator’s normal limit of 5,000ft. The air traffic controller directed the crew to use ‘desired speed’, an instruction that permitted the crew to reduce speed, but the flight crew did not slow the aircraft. The crew only began slowing the aircraft when cleared for the approach. This put OJC closer to the proceeding aircraft and, to ensure separation was maintained, the controller directed the crew to reduce speed to 170 kt, then to minimum speed. This was a relatively large speed reduction, to be completed in a limited time, which resulted in a further increase in workload for the crew.
The high-speed descent and subsequent high-speed approach also meant that there was limited opportunity for the crew to identify any abnormal attitude changes associated with the glideslope disturbance. In interview afterwards, remarks by the pilot flying about being mindful of the need to slow down, the deviation from normal speeds, the time taken to process the meaning of indications displayed on the HUD and PFD, and the communication and control changes between the crew were likely indicative of a higher-than-normal workload.
About 25 seconds after capturing the glideslope, the autopilot was manually disconnected and the pilot monitoring (captain) made several rapid changes to the flight directors and approach modes. Those actions appear to have been performed in response to the unusual indications displayed following the glideslope disturbance. They also appear to have been actioned without the usual action and confirmation as required by normal standard operating procedures.
As a consequence of not confirming the status of the reselected modes, both flight crew members appear to have experienced a degree of autopilot and flight director mode confusion. The crew incorrectly assumed that the correct glideslope information was being displayed, and did not notice any indications to the contrary. The high workload may also explain the discrepancy between when the flight crew thought they disconnected the autopilot and when the recorded data indicated the disconnection occurred.
Reports from the flight crew that they missed making, and/or did not hear some of the required standard approach calls, including the altitude crossing check at the outer marker, indicate some task-shedding occurred due to the high workload.
Findings
From the evidence available, the following findings are made with respect to the flight below minimum altitude involving Boeing 787, registered 9V-OJC, on 4 December 2015.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Contributing factors
The aircraft prematurely captured the runway 21 glideslope as a signal anomaly occurred, most likely caused by another aircraft taxiing to take off on the same runway. This resulted in the autopilot flight director system reverting to a degraded mode of operation.
Following disruption to the glideslope, the crew descended the aircraft unaware that the information they were following was taking them below the ILS glideslope, leading to activation of the aircraft's ground proximity warning system.
The flight crew were likely experiencing higher than normal workload, due to a combination of the high speed approach and troubleshooting the unexpected glideslope indications. This reduced the effectiveness of cockpit communication and delayed correction of the aircraft’s low altitude.
The occurrence
On 4 December 2015, a Scoot Boeing 787-9 aircraft, registered in Singapore as 9V-OJC (OJC), was operating a scheduled passenger flight from Changi International Airport, Singapore, to Perth International Airport, Western Australia. The first officer was the pilot flying (PF), and the captain was the pilot monitoring (PM)[1]. Also on the flight deck was a second officer conducting his first observation flight as part of his training on the 787 aircraft.
During the descent into Perth, Air Traffic Control (ATC) cancelled the normal speed restriction of a maximum of 250 kt below 10,000 ft, and requested the flight crew maintain 280 kt. This higher‑than‑normal speed was required to allow sequencing with other arriving traffic.
At about 1736 Western Standard Time,[2] as the aircraft was approaching 9,000 ft, the crew contacted the Perth approach controller and were instructed to maintain 9,000 ft. About a minute later, they were cleared to descend to 5,000 ft. At this time, the flight crew had a conversation about the speed they were flying being higher than the operator’s guidelines, which recommended a speed no greater than 250kts below 5,000 ft. The captain subsequently instructed the first officer to maintain the higher speed, as per the ATC instructions.
At 1740, after being cleared to descend to 4,000 ft, the crew reported to the controller that they were still maintaining 280 kt. In response, the approach controller advised the crew to resume their desired speed. The standard arrival speed at this point was 230 kt.
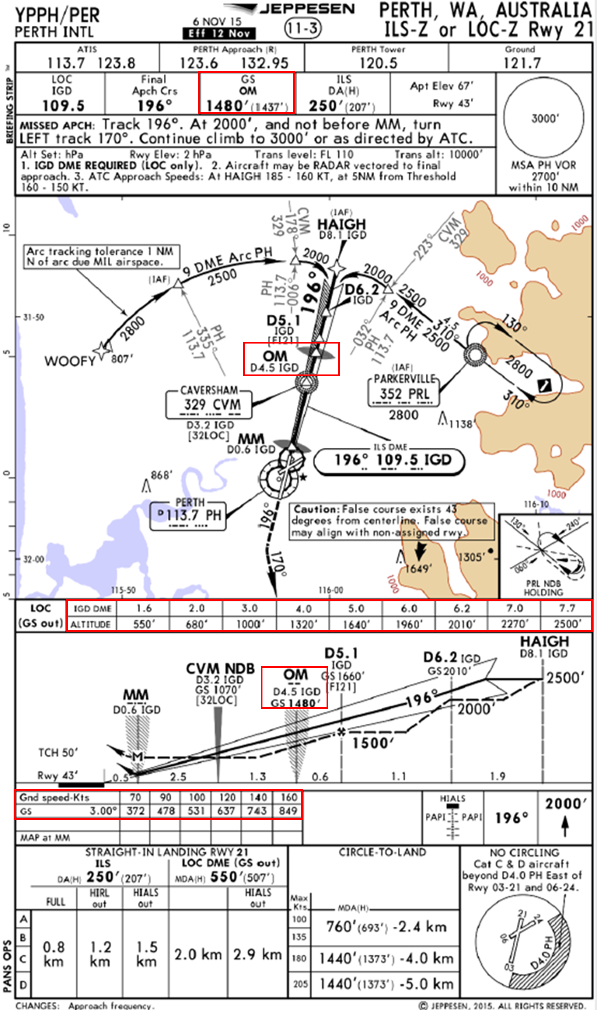
At 1741, the flight crew were cleared for a further descent to 2,500 ft and were given clearance to conduct the Runway 21 Instrument Landing System[3] (ILS) approach (Figure 1). At 1742, the approach controller instructed the crew to reduce speed for the approach. After 30 seconds, the crew were instructed to reduce speed further to 170 kt. At this time, the aircraft was approaching waypoint HAIGH, the initial approach fix (IAF) of the ILS approach, at an altitude of 2,600 ft and with an airspeed of about 240 kt. The published arrival speed from HAIGH was between 160 kt and 185 kt.
At 1743:13, both the ILS localiser (LOC) and glideslope (G/S) functions appeared to have been captured normally, with flight crew noting green indications for both on the flight mode annunciation panel. At this point, the aircraft was clear of cloud and the flight crew had the runway in sight. The Perth Automated Terminal Information Service identified the visibility as greater than 10 km, and the cloud as ‘FEW’[4] at 3,000 ft.
At 1743:32, the aircraft was directed by ATC to slow to the minimum approach speed. At 1744, the aircraft approached the outer marker (OM) (Figure 1) while descending through an altitude of about 1,000 ft, with a descent rate of about 1,800 fpm and an airspeed of 184 kt. This altitude was about 500 ft below the required height for this point of the approach, with a descent rate about double that required to maintain the glideslope.
A review of recorded Continuous Parameter Logging flight data after the incident indicated that, at around the time of the glideslope capture, there was a three‑second disturbance to the glideslope signal. This disturbance should have appeared as a slight oscillation of the glideslope indications on both the primary flight displays (PFDs) and the head-up displays (HUDs). The flight crew later reported that they did not notice the disturbance. The data further showed that the glideslope was prematurely captured by the autopilot flight director system (AFDS). As a result of the temporary disturbance, the AFDS entered a degraded mode of operation several seconds after the disturbance. At the time this occurred, 1743:36, the aircraft was at a distance of about 7 DME[5] (about 13 km) from the Runway 21 threshold, and past the initial approach fix waypoint HAIGH, descending through 2,120 ft with a descent rate of about 1,300 feet per minute (fpm) and an airspeed of 206 kt.
Figure 1 - Perth runway 21 ILS approach chart used by Scoot flight crew
Red boxes show the expected height at the outer marker (1480 ft when 4.5 nm from runway threshold), required altitudes to maintain the three degree glideslope for the approach, and the expected decent rate in feet per minute to maintain the glideslope for a range of approach speeds.
Source: Jeppesen annotated by ATSB
In the degraded mode, the glideslope flight path was no longer tracked by the AFDS, and instead the AFDS entered an attitude-stabilising mode based on the inertial data existing at that time. The resulting descent rate guidance displayed to the flight crew on the flight director was higher than that required to maintain the published 3° approach path.
The flight crew did not recall seeing any of the indications in the flight deck about the degraded AFDS mode, which should have normally displayed as both an amber line displayed through the G/S active mode text on the PFD, and as a line through the G/S active mode text on the HUD. In addition, an ‘AUTOPILOT’ caution message should have been displayed on the engine indicating and crew alerting system (EICAS). The flight data indicated that the autopilot was manually disconnected at 1743:38, two seconds after the AFDS entered the degraded mode, and the flight directors were cycled off then on again at 1743:45 with the intention of resetting the AFDS. The LOC and V/S modes then became active.
At 1744:24, the flight crew received an aural ‘GLIDESLOPE’ alert from the aircraft’s enhanced ground proximity warning system, indicating an excessive deviation below the required glideslope approach path. The flight crew later recalled that it was after receiving the ‘GLIDESLOPE’ caution alert that they observed a line through the G/S text on their PFDs and failure mode indication on the HUDs. The first officer reported also observing an ‘AUTOPILOT’ caution message on the EICAS at about this time. These indications are consistent with the AFDS degraded mode. Flight data indicated that the crew were taking action to respond to the degraded mode just prior to the aural alert. Resetting the flight directors resulted in the LOC and Vertical Speed (V/S) modes becoming active. The G/S mode remained armed, but did not become active.
In response to the alert, the captain then instructed the first officer to ‘power up’ and stop further descent. The first officer did not respond at this point, as he was reportedly still managing the energy of the aircraft to slow the approach down, and assessing the caution messages received.
As the aircraft passed over the OM, it descended through 930 ft with an airspeed of 180 kt, and a descent rate of 1,700 fpm. The required height at this point was 1,480 ft, the target approach speed was 156 kt, and a descent rate of about 850 fpm. The procedural approach speed limit was 160 kt. At this time, the captain took control of the aircraft with the intention of arresting the descent rate, correcting the flight path, and continuing the approach. However, the first officer advised the captain that the approach was outside the company’s stable approach criteria and recommended they conduct a go-around. As this was occurring, the flight crew visually observed that the precision approach path indicator (PAPI)[6] lights were all red, indicating the aircraft was significantly lower than required for the approach, and commenced a go-around.
At about 1745, the Perth Tower controller asked the crew to confirm they had visual reference with the runway, and to check their altitude. At that stage the aircraft had climbed to an altitude of 650 ft. The crew responded to the controller, advising that they were conducting a go-around.
A minimum altitude of 590 ft (520 ft above the ground) was recorded at 1744:47, when the aircraft was at 3.5 DME (5 km) from the runway, at a position where the glideslope height was 1,160 ft. The time between the first aural ‘GLIDESLOPE’ caution and commencement of the climb in the go-around was 23 seconds.
The aircraft subsequently conducted another ILS approach to the same runway. There was no signal disturbance during that approach and the ILS was conducted in accordance with the prescribed procedure. The aircraft landed at about 1758.
The sources of information during the investigation included:
the crew of 9V-OJC
Scoot
Airservices Australia
Boeing.
References
Airservices Australia (2015), Safety Bulletin – Standard Terminal Area Arrival Speeds. 23 January 2015.
Crawford, J and Neal, A (2006), A Review of the Perceptual and Cognitive Issues Associated with the Use of Head-Up Displays in Commercial Aviation. International Journal of Aviation Psychology, Volume 16, Number 1 pp 1-19.
Federal Aviation Administration (2010); Advisory Circular AC-25.1322-1 Flightcrew Alerting. US Department of Transportation, Federal Aviation Administration.
Flight Safety Foundation (2009), Approach and Landing Accident Reduction Toolkit Briefing note 4.2 – Energy Management. Flight Safety Foundation.
Gibb, R, Gray, R and Scharff, L (2010), Aviation Visual Perception. Ashgate, United Kingdom
International Civil Aviation Organisation (2018); Annex 10 – Aeronautical Telecommunications Volume 1 Radio Navigation Aids. Seventh Edition, July 2018. International Civil Aviation Organisation.
Nichol, RJ (2015), Airline Head-Up Display Systems: Human Factors Considerations. International Journal of Economics and Management Sciences, Volume 4, Issue 5.
Wickens, CD, Hollands, JG, Banbury, S and Parasuraman, R (2013); Engineering Psychology and Human Performance. Fourth Edition. Pearson Education.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the crew of 9V-OJC, the operator, Airservices Australia, Boeing, the Civil Aviation Safety Authority, the National Transportation Safety Board (United States) and the Transport Safety Investigation Bureau (Singapore)
Submissions were received from the operator, the Transport Safety Investigation Bureau (Singapore) and Boeing. The submissions were reviewed, and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On final approach to Launceston, maximum nose-up stabiliser trim was insufficient to trim out the nose-heavy force. After landing it was found that 60 golf bags weighing approximately 1,300 kg had not been included on the aircraft load trim sheet. The golf bags belonged to a tour group of 60 people who were to travel some days after this occurrence. They were bulk delivered to the baggage handling area at Melbourne Airport to be forwarded to Launceston on a space available basis to meet a requirement that they be available when the group arrived.
The load controller and the baggage loaders were aware that the golf bags were to be moved on a space available basis. The operator's Ramp Manual requires that a load plan must be prepared for each flight. It states that a load plan is an instructional document which specifies where cargo, special load items, livestock, mail, and baggage are to be loaded on an aircraft. The document is produced by the load control section and distributed to members of the loading team so they can perform their duties in the correct loading of the aircraft.
It is necessary to follow the load plan to ensure that the load is correctly segregated and all weight and balance requirements are met. When the loading of an aircraft differs from the load plan, the load controller is to be consulted. On this occasion the loading supervisor informed the load controller that the aircraft was full but did not tell him that the 60 golf bags were on board. The load controller was aware that low density cargo was on board. He had not considered it possible to load the golf bags as well and they were not included in the load plan.
At the time of the occurrence, the load plan declaration stated:
This aircraft has been loaded in accordance with these instructions except for the deviations recorded. The load has been secured in accordance with company regulations. The loading supervisor did not sign the declaration, nor did the load controller seek such certification prior to completing the load and trim sheet. Two load conditions are shown in the following list.
The first column is the load displayed on the load plan accepted by the crew. The second column is the estimated load with the extra 60 golf bags.
Load displayed on the load plan accepted by the crew
Estimated load with the extra 60 golf bags
Bay 1 (most fwd) 26 kg
350 kg
Bay 2 26 kg
472 kg
Bay 3 260 kg
468 kg
Bay 4 212 kg
212 kg
Bay 5 325 kg
500 kg
Bay 6 (most aft) 325 kg
500 kg
Bays 1 to 4 are in the forward fuselage and received most of the extra load, thereby adding to the forward centre of gravity.
The horizontal stabilizer trim setting listed on the load trim sheet was 1.3 units nose up. The crew did not notice any extra nose-down moment during takeoff. It only became evident during the approach and landing. The investigation team recalculated the trim, taking into account the most probable baggage loading condition. It was concluded that the aircraft was still just within the forward limit of the centre of gravity envelope at take-off. The required take-off horizontal stabilizer trim setting would have been 2 units nose up on a 3-unit scale. VH-FKO was the most nose-heavy F28 in this operator's fleet.
The load controller stated that to compensate for this he had blanked out the front row of four seats. However, the computer-generated load trim sheet showed that the aircraft was "trimmed by seat row" and, using the code "BLKD 0", showed that no seats were blocked. The requirement for the front row of four seats to remain unoccupied because of balance considerations was not brought to the attention of the cockpit and cabin crews. The aircraft had a fuel load of 4,400 kg in the wing tanks. No fuel was carried in the centre tanks.
The centre of gravity moved rearwards with fuel burn. There were 65 passengers including 4 infants who occupied 61 out of 74 seats. The investigation did not determine if passengers were redistributed in the cabin after takeoff, resulting in some or all of the four front seats being occupied. When combined with the nose-down force generated by the weight of the 60 golf bags, any forward movement of passengers would have moved the centre of gravity up to or just outside the forward limit, depending on how many of the front row seats were occupied.
The operator uses a system of standard passenger and baggage weights rather than actual weights when compiling a load trim sheet. Accordingly, the actual weights on this flight could not be determined.
ANALYSIS
Most passenger jet aircraft have a large centre of gravity range and variations from a load plan may be permissible provided the aircraft is loaded within the centre of gravity limits. The F28 aircraft type has only a small tolerance to variations from a load plan which conforms to the manufacturer's specifications. The loading supervisor did not certify that the aircraft had been loaded in accordance with the operator's instructions. Certification is part of the operator's quality assurance safety net.
On this occasion the safety net failed. The reason the documentation was not signed could not be clearly established. The operator stated that the reason the loading supervisor did not sign the load plan was an industrial issue rather than a safety issue. The reason maximum nose-up stabiliser trim was insufficient to trim out the nose-heavy force during the approach and landing was not determined.
Findings
1. The cargo and baggage were not loaded in accordance with the load plan.
2. The 60 golf bags were not included in the weight and balance calculation on the load trim sheet.
3. Some passengers may not have been seated in accordance with the load plan during the approach and landing.
4. Maximum nose-up stabiliser trim was insufficient to trim out the nose-heavy force during the approach and landing.
Significant factors
1. The loading supervisor did not certify for the accuracy of the loading and did not ensure that the load controller was aware of the difference between the load plan and the actual loading.
2. The load controller did not advise the cockpit and cabin crews that the front row of four seats was not to be occupied due to balance considerations.
SAFETY ACTION
The Bureau of Air Safety Investigation issues safety advisory notice SAN 960031 to the Civil Aviation Safety Authority. The Bureau of Air Safety Investigation informs the Civil Aviation Safety Authority that it is possible, unless adequate notification is given to cockpit and cabin crew, that the movement and reseating of passengers can inadvertently cause an out of balance situation of certain aircraft under certain loading conditions. Furthermore, as a result of this occurrence, the operator advised that it had initiated the following
Safety actions
1. Established an aircraft load management group. This group compromises company personnel dedicated to establishing operating procedures to ensure aircraft are loaded in accordance with regulatory and company requirements. The group is also required to conduct audits of all operator ports to ensure all requirements are being met in the field and to develop a training syllabus for all staff involved with the loading of aircraft.
2. Initiated an aircraft load management training course. This course is designed for state managers, operations managers, ramp supervisors, load controllers, senior clerks, senior freight clerks and leading hand loaders. The course syllabus covers all aspects of aircraft loading, weight and balance and the legal requirements of the Civil Aviation Regulations and Civil Aviation Orders.
3. Developed an aircraft abnormal loading alert form to provide staff with a method of reporting any incidents or events which may compromise company procedures or matters of safety with regard to the loading of aircraft.
4. Introduced a requirement for the leading hand who loaded the aircraft, to sign a declaration on the load sheet. The declaration states: "I certify that: - loading staff have been instructed to load this aircraft in accordance with the load plan - all deviations from the load plan have been reported - all ULDS [container] and bulk cargo have been loaded and secured in accordance with company procedures".
5. Appointed a national ramp manager to co-ordinate ramp and loading procedures across the network of ports used by the operator.
6. Introduced a system of examination and certification of the load controllers within handling companies on the international network. A similar scheme is being introduced for the domestic network.
7. Introduced an enhanced computerised weight and balance system. This system provides more automation to the loading process and will be introduced to enhance the documentation for the ramp staff.
8. Provided improved communications between the load controller and leading hand loaders with the introduction of two-way radios at the major stations.
The crew of VH-EWD had flight planned for a regular public transport flight from Canberra to Coolangatta using the route designator C4CBCGXX where XX is the modifier for that particular route. The Melbourne computer aided flight strip printing system interpreted the XX modifier as a track via Bindook and Sydney. The systems used by the airline and Canberra Air Traffic Services (ATS) interpreted XX as a track via Yass and Mudgee.
The Civil Aviation Authority (CAA), while retaining the XX modifier, had recently changed the applicable route from Bindook/Sydney to Yass/Mudgee. The airline and Canberra ATS had effected the appropriate software changes for the route modifier whereas Melbourne ATS had not.
EWD departed Canberra at 0850 EST and tracked via the Yass/Mudgee route as expected by Canberra Air Traffic
Control (ATC).As the vertical limit of Canberra ATC is 10,000 ft, co-ordination procedures between Canberra and Melbourne Sector require the notification of an impending departure to be given to Melbourne prior to the aircraft becoming airborne.On this occasion co-ordination was not carried out until after EWD had departed.
Additionally, when Canberra Approach informed Melbourne Sector of EWD's departure, the controller incorrectly referred to the aircraft as EWG.
On receiving the departure advice, the Melbourne controller actioned his EWD flight strip and changed the callsign to EWG. The track details on his strip indicated a track via Bindook and Sydney. As there was no other traffic in that portion of airspace, he elected to wait until he had confirmed the callsign with Canberra and observed the aircraft on radar before taking any additional amendment action. At 0853 Melbourne Sector contacted Canberra Approach to confirm the callsign of the aircraft on the Yass track as their radar was indicating EWD.
Further co-ordination took place between Melbourne and Canberra, which confirmed that the Coolangatta bound aircraft was tracking via Yass and Mudgee. The Melbourne controller subsequently amended all details held in the Area Approach Control Centre for the flight and EWD proceeded without incident.There was no breakdown in separation and the transfer of responsibility from Canberra to Melbourne was performed in accordance with the prescribed procedures.
CONCLUSION
Significant Factors
The following factors were considered relevant to the development of the incident.
Melbourne ATS had not made the necessary software changes for the route, thus the route modifier being used by Melbourne ATS was incorrect.
Canberra Approach Control did not co-ordinate the impending movement of VH-EWD with Melbourne Sector prior to its departure.
Canberra Approach Control subsequently used an incorrect callsign when co-ordinating VH-EWD's departure.
SAFETY ACTION
In response to safety deficiencies identified during this investigation the CAA amended their procedures for the allocation of route designator modifiers.The CAA airspace and air-route structure reviews are changing the parameters of design in respect to these problems and intend that all the new air routes will require new route modifiers for flight planning purposes.
The flight plan for the aircraft, Sydney to Hong Kong, was received at Brisbane Air Traffic Control at approximately 1130 hours EST with a planned departure time from Sydney of 1300 hours. A departure message was received at 1325 hours. No other flight plan details were received on the aircraft by either Brisbane or Darwin Air Traffic Control.
At 1540 hours, the aircraft reported at Mt Isa, estimating position BROCK at 1600 hours. According to the flight plan, the next position reporting point should have been GOVE. There was no conflicting traffic and the aircraft was cleared via BROCK.
Twenty minutes prior to the aircraft's departure from Sydney, the aircraft commander was advised of an increase in zero fuel weight for the aircraft and amended the flight plan as a result. The handling agent for the operator failed to submit the updated plan. The reason for this omission was not determined.
The aircraft departed Sydney at 0752 hours EST on a scheduled commercial air transport flight, landing at Cowra and Young before terminating at Forbes at 0940 hours. The aircraft subsequently departed Forbes at 1545 hours for the return flight to Sydney via West Wyalong, Forbes, Young, and Cowra, departing Cowra at 1815 hours with six passengers on board.
During the flight the pilot was monitoring the fuel state, and became concerned that there may not be sufficient fuel on board to reach Sydney. When the aircraft was overhead Camden, the pilot saw the right hand fuel contents gauge indicating near empty and immediately decided to divert to Bankstown. Sydney Approach advised the pilot that the aircraft was closer to Hoxton Park. As a result, the pilot elected to divert to Hoxton Park, landing at 1856 hours at an estimated weight of 2765 kg. The aircraft was refuelled, departed Hoxton Park and landed safely at Sydney. Hoxton Park has a pavement restriction which restricts normal aircraft operations to aircraft up to a maximum take-off weight of 1350 kg.
Prior to departing Forbes, the pilot had calculated the aircraft fuel requirements, and was satisfied that adequate fuel remained to complete the flight without refuelling. However, he had made an error in his calculations, and had omitted to take into account fuel consumed during take-off and climb as required by the company fuel policy.
SIGNIFICANT FACTORS
The following factors were considered relevant to the development of the incident.
1. The pilot failed to accurately determine the total fuel required for the flight from Forbes to Sydney.
2. During the sector from Cowra to Sydney, the pilot realised there was insufficient fuel in the aircraft to safely complete the flight.
3. As a result of the late appreciation of the aircraft's critically low fuel state, the pilot was forced to divert to an aerodrome suitable for Piper PA 31 operations only in emergency situations.
The pilot of a motorised glider declared an inflight emergency to Flight Service, advising that he was above cloud, south-west of Camden, with 50 minutes fuel endurance. The aircraft was not equipped with a transponder but carried a Global Positioning System. An alert phase was declared and, following liaison with Sydney Approach, the aircraft was located by primary radar returns. The alert phase was later upgraded to a distress phase when it was apparent that the aircraft would shortly run out of fuel while still above thick cloud.
Communications with the aircraft ceased until a 'Careflight' helicopter finally made contact with the pilot, who indicated that the aircraft had run out of fuel and was gliding. The 'Careflight' pilot subsequently reported that the glider had landed, and the pilot was uninjured. The glider pilot later reported that he had planned to fly from Gulgong to Camden. The weather forecast indicated that the weather on the coast was poor, with extensive low cloud. However, by his own observation, the weather was fine to the south of Gulgong. The aircraft was winch launched to a height of 1,500 ft at Gulgong before departing to the south with an almost full fuel tank (22 litres maximum), with the pilot intending to divert to Bathurst if necessary.
The weather south of Bathurst continued to improve, but low cloud cover extended to the east towards the coast. By the time he had thermalled to 9,500 ft the glider pilot said he was about 80 km west of Camden and some 10 km west of the line of cloud. After contacting Camden tower for the current weather situation, the pilot assessed that he could continue in accordance with the Visual Flight Rules and land at Camden. After gliding down to 6,500 ft, the motor was started and he continued towards Camden, above cloud. However, further contact with Camden tower indicated that the weather had deteriorated and there was now almost total cloud cover.
The pilot contacted Sydney Centre for a clearance into controlled airspace and held for some time about 20 km west of Camden to assess the weather. As there was no improvement, he was authorised to climb to 10,000 ft so that he could then glide to the west, beyond the cloud line, into suitable outlanding country. At 10,000 ft the engine stopped when the fuel was exhausted. However, the engine could not be retracted by normal or emergency methods, severely restricting the glide performance of the aircraft. Unable to now reach the end of the cloud line, and descending into wispy cloud, the pilot finally found a hole in the cloud and spiralled down to land in a small paddock.
After touchdown the pilot had to ground loop the glider to avoid colliding with a fence, resulting in damage to the landing gear. The pilot subsequently reported that after checking and re-crimping the electrical wiring for the engine retract motor, the engine retracted normally.
At approximately 1300 CST, 7 June 1995, a military aircraft suffered a landing gear failure during the landing roll on runway 11 at Darwin. The aircraft ground looped through 180 degrees, coming to rest on the northern (left) side of the runway between taxiways B2 and E2, with about 0.4 m of its left wingtip overhanging the runway.
Not long after that occurrence, the crew of VH-TJV, which was on descent to Darwin, was advised by Air Traffic Control (ATC) of the accident. They were given the location of the disabled aircraft and informed that runway 11/29 would be closed for an estimated period of 1-2 hours. The crew considered using runway 36 but calculations showed that it would be unacceptable. After calculating the aircraft's endurance, the crew decided to divert to Tindal. Both pilots subsequently reported that at the time of the diversion they believed that the accident aircraft was at about the midway point of runway 11/29.
When the aircraft arrived at Tindal the surface movement controller passed a message to the crew from RAAF Darwin, advising that runway 11 now had an available length of 5,500 ft, but with a landing over a displaced threshold and the accident aircraft. Runway 29 was also available with a 15kt downwind component.
RAAF Darwin ATC had advised RAAF Tindal ATC that runway 11 had a landing distance available (LDA) of 1,936 m and a take-off run available (TORA) of 2,036 m. This message was to be passed to the crew of VH-TJV after its arrival at Tindal. The RAAF flight planning officer, who received the message, wrote the LDA and TORA down on a piece of notepad paper and personally delivered it to the aircraft, handing it to the pilot in command. He believed he had advised the pilot in command of the displaced threshold and that the landing would be over the disabled aircraft. The pilot in command remembered being given the handwritten message but stated that he had not been given any information other than the LDA and TORA.
After arranging for the aircraft refuelling and passenger requirements, the pilot in command contacted the company's Operations Department by telephone to report arrival at Tindal, and to arrange for another flight plan to be issued for the Tindal - Darwin sector. A short time later he called Operations again and was transferred to a dispatcher who arranged the flight plan issue. The pilot in command advised that he did not require another copy of the weather as the information he had was still valid. The dispatcher assumed that since the pilot in command was in the area, and aware of the problem in Darwin, there was no need to send the NOTAM concerning the displaced threshold as this would mean transmitting all the Darwin NOTAM pages, therefore only the flight plan was sent.
VH-TJV departed Tindal for Darwin at approximately 1550 CST.
During approach to Darwin the co-pilot obtained the following landing information from the Automatic Terminal
Information Service (ATIS):"Information Juliet, runway 11, displaced threshold, 36, wind 060/10-15, QNH 1009, 29.80, temperature 32, CAVOK, runway 11 LDA 1,936 m, TORA 2,036 m, pedestrians and vehicles operating in the undershoot". The co-pilot annotated the relevant information onto the landing data card, then showed it to the pilot in command who had also been monitoring the ATIS while communicating with ATC. The pilot in command acknowledged but did not confirm the information as required by company policy. Neither pilot could recall noticing the information concerning the displaced threshold.
When the aircraft was on final for runway 11, ATC again advised of the displaced threshold and instructed the crew to report sighting the displaced threshold markers. Then, after a pause of several seconds, the controller advised that the visual approach slope indicator system (VASI) was turned off. The crew subsequently reported that they did not hear the reference to the requirement to sight the markers although they did note that the VASI was not available. ATC did not prompt the crew when they had not reported sighting the displaced threshold markers.
As a precautionary measure when aircraft were landing, all vehicles and personnel were removed from the undershoot area. Only personnel working on the disabled aircraft remained in position.
Although the weather was fine and clear, the crew reported that from the air there was a certain amount of haze and sun glare which made objects on the ground appear to blend into their surroundingsThey advised that during the approach they were concentrating on maintaining the correct speed and profile to arrive as close as possible to the threshold in order to utilise all of the available runway length, and did not see the white runway unserviceable crosses located in the undershoot area.
The controllers reported that when they noticed the aircraft on short final, about 150-200 ft above ground level (AGL), it appeared about to land in the undershoot area. The controllers believed that RAAF policy precluded turbo-jet aircraft from going around below 200 ft AGL due to slow engine response time, and therefore considered it safer to allow the aircraft to continue. The crew's first awareness of landing in the undershoot area was when the aircraft passed over one of the white crosses.
The information supplied to the crew by ATC prior to their diversion to Tindal concerning the location of the disabled aircraft, and the available runway length situation, appeared to have allowed both pilots to develop a mindset that the western end of runway 11, that is the normal threshold, was the serviceable area.
The airport operator, who had arranged the displaced threshold, advised that all markings were in accordance with the Rules and Practices for Aerodromes (RPA) standards. The temporarily displaced threshold was marked with Vee-Bars, and the white crosses in the undershoot area were twice the standard size, i.e. 12 m x 0.9 m. RPAs also require runway threshold identification lights (RTIL) to be in place, marking a displaced threshold at aerodromes serving international regular public transport jet aircraft, e.g. Darwin. These lights were not available.
Prior to the occurrence the pilot in command had been rostered for two days on reserve duty, preceded by one day off, and the co-pilot had been off duty for three days. They had completed a 10-hour tour of duty, having flown four sectors including the diversion.
Since 1981 there have been 25 reported occurrences of pilots failing to see runway displaced threshold or unserviceable markings, six occurring since 1990. Anecdotal evidence suggests that this figure may be much higher. In many cases poor contrast of the markings with the surrounding surface may have been the problem.
SIGNIFICANT FACTORS
Information flow available for the crew at the Tindal diversion point was inadequate.
Information provided to the crew by RAAF Tindal was inadequate.
The company flight dispatcher failed to provide a hard copy of the NOTAM to the crew.
The Darwin ATIS was misleading; however, enough information was available for the crew to seek clarification.
The co-pilot did not take note of the ATIS comments about the displaced threshold, and the pilot in command, contrary to company policy, did not confirm the ATIS information.
The crew developed a mindset regarding the serviceable runway and the disabled aircraft location, and did not clarify information available to them.
ATC did not verify that the crew understood the instruction to sight the displaced threshold markers.
ATC did not issue go-around instructions.
Light conditions may have made the runway displaced threshold markings difficult to see.
SAFETY ACTION
The Bureau of Air Safety Investigation issued interim recommendation IR950176 to the Civil Aviation Safety Authority.
"The Bureau of Air Safety Investigation recommends that the Civil Aviation Safety Authority:
"(i) review "runway displaced threshold" and "runway unserviceable" markings to improve the visibility to pilots under all conditions. This review should consider the use of different colours, shapes and backgrounds to increase the contrast and distinguishability of such runway markings; and
"(ii) ensure that airport owners and operators have the correct portable runway lighting available for identifying unserviceable areas of the runway where required."
The following response was received from the Civil Aviation Safety Authority on 17 October 1995:
"I refer to Interim Recommendation IR950176 concerning the displaced threshold incident involving a Boeing 737, VH-TJV, at Darwin on 7 June 1995.
"Summary
"(i) The Authority has no plans to review the standards for runway displaced threshold and runway unserviceable.
"(ii) Work is currently being undertaken on the production of a Civil Aviation Order on Aerodrome Lighting. "Background to Response
"Displaced Threshold and Unserviceability markings depicted in Rules and Practices for Aerodromes, Chapters 11 and 20, are consistent with ICAO standards and recommended practices. The Authority has no plans to review these standards.
"Work is currently being undertaken on the production of a CAO on Aerodrome Lighting which will include the standards for displaced threshold lighting and temporary runway end lighting. It is considered that, in the interim, the requirements of the lighting section of the Rules and Practices for Aerodromes is an adequate and acceptable standard. It is not anticipated that these requirements will be changed significantly with the making of the CAO."