On 29 May 2006 at about 0805 Eastern Standard Time, a Boeing Company 737-7Q8 aircraft (737) passed within 400 ft vertically of an Aero Commander 680-FL (Aero Commander) aircraft. At that time there was less than the minimum 3 NM radar separation standard or the 1,000 ft vertical separation standard between the two aircraft.
The 737 departed Melbourne Airport tracking to the north and then to the north-east of Melbourne on a runway 27 DOSEL 3 standard instrument departure (SID). The Aero Commander became airborne off runway 35 at Essendon. The pilot of the Aero Commander was instructed to track overhead Melbourne Airport and climb to 3,000 ft. From overhead Melbourne Airport, the pilot was instructed to fly a heading of 310 degrees magnetic.
The pilot of the Aero Commander advised the departures controller that he had the 737 in sight. However, there was a breakdown of separation standards because the departures controller did not comply with the requirements of the Manual of Air Traffic Services (MATS) when he assigned separation responsibility to the pilot of the Aero Commander.
On 25 January 2006, a Boeing Company 777-200 (777) was en route from Christchurch, NZ, to Singapore at flight level (FL) 360. A Boeing Company 737-838 (737) was en route from Alice Springs, NT, to Sydney, NSW, on a reciprocal track at FL370. At 0422.30 Coordinated Universal Time the two aircraft passed each other in the vicinity of waypoint APOMA, in the Melbourne Flight Information Region.
The pilots of the 777 had requested a clearance to climb to FL380. The separation standard that was applicable between the two aircraft, before the air traffic controller could authorise climb for the 777, was a ten minute longitudinal standard. That standard required the controller to calculate the estimated time the two aircraft would pass, using a method approved in the Manual of Air Traffic Services. Once that estimated time of passing was established, ten minutes either prior to, or after, that time of passing had to be applied. In the circumstances, a vertical separation standard needed to exist from the estimated time of passing plus the ten minutes. The crew of the 777 had been instructed to climb to FL380 at the estimated time of passing plus 8.5 minutes. There was an infringement of separation standards.
The air traffic controller's initial scan of the air situation display was incomplete and did not detect that a procedural separation standard would not exist between the 737 and the 777, or that he needed to calculate the time that the 10 minute longitudinal separation standard was established. A more comprehensive initial scan of the air situation display by the controller may have facilitated timely action to avoid an infringement of separation standards.
The information provided to the Alice Springs aerodrome controller, from both the pilot of the C310 and the crew of the 717, indicated that a lateral separation standard existed between the aircraft. On that basis, the aerodrome controller cleared the crew of the 717 to descend below the level of the C310. However, the position of the Cessna C310 relative to the 717, as reported by the 717 crew, at the time the aerodrome controller cleared the 717 crew to descend through the level of the C310, meant that no procedural separation standard existed between the two aircraft. The aerodrome controller had no indication that the information from either source may have been erroneous, before clearing the 717 to descend through the level of the C310. It was not possible for the investigation to determine why the lateral separation standard applied by the aerodrome controller was compromised.
The integrity of procedural separation standards relies on the accuracy of information provided to air traffic control by pilots. Once the pilot of the C310 reported that the aircraft was established in the training area, the aerodrome controller had established a lateral separation standard between the C310 and the 717. He was then able to clear the 717 to descend through the level of the C310. Pilots need to be mindful of the importance of the accuracy of the information they provide to air traffic control in maintaining the integrity of published separation standards.
Factual Information
On 17 November 2005, at 1327 Central Standard Time, a Boeing Company 717-200 (717) aircraft, registered VH-NXE, was inbound to Alice Springs, NT, on the 055 degree radial of the very high frequency omni-directional radio range (VOR) ground-based navigation aid, on a scheduled flight from Cairns, Qld. The 717 crew reported to the Alice Springs aerodrome controller that they passed almost overhead and within about 1,500 ft of a Cessna Aircraft Company C310R (C310) that was outbound from Alice Springs.
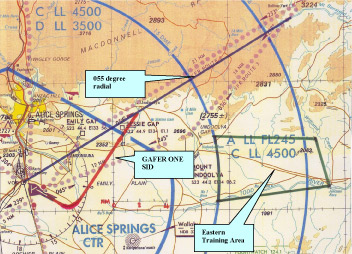
The C310, registered VH-JOI, was being operated on a pilot instrument rating renewal flight and, after becoming airborne off runway 12, was being tracked via a GAFER ONE standard instrument departure (SID), on climb to operate in a training area located to the east of Alice Springs (Figure 1), not above 6,000 ft. A SID is a published instrument flight rules departure comprising obstacle clearance data to the minimum safe altitude and tracking data until the aircraft reaches a specified point on its air traffic control cleared route. The GAFER ONE SID provided altitude requirements and heading instructions that enabled the pilot to intercept the 055 degree radial from the VOR.
Figure 1: Alice Springs visual terminal chart showing the 055 degree radial, the approximate track of the GAFER ONE standard instrument departure and the Eastern Training Area
The approved testing officer, who was also the pilot in command on board the C310, later reported that when the aircraft was at about 15 NM from Alice Springs, the pilot being tested turned the aircraft right, off the 055 degree radial of the VOR, and tracked towards the training area.
The Alice Springs airspace was not serviced by radar and as such the Alice Springs aerodrome controller was required to apply non-radar (procedural) control, in accordance with published procedures. The aerodrome controller was responsible for controlling aircraft operating within the Alice Springs control zone and control area up to 8,500 ft. Procedural control is achieved by the use of information from sources other than radar. The aerodrome controller intended to establish a lateral separation standard between the C310 and the inbound 717 once the C310 was established in the training area.
The aerodrome controller initially applied a vertical separation standard of 1,000 ft between the C310 and the 717. At 1326, the pilot of the C310 reported, to the aerodrome controller, that the C310 was established in the training area to the east of Alice Springs. That training area was procedurally separated, using a lateral separation standard, from the 055 degree radial from the Alice Springs VOR. Once the pilot of the C310 reported established in that training area, the C310 was laterally separated from the 717. The aerodrome controller then cleared the crew of the 717 to descend below the altitude of the C310.
About a minute later, the crew of the 717 reported that they had the C310 in sight about 1,500 ft below their aircraft. The pilot in command of the C310 later reported that he heard that broadcast made by the crew of the 717, but despite conducting a search for the 717, did not see the aircraft.
Summary
On 17 November 2005, a Boeing 717-200 (717) aircraft departed Cairns, Qld, on a scheduled flight to Alice Springs, N.T. It reportedly passed within 1 NM horizontally and 1,500 ft vertically of a Cessna Aircraft Company C310R (C310) aircraft that was outbound from Alice Springs, NT, on an instrument flight rules (IFR) training flight.
The information provided to the Alice Springs aerodrome controller indicated that a lateral separation standard existed between the aircraft. On that basis, the aerodrome controller cleared the crew of the 717 to descend below the level of the C310. However, the position of the Cessna C310 relative to the 717 at the time the aerodrome controller cleared the 717 to descend through the level of the C310 meant that no procedural separation standard existed between the two aircraft. The aerodrome controller had no indication that the information from either source may have been erroneous.
Alice Springs airspace is not serviced by radar, and there was no recorded information on board either aircraft that could be used to determine the exact proximity between the two aircraft at their closest point. It was not possible for the investigation to determine why the lateral separation standard applied by the aerodrome controller was compromised.
Pilots should be mindful of the importance of the accuracy of the information they provide to air traffic control, in maintaining the integrity of published separation standards.
On 3 November 2005, the aerodrome controller (ADC) at Gold Coast Airport, Qld issued the crew of a Boeing 717 (717) aircraft a take-off clearance following closely behind an Airbus A320 (A320) aircraft. The ADC was responsible for the initial visual separation between the two aircraft and also for providing a suitable separation standard for the Brisbane approach controller who was responsible for the overlying airspace. While the ADC was able to continue to visually separate the two aircraft after departure, he was not able to communicate this or arrange another standard, with the approach controller. The two aircraft entered the approach controller's airspace with less than the required radar separation standard and the approach controller took action by initiating a significant change in heading for the 717. There was a breakdown of co-ordination.
The pilot in command of the 717 later reported that the crew had considered the distance behind the A320 to be safe for their departure, and that the crew maintained visual contact with the A320 throughout the takeoff, departure and subsequent tracking.
Documentation available to both controllers provided guidance relating to coordination phraseology and separation responsibilities. The attempted coordination exchange did not adhere to the requirements of these documents and was continuously interrupted as a result of the workload of both controllers. The incident highlighted the need for controllers to use clear unambiguous words and phrases to ensure complete understanding of all communications, including coordination exchanges. It also highlighted the importance of tactical separation assurance which places emphasis on traffic planning and conflict avoidance, rather than conflict resolution.
As both the ADC and the crew of the 717 had continuous visual contact with the two aircraft it was unlikely that the situation would have resulted in the aircraft coming into such close proximity as to have presented any significant safety risk.
As a result of this incident, the operator issued a course deviation indicator (CDI) setting standing order. That order included the instruction that if a crew receives an assigned heading from air traffic control, prior to take-off, the Electronic Horizontal Situation Indicator CDI was to be set to that heading.
The operator also issued an inter-crew communications standing order that included a requirement for the pilot not flying to call 'approaching heading' within 15 degrees of an assigned heading following the initial turn after takeoff. The order also stated that:
As a general rule in multi crew operations any ATC or other internal critical instructions need to be read back amongst the crew to ensure that the instruction has been acknowledged and understood.
Analysis
The pilots of the Saab were instructed by air traffic control to depart Townsville on a heading of 350 degrees magnetic, to ensure a lateral separation standard existed between the Saab and the arriving Cessna 310. However, on departure, the pilots of the Saab continued their left turn, through the assigned heading. That reduced the lateral separation between the Saab and the inbound Cessna and resulted in an infringement of separation standards. This analysis examines the development of the occurrence and highlights the safety issues that became evident as a result of the investigation.
Despite a correct readback to the controller and recording the assigned heading on the Takeoff and Landing Data Card, the copilot forgot about the heading instruction as he commenced the turn after takeoff. The pilot's familiarity with the visual departures to the west, and his expectation of a visual departure on this occasion, may have contributed to the occurrence.
A person's capacity to remember to perform a task in the future can be adversely affected by workload, distraction, lack of mindfulness because of familiarity, and the elapsed time between any instruction and the proposed activity. Although the sterile cockpit policy practiced by the crew reduced the risk of distractions, the takeoff necessarily involved a high workload and there was a period of elapsed time between the assignment of the heading and initiation of the turn. Application of a cue such as setting the assigned heading on the EHSI heading selector or on the course deviation indicator would reduce the risk of flight crew forgetting assigned headings.
Monitoring by the pilot not flying is a means of early identification of heading deviations. In this case, the pilot in command was busy adjusting the power levers and did not immediately realise that the aircraft's heading had diverged from the assigned heading. Although the pilot not flying has a number of actions to perform during a departure, monitoring critical phases of the flight should be a high priority.
The controller's plan for separating the Saab and Cessna was based on establishing a lateral separation standard based on the Saab's assigned heading of 350 degrees and the Cessna's inbound radial of 329 degrees. The aerodrome controller and approach controller both became aware that the Saab had turned through the assigned heading, but were initially uncertain of the crew's intentions. It was a dynamic situation and the approach controller attempted to mitigate the effect of the Saab's displaced departure track by alerting the Cessna pilot to the proximity of the Saab and instructing him to conduct an orbit.
Although there was an infringement of separation standards, the Cessna's orbit delayed the closest point of approach, allowing time for the Saab to climb, which increased the vertical distance between the two aircraft as they passed. The left orbit would have been more effective had the Saab continued onto the flight planned track. However, there was little time for the approach controller to establish radio contact and ascertain the crew's intentions before the Saab crew turned their aircraft back to a heading of 350 degrees and passed almost overhead the Cessna with about 500 ft vertical separation between them.
The Traffic Alert Collision Avoidance System (TCAS) alerted the Saab crew to the proximity of the Cessna and reduced the risk of collision.
Factual Information
Sequence of events
On 13 October 2005 at 0618 Eastern Standard Time, a Saab Aircraft AB 340B (Saab), registered VH-UYA, departing Townsville Airport, Qld, came within the minimum separation standard of 1,000 ft vertically and of 3 NM horizontally of an inbound Cessna Aircraft Company 310R (Cessna), registered VH-TFP. There was an infringement of air traffic control separation standards.
The crew of the Saab was operating a scheduled passenger flight to Trepell, in central Queensland, in accordance with the instrument flight rules. Air traffic control issued a clearance to the crew to track via waypoint CATEY, a track of 243 degrees magnetic from Townsville. At 0611, the crew taxied for runway 01 1. After the crew reported ready for departure, the aerodrome controller issued the crew with a departure clearance, including an instruction to turn left, heading 350 degrees, visual. The pilot in command confirmed the instruction with the copilot. The copilot, who was the pilot flying, then read back the clearance to the aerodrome controller. Both pilots reported that the departure clearance was written on the Take-off and Landing Data Card before completing the pre-take-off checks and commencing the take-off roll.
Recorded information showed that as the Saab was rolling, the Cessna was 9 NM from Townsville, inbound from Cairns, Queensland on the 329 radial, and was on descent to 1,800 ft.
When the Saab had reached an altitude of between 600 and 700 ft the copilot commenced a left turn, engaged the autopilot, and selected a heading of about 210 degrees to intercept the planned outbound track of 243 degrees. At about 1,000 ft the pilot in command, as the pilot not flying, set the power levers to climb power. During the turn, at a heading of about 290 degrees, the pilot in command realised that they had flown through the assigned heading and alerted the copilot. The copilot reported that at about the same time he also realised they had flown through the assigned heading. He disengaged the autopilot and quickly turned the aircraft to the right onto the assigned heading of 350 degrees. During the turn, the Saab's Traffic Alert and Collision Avoidance System (TCAS) produced a traffic advisory (TA) consisting of an aural alert of 'traffic traffic' and the crew observed an amber symbol on the TCAS display that was indicating traffic below them. The crew attempted to sight the traffic but were unsuccessful. The pilot in command advised the approach controller that they were turning onto 350 degrees.
Both the approach controller and the aerodrome controller noticed that the Saab appeared to be turning as if to intercept the flight planned 243 radial. The aerodrome controller attempted to contact the Saab crew however, at that time the crew were in the process of transferring to the approach frequency and had not yet established contact. The approach controller provided traffic information to the pilot of the Cessna and when the pilot reported that he had not sighted the Saab, the approach controller instructed him to make a left orbit. The Saab crew subsequently contacted the approach controller and advised that they were turning onto a heading of 350 degrees visual, passing 2,200 ft. The approach controller passed updated traffic information to the Cessna pilot who then sighted the Saab about 500 ft above him and 0.5 NM ahead.
Recorded radar information indicated that when the horizontal distance reduced to approximately 3 NM between the closing aircraft, there was 400 ft vertical separation, and the Saab subsequently flew about 500 ft directly over the Cessna.
Operational aspects
Prior to engine start, the Saab crew set the Electronic Horizontal Situation Indicator (EHSI) heading selectors to the runway heading and the course deviation indicators to the outbound track of 243 degrees.
The operator did not require any change to the EHSI heading selectors or course deviation indicators in response to heading assignments in departure clearances. The operator required pilots to set the EHSI heading selector to runway heading in readiness for a one engine inoperative situation. It was common practice for the operator's crews to confirm a departure clearance with each other before it was written down and read back to the controller.
The pilot in command indicated that, as the pilot not flying, he monitored the conduct of the flight. However, there was no specific operator requirement for the pilot not flying to monitor the turn and ensure that the pilot flying captured assigned headings.
The Saab crew reported that they were observing the 'sterile cockpit' policy specified in the operator's aircraft operating manual. That policy prohibited discussion about anything except the immediate operation of the aircraft while an aircraft was climbing or descending below 10,000 ft. They indicated that their workload was normal and that they were not rushing. The copilot considered that he was not tired and there was no apparent reason for him forgetting about the assigned heading. He also said that most of the Saab operations from Townsville involved visual departures to the west and the assignment of radar headings with departure clearances was unusual.
The TCAS fitted to the Saab provided aural and visual traffic advisories when an aircraft equipped with a functioning transponder was within about 45 seconds of the projected closest point of approach. When an aircraft was within approximately 30 seconds of the closest point of approach, the TCAS issued aural and visual resolution advisories. The operator's requirements for crew response to a TCAS traffic advisory was: 'Conduct a visual search for the intruder. If successful, maintain visual acquisition to ensure safe separation.'
The weather conditions were reported to be a light wind with greater than 10 km visibility and 1 to 2 eighths cloud coverage at 2,000 ft.
Runway 01 heading is 016 degrees M.
Summary
On 13 October 2005, at 0618 Eastern Standard Time, a Saab Aircraft AB 340B (Saab), registered VH-UYA, departing Townsville Airport, Queensland, came within the minimum separation standard of 1,000 ft vertically and of 3 NM horizontally of an inbound Cessna Aircraft Company 310R (Cessna), registered VH-TFP. There was an infringement of air traffic control separation standards.
The pilots of the Saab were instructed by air traffic control to depart Townsville on a heading of 350 degrees magnetic, to ensure a lateral separation standard existed between the Saab and the arriving Cessna. However, on departure the pilots of the Saab continued their left turn through the assigned heading, before turning their aircraft back to a heading of 350 degrees. The approach controller provided traffic information to the pilot of the Cessna and when the pilot reported that he had not sighted the Saab, the approach controller instructed him to make a left orbit. The Saab passed almost overhead the Cessna with about 500 ft vertical separation between them.
Despite a correct readback to the controller and recording the assigned heading on the take-off and landing data card, the Saab copilot forgot about the heading instruction as he commenced the turn after take-off. The pilot in command, as the pilot not flying, intended to monitor the conduct of the flight but was busy adjusting the power levers and did not immediately realise that the aircraft's heading had diverged from the assigned heading.
Following the occurrence the operator of the Saab issued two standing orders.
On 31 August 2005, the crew of a Fairchild Industries Inc SA227–DC (Metro) aircraft had been issued a clearance for a visual approach to runway 14 at Brisbane Airport. At about the same time, the crew of a Boeing Company 717–200 (717) aircraft had been issued a take-off clearance from runway 01. The crew of the Metro commenced a go-around from runway 14 at about the same time the 717 became airborne from runway 01. The 717 crossed about 625 m in front of, and 580 ft above, the Metro. There was a breakdown of separation.
The Metro’s descent to Brisbane had been restricted by another aircraft, which placed it above the normal descent profile. The crew of the Metro subsequently continued an approach that was unlikely to be conducted successfully. The aerodrome controller misjudged the position of the Metro, which resulted in the incorrect application of separation standards. This also meant that the controller did not give adequate consideration to the likelihood of a go-around by the crew of the Metro.
After the Metro crew commenced the go-around, the controller was unable to visually separate the aircraft. The controller had not provided traffic information to the crew of either aircraft, nor was he required to do so. The controller attempted to make the Metro crew aware of the 717, but did not provide the information in the form of a safety alert as required by the Manual of Air Traffic Services.
Without prior knowledge of the 717, the crew of the Metro found it difficult to identify the correct aircraft, as the 717 was initially below their level and masked by background lighting.
As a result of previous occurrences, the ATSB had previously issued a safety recommendation to Airservices Australia in October 2006 in relation to the provision of relevant traffic information, to enhance pilot situational awareness.
On 25 June 2005, a Bombardier Aerospace Dash 8-315 (Dash 8) aircraft was being operated on a scheduled passenger service from Weipa to Cairns, Qld, while three Aero Commander Div Shrike Commander aircraft (Aero commander) were tracking to Cairns from Cooktown, Qld. The four aircraft were in an arrival sequence of seven aircraft tracking to runway 15. Visual meteorological conditions existed during the period of the aircrafts' arrivals.
Based on the aircrafts' estimated arrival time, the Dash 8 was 3 minutes behind the three Aero commanders. The Aero commanders were maintaining 1,000 ft above mean sea level, and the Dash 8 was on descent from 5,000 ft. The Cairns approach controller estimated that low level headwinds would delay the Aero commanders more than the Dash 8. Consequently, the controller re-ordered the landing sequence to place the Dash 8 ahead of the Aero commanders for landing. The approach controller notified the aerodrome controller of the change in the landing sequence.
At 1705 Eastern Standard Time, when the Dash 8 was on final approach at about 6 nautical miles1 (NM) from the airport, the crew received a traffic alert and collision avoidance system (TCAS) traffic advisory. The crew saw an Aero commander to the left at about 3 NM, and observed on the TCAS display another aircraft in close proximity. Very shortly after, they received a TCAS resolution advisory to climb their aircraft, which they followed. The crew reported that as they were climbing, they saw an Aero commander pass to the left of the Dash 8.
The four aircraft were being operated on instrument flight rules category flights that required separation by air traffic control. Controllers could use a 3 NM radar separation standard, a vertical separation standard of 1,000 ft, visual separation by the aerodrome controller, or require a pilot to sight and follow another aircraft. The approach controller's intention was to separate the aircraft using sight and follow procedures.
As the aircraft approached the airport the aerodrome controller used non-standard coordination phraseology that was misunderstood by the approach controller. The approach controller subsequently instructed the crew of the Dash 8 and the three Aero commanders to transfer to the aerodrome controller's radio frequency. The resultant traffic situation presented to the aerodrome controller was difficult to resolve using visual separation or sight and follow procedures.
The TCAS events occurred as the first Aero commander turned right to track behind the Dash 8 on the final approach to runway 15. The Aero commanders were from the same operator and often used sight and follow procedures between company aircraft on arrival.
An Airservices Australia (Airservices) investigation found that the occurrence was due to the following factors:
the approach controller made an error of judgement in assessing the new traffic sequence
the aerodrome controller used non-standard coordination phraseology that was misinterpreted by the approach controller
the use of sight and follow procedures for the number of aircraft involved increased controller workload
the approach controller's lack of recent familiarisation with tower visual separation procedures.
The Airservices report made six recommendations, and the following action has been taken in regard to the recommendations:
tower and approach/departure controllers were reminded to use standard coordination phraseology to reduce the possibility of ambiguity
a tower and approach/departure area familiarisation program has been implemented that requires participating controllers to complete a project paper
letters of agreement regarding sight and follow procedures have been finalised with two local operators.
A nautical mile is equal to 1852 metres.
Summary
On 25 June 2005, a Bombardier Aerospace Dash 8-315 (Dash 8) aircraft and three Aero Commander Div Shrike Commander aircraft (Aero commander) were in an arrival sequence of seven aircraft to runway 15 at Cairns Airport. At 1705 Eastern Standard Time, when the Dash 8 was on final approach at about 6 nautical miles (NM) from the airport, the crew received a traffic alert and collision avoidance system (TCAS) traffic advisory. The crew saw an Aero commander to the left at about 3 NM, and observed on the TCAS display an aircraft in close proximity. Very shortly after, the crew of the Dash 8 received a TCAS resolution advisory to climb their aircraft, which they followed. The crew reported as they were climbing, they saw a second Aero commander pass to the left of the Dash 8.
An Airservices Australia (Airservices) investigation of the occurrence found that the occurrence was due to the following factors:
the approach controller made an error of judgement in assessing the new traffic sequence
the aerodrome controller used non-standard coordination phraseology that was misinterpreted by the approach controller
the use of sight and follow procedures for the number of aircraft involved increased controller workload
the approach controller's lack of recent familiarisation with tower visual separation procedures.
The Airservices report made four recommendations to Cairns Terminal and two recommendations to Cairns Tower, for action.
The post implementation review by Airservices Australia of the June 2003 review of breakdown of separation occurrences found that since the recommendations were implemented, errors in either building or maintaining situational awareness by the controllers involved had reduced to 44 percent of occurrences involving infringements of separation standards.
Analysis
In this occurrence, the controller did not perceive the potential conflict between the aircraft, despite previous refresher training that should have assisted in the task.
Although the presence of the supervisor in the operations room created an opportunity to discuss an operational issue, it was not a priority. The controller should have discussed the issue at some other time when he was not responsible for an operational position. The supervisor was also in a position to defer the discussion with the controller, until a more suitable time or location, which would have reduced the likelihood of compromising operations.
While distraction could not be discounted as a contributing factor, the circumstances of the occurrence are consistent with the findings of the Airservices Australia June 2003 review, particularly with respect to low levels of situational awareness by controllers. Over time, the benefits of the implementation of the review recommendations in helping to develop controller awareness of potential performance limitations should become apparent.
Summary
On 19 April 2005 at about 1522 Eastern Standard Time, a Boeing Company 747-422 (747) aircraft was en route from Sydney, NSW, to Los Angeles, USA, on climb to flight level (FL) 310 and a de Havilland Dash 8 (Dash) aircraft was en route from Lord Howe Island to Sydney, maintaining FL240. The crew of the Dash had been issued with a clearance to descend to 10,000 ft above mean sea level. The intended tracks of the aircraft intersected at a point about 90 NM east of Sydney.
The aircraft were under radar control by the Brisbane Centre Ocean sector controller. The Australian Advanced Air Traffic System (TAAATS) assessed the two aircraft as potentially being in conflict and activated the short-term conflict alert (STCA) on the air situation display. Following activation of the STCA, the Ocean controller saw that the aircraft were about 16 NM apart and instructed both crews to turn their respective aircraft left in an endeavour to maintain the minimum radar separation standard of 5 NM. Analysis of recorded data from TAAATS showed that the aircraft passed with 4.1 NM lateral and 400 ft vertical spacing. The required minimum vertical separation standard was 1,000 ft. There was an infringement of separation standards.
The controller had been operating in the position for about 50 minutes prior to the occurrence. The level of complexity within the sector was reported to be light to moderate. The controller reported that despite reviewing the aircraft's tracks he expected the track of the 747 to be northwest of the inbound track of the Dash 8. Immediately prior to the activation of the STCA the controller was not monitoring the aircraft situation display as he was discussing operational coordination issues with an operational supervisor, who was consulting a chart located near the Ocean sector console position. The controller had initiated the discussion with the supervisor to follow up previous correspondence on the issue.
A review of breakdown of separation occurrences, conducted by Airservices Australia in June 2003, found that 92 percent of en route sector infringements of separation standards involved an error in either building or maintaining situational awareness by the controllers involved. The review made 31 recommendations and Airservices Australia has implemented all the recommendations of the review.
Since July 2003, the controller had undergone refresher training that included compromised separation (February 2004), separation assurance (February 2004), human factors awareness (March 2005) and situational awareness (March 2005).
Occurrence summary
Investigation number
200501720
Occurrence date
19/04/2005
Location
167 km E Sydney, (VOR)
State
New South Wales
Report release date
13/09/2005
Report status
Final
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Loss of separation
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
De Havilland Canada/De Havilland Aircraft of Canada
On 9 April 2005 at about 0815 universal coordinated time, the Transport Accident Investigation Commission (TAIC) of New Zealand notified the Australian Transport Safety Bureau (ATSB) of an air safety occurrence involving an Australian-registered and operated aircraft, which occurred earlier that evening near Auckland International Airport. The ATSB appointed an accredited representative to participate in the investigation into the occurrence, in accordance with clause 5.18 1 of Annex 13 to the Convention on International Civil Aviation. To protect the information supplied by TAIC to the ATSB and investigative work undertaken to assist TAIC, the ATSB initiated an investigation under the Transport Safety Investigation Act 2003. The report presented below was prepared principally from information supplied to the ATSB.
FACTUAL INFORMATION
The occurrence involved a Boeing Company B747-338 (747) aircraft, registered VH-EBW, with a crew of 16 and 346 passengers, which was being operated on a scheduled passenger service between Sydney, Australia, and Auckland, New Zealand. The copilot was the handling pilot for the flight.
As the 747 was on the landing approach to runway 23 right (23R) at Auckland, the Auckland Tower and Terminal controllers observed an unidentified aircraft tracking towards the approach path of the 747. The controllers instructed the crew of the 747 to discontinue the approach, and turn the aircraft right towards the central city area, and to climb to 3000 ft. The aircraft subsequently entered instrument meteorological conditions (IMC) at an altitude of 3,000 ft above mean seal level (AMSL). The flight crew reported that shortly after, and while still in IMC, they received a TERRAIN, PULL-UP warning from the aircrafts enhanced ground proximity warning system (EGPWS). The pilot in command took control of the aircraft and commenced an immediate climb in accordance with the operators 747 procedures. The crew advised air traffic control that they had received a GPWS terrain warning, and that they were climbing the aircraft to 5,000 ft AMSL.
At the same time, a New Zealand-registered 747 was making an instrument approach to runway 23R, and had been cleared to descend to an altitude of 4,000 ft AMSL. As the Australian-registered 747 was climbing to 5,000 ft AMSL, it passed about 1.9 NM behind the New Zealand-registered 747, which was descending through 4,500 ft AMSL. The required separation standard was 3 NM laterally or 1,000 ft vertically. There was an infringement of the required separation standard. No avoiding action was taken, or was required to be taken, by either crew.
The TAIC is the independent New Zealand government entity responsible for no blame safety investigation of accidents and incidents in New Zealand. The Australian accredited representatives role in the investigation has been to provide the TAIC with information about the aircraft and its operation, recorded flight data recovered from the aircraft flight data recorders, crew details, and records of discussions taken during separate interviews conducted with the pilot in command and the copilot of the Australian-registered 747. The TAIC expects to complete the investigation into this occurrence by October 2005, and will publish the final report on its website at www.taic.org.nz.
1Clause 5.18 - The State of Registry, the State of the Operator, the State of Design and the State of Manufacture shall be entitled to appoint an accredited representative to participate in the investigation.
As a result of this occurrence, Airservices Australia proposed the following system improvements:
Brisbane approach training packages to be revised to incorporate runway 14/32 scenarios in future training modules
Examine options for including additional content on tower visual separation procedures into Brisbane approach training modules
Routine performance assessments for Brisbane approach controllers to formally assess knowledge of reciprocal runway procedures.
At the time of writing this report, the Bureau had not received advice from Airservices Australia regarding the status of these proposals. On 20 December 2005, Airservices Australia advised the ATSB of the following safety actions:
Knowledge of reciprocal runway operations is tested during assessments.
Tower controllers have completed familiarisation periods in approach.
Analysis
ANALYSIS
Introduction
Although there was no specified minimum distance standard for visual separation in these circumstances, the aerodrome controller was unable to continue to apply a visual separation standard, in azimuth, between the 737 and the Aero Commander. This analysis examines the development of the occurrence and highlights the safety issues that became evident as a result of the investigation.
Noise abatement procedures
Airspace restrictions imposed by the noise abatement procedures in force at the time of the occurrence resulted in limited options available to either the aerodrome controller or the approach controller to separate the departing Aero Commander with the inbound aircraft. The approach controller determined that he would be unable to establish and maintain a separation standard between the two aircraft and comply with noise abatement procedures, and so relied on the aerodrome controller to separate the two aircraft using visual separation.
The requirement for pilots to request a start clearance would normally provide the aerodrome controller with an opportunity to assess the traffic situation, in light of airspace limitations associated with noise abatement procedures, so that any delays can be absorbed prior to the aircraft's engines being started. A heading of 360 degrees was an appropriate heading in the circumstances. It would also have complied with noise abatement procedures and facilitated the application of visual separation in azimuth.
Controllers cannot be held responsible for delays to departing aircraft as a result of noise abatement procedures. Controllers are required to take such restrictions into account in their normal decision-making processes. The noise abatement procedures themselves were not considered to have contributed significantly to this occurrence.
Air traffic control separation standards and procedures
The converging tracks of the two aircraft precluded the aerodrome controller from ensuring that visual separation, in azimuth, was not infringed.
The low light conditions at that time of day and the cloud cover, may have made it difficult for the aerodrome controller to visually determine the departure track of the Aero Commander. Reference to the tower radar display was authorised by the Manual of Air Traffic Services (MATS) and would have clearly indicated the Aero Commander's track. Had the aerodrome controller referred to the tower radar display earlier, he may have been able to take action in sufficient time to ensure that separation was not infringed.
The situation which arose, where the aerodrome controller was separating the aircraft while the aircraft were not on the aerodrome control frequency, was not consistent with the letter of agreement. However, it did enable the approach controller to provide mutual traffic information to the pilots of both aircraft. That increased the awareness of the 737 crew of the presence of the Aero Commander and assisted the pilot of the Aero Commander to see the 737.
Although it would have been difficult for the aerodrome controller to separate the departing Aero Commander on a heading of 090 degrees, with arriving aircraft on the final approach path for runway 19, the aerodrome controller accepted those instructions and confirmed that he could separate in those circumstances. On that basis, the approach controller authorised the departure. The approach controller coordinated the departure instructions with the aerodrome controller in accordance with the letter of agreement. The approach controller confirmed, on a number of occasions, that the aerodrome controller had accepted responsibility for separating the Aero Commander on a heading of 090 degrees. The approach controller had no way of knowing that the aerodrome controller had misunderstood the instruction.
From the aerodrome controller's perspective, a heading of 360 degrees off runway 32 was appropriate given the disposition of the arriving aircraft. It would also have complied with the noise abatement procedures and enabled him to visually separate the Aero Commander in azimuth with the 737, once the 737 was established on the final approach path.
The aerodrome controller's subsequent request for a 20 degree left turn for the Aero Commander is difficult to reconcile. The resultant heading of 070 degrees turned the Aero Commander towards the 737 and does not appear to be consistent with a resolution of the developing confliction. By that time the aerodrome controller could not have been certain from visual observation that the aircraft were not in close proximity.
The investigation was unable to determine why the aerodrome controller had a 'mindset' that the Aero Commander was departing on a heading of 360 degrees, when that option was never discussed or coordinated with the approach controller. The higher workload that was reported to have resulted from The Australian Advanced Air Traffic System data upgrade may have had an adverse effect on the aerodrome controller's cognitive processes towards the end of the night shift. The possibility that fatigue contributed to the occurrence could not be discounted.
Factual Information
Sequence of events
On 14 April 2005, an Aero Commander 500-S aircraft, registered VH-YJR, departed Brisbane aerodrome on a non-scheduled flight to Maryborough, Qld. It passed within 1 NM horizontally and 500 ft vertically of a Boeing Company 737-76Q (737) aircraft, registered VH-VBU, that was inbound from Darwin, NT, on a scheduled passenger service.
The Aero Commander became airborne off runway 32 at 0543 Eastern Standard Time, 4 minutes after the nominated first light for Brisbane aerodrome. The Brisbane aerodrome controller had instructed the pilot of the Aero Commander to turn right, once airborne, onto a heading of 090 degrees and to climb to 2,000 ft. The pilot complied with the departure instructions and contacted the approach controller on the approach frequency. The approach controller acknowledged that broadcast and asked the pilot for 'good forward speed'.
The crew of the 737 were on the approach frequency and were positioning the aircraft for final approach to runway 19. Although the pilot of the Aero Commander and the crew of the 737 were on the approach frequency, the aerodrome controller confirmed with the approach controller that he was visually separating both aircraft as had been previously agreed. The aerodrome controller later reported that he was expecting the approach controller to assign a heading of 360 degrees to the pilot of the Aero Commander.
The approach controller passed traffic information to the pilots of both aircraft and the Aero Commander pilot sighted the 737 soon after. At 0544:20 the crew of the 737 reported that they were established on the final approach path for runway 19. The approach controller advised them that the Aero Commander was going to cross the runway 19 final approach path and that the tower was providing visual separation.
The aerodrome controller became concerned about the separation between the two aircraft and at 0544:50 asked the approach controller to instruct the pilot of the Aero Commander to turn left 20 degrees. That instruction was passed and the Aero Commander pilot complied. The aerodrome controller was still concerned and asked the approach controller to instruct the pilot of the Aero Commander to make an immediate hard left turn onto a heading of 360 degrees. The approach controller advised the aerodrome controller that he was concerned about that heading and did not transmit the instruction.
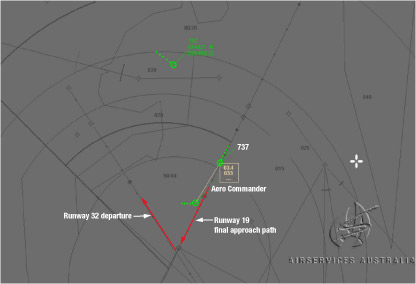
By 0545:26 the aerodrome controller considered that the Aero Commander had crossed the runway 19 final approach path. In response to a request by the approach controller, the pilot of the Aero Commander confirmed that he could see the 737, but at that stage the 737 crew had not seen the Aero Commander. Not long after that, the 737 crew saw the Aero Commander and were subsequently transferred to the Brisbane tower frequency. Figure 1 shows the position of the two aircraft as the Aero Commander crossed the final approach path at 0545:30.
Figure 1: Relative flight paths of the Aero Commander and the 737 as the Aero Commander crossed the final approach path of runway 19 at 05:45:30
A review of the recorded radar data showed that separation between the aircraft reduced to a minimum of 0.95 NM horizontally, at which time vertical separation had reduced to 500 ft.
Noise abatement procedures
The noise abatement procedures applicable at Brisbane at the time of the occurrence specified that all aircraft departing runway 32 between 2200 and 0600 must be contained within a sector of airspace between 360 and 120 degrees, over water, until leaving 5,000 ft. A heading of 360 degrees for a departure from runway 32 would have complied with those requirements.
To comply with the noise abatement procedures, runway 19 was the nominated duty runway for arrivals, and runway 01 was the nominated duty runway for departures. Pilots were also advised, on the automatic terminal information service, to obtain approval from air traffic control prior to starting engines. The requirement for a start clearance in thesecircumstances was in accordance with the Manual of Air Traffic Services (MATS) and enabled any delays to be absorbed on the ground before an aircraft's engines were started.
The aerodrome controller issued a start clearance to the pilot of the Aero Commander. The aerodrome controller did not coordinate the start clearance with the approach controller, nor was he required to do so. The ADC was required to review the disposition of inbound traffic when making a decision as to the timing of a start clearance.
The approach controller reported that he instructed the aerodrome controller to assign a departure heading of 090 to the pilot of the Aero Commander to ensure compliance with the noise abatement procedures.
Air traffic control separation standards and procedures
Control of aircraft in the Brisbane aerodrome terminal area was provided by an aerodrome controller located in the control tower using visual procedures, or by an approach controller using radar information. The MATS stated that the primary role of aerodrome controllers was to maintain visual observation of aircraft operations. Coordination of responsibilities and roles was required between the aerodrome controller and the approach controller, and formal guidelines were specified in a letter of agreement. The letter of agreement stated in part that:
In visual conditions, separation is achieved by the application of a radar standard or the provision of visual separation.
It also stated that:
In the application of visual separation, BNT [Brisbane aerodrome controller] shall ensure that separation in azimuth 1 is maintained until the establishment of a radar or procedural separation standard … In all situations where BNT is providing visual separation, traffic that will operate in close proximity will be retained on TWR [tower] frequency.
Although the aerodrome controller transferred the pilot of the Aero Commander to the departures frequency, the approach controller did not accept separation responsibility for the aircraft after the 737 was established on the runway 19 final approach path. He reported that he may not have been able to maintain the minimum radar separation standard of 3 NM horizontally, or 1,000 ft vertically.
The aerodrome controller reported that he accepted responsibility for visual separation between the two aircraft once the 737 was established on the runway 19 final approach path, because he had a 'mindset' that the Aero Commander was going to turn right onto a heading of 360 degrees once airborne. The aerodrome controller later reported that he would not have accepted responsibility for separation if he had realised that the approach controller had assigned a heading of 090 degrees, because that heading would not have enabled him to maintain visual separation between the two aircraft. Although the pilot of the Aero Commander advised the approach controller that he had the 737 in sight, the approach controller did not assign responsibility for separation to the pilot of the Aero Commander. There was an infringement of separation standards.
The information in the letter of agreement was supported by the Manual of Air Traffic Services (MATS), which contained procedures to be used by air traffic controllers. Paragraph 4.5.2.8 (effective 10 June 2004) stated that:
In providing visual separation, controllers should rely primarily on azimuth. Visual separation by judgement of relative distance or height shall be used only with such wide margins that there is no possibility of the aircraft being in close proximity.
The Brisbane tower was equipped with a radar display that provided the aerodrome controller with the same traffic display that was provided to the approach controller. The MATS addressed the use of tower radar in an aerodrome control service. It stated that the tower radar display was available for the determination of the altitude, position, or tracking of aircraft to establish or monitor separation. However, the MATS also stated that:
…the use of Tower radar should not impinge upon an aerodrome controller's primary function of maintaining a visual observation of operations on and in the vicinity of the aerodrome.
The MATS also stated that separation assurance could be achieved through planning traffic to ensure separation, executing the plan to achieve separation and monitoring the situation to ensure that the plan and the execution are effective.
Aerodrome controller
The aerodrome controller was trained and rated for the aerodrome control function at Brisbane. At the time of the occurrence he was nearing the end of a night shift which had commenced at 2200 the previous day. He reported that there had been a data upgrade to The Australian Advanced Air Traffic System during the night. The aerodrome controller considered that the data upgrade resulted in a higher workload than a standard night shift.
The aerodrome controller reported that, at the time of the occurrence, he felt fatigued. He also reported that he was feeling slightly unwell, but that he considered himself fit for duty. He was sleeping adequately and, apart from the slight illness, there were no indications of any personal, physiological or medical issues that were likely to have influenced the controller's performance.
Meteorological information
The weather information being broadcast to pilots for Brisbane Airport at the time of the occurrence advised that the visibility was greater than 10 km, that there were showers in the area and some cloud at 2,500 ft. The wind was reported as 180 degrees at 8 kts, with a maximum downwind of 10 kts on runway 01.
1. Horizontal bearing or direction.
Summary
On 14 April 2005, an Aero Commander 500-S aircraft, registered VH-YJR, departed Brisbane aerodrome on a non-scheduled flight to Maryborough, Qld. It passed within 1 NM horizontally and 500 ft vertically of a Boeing Company 737-76Q (737) aircraft, registered VH-VBU, that was inbound from Darwin, NT, on a scheduled passenger service.