In the evening of 29 April 2023, 2 Qantas Boeing 737-838 aircraft were undertaking operations from runway 16L at Sydney Airport, New South Wales. VH-VZW was on final approach to land while VH-VZM was preparing to take off. Shortly after VH-VZM commenced the take-off roll the aerodrome controller identified the spacing between the 2 aircraft had reduced to a distance that could result in compromised runway separation and instructed the crew of VH-VZW to go-around. During the missed approach, the separation between the 2 aircraft reduced to 0.8 NM (1.5 km) horizontally and 330 ft vertically as they climbed away from the runway.
What the ATSB found
The ATSB identified that the go-around instruction issued by the aerodrome controller was delayed by about 12 seconds due to an inadvertent interjection by the tower shift manager. The ATSB also found that the instruction issued to the crew of VH-VZW by the aerodrome controller subsequent to the go-around was interpreted as a cancelation of the published missed approach procedure. Consequently, the crew did not turn left at 600 ft as required by the procedure and instead continued on the runway track.
What has been done as a result
Airservices Australia advised that in response to the occurrence it would, among other actions:
conduct an analysis of landing runway occupancy times at Sydney Airport
add defensive controlling techniques and minimum assignable altitudes for go-around scenarios
conduct an assurance review of go-arounds at Sydney involving a second aircraft requiring controller intervention
add night-time go-around scenarios to compromised separation training.
Safety message
Aerodrome controllers are required to maintain an orderly flow of air traffic, with minimal delays, while ensuring safe separation between arriving and departing aircraft. This complex operation requires controllers to exercise their professional judgement when applying visual separation standards in a variety of environmental and procedural scenarios. In such a setting, it is inevitable that errors will be made by controllers and pilots alike. Consequently, the sociotechnical system within which these activities take place should be designed to be resilient of these errors and reduce the impact individual actions can have on the overall safety of operations.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
In the evening of 29 April 2023, 2 Qantas Boeing 737-838 aircraft were using runway 16L at Sydney Airport, New South Wales:
VH-VZW on final approach to land
VH-VZM awaiting clearance to enter the runway to take off.
VH-VZW was conducting a scheduled air transport flight from Auckland Airport, New Zealand to Sydney Airport, with 2 flight crew, 5 cabin crew and 100 passengers on board. VH-VZM was conducting a scheduled air transport flight to Brisbane Airport, Queensland, with 2 flight crew, 4 cabin crew and 52 passengers on board.
Air traffic control was being provided to both aircraft by the aerodrome controller east (ADCE) in the Sydney Airport tower (see Sydney Airport air traffic control). The wind at the time was 202°–228° at 11–14 kt, the cloud cover[1] was few at 1,500–2,800 ft and scattered at 2,400–4,900 ft, and it was night.
At 1745:39, as a landing Cessna Citation Mustang passed the runway 16L threshold, the ADCE instructed the crew of VH-VZM to line up and wait on runway 16L with an assigned departure heading of 140°. The crew of VH-VZM acknowledged the instruction and taxied the aircraft onto the runway. The crew then waited for take-off clearance. At 1746:07, the ADCE saw that the Mustang was taking longer than anticipated to vacate the runway and instructed the crew to expedite the exit. In total, the Mustang took 73 seconds from landing to vacating the runway, about 23 seconds longer than the ADCE expected.
At 1747:03, the ADCE issued a take-off clearance to the crew of VH-VZM. At this time VH-VZW was about 2.4 NM (4.4 km) from the threshold of runway 16L on approach to land. The crew of VH-VZM pushed the thrust levers forward and waited for both engines to stabilise. This process took about 4 seconds longer than normal due to a permissible unserviceability[2] affecting the performance of one of the engines. At 1747:18, the flight crew pressed the take-off go around (TOGA)[3] button and commenced the take-off.
Meanwhile, VH-VZW was now about 1.7 NM (3.1 km) from the threshold of runway 16L. The captain of VH-VZW, who was pilot monitoring (PM),[4] assessed that the spacing between VH-VZM and VH-VZW had reduced to a distance that would likely result in a ‘go-around’.[5] Consequently, the captain instructed the first officer (FO), who was pilot flying (PF), to mentally prepare for a possible go-around.
The ADCE, also aware of the reduced spacing between the 2 aircraft (see Runway separation standard) and the potential for compromised runway separation, decided to issue a go-around instruction to the crew of VH-VZW and alerted the tower shift manager (TSM) of the situation (see section titled Sydney Airport air traffic control). The TSM moved to look at the runway and began assessing the traffic scenario.
At 1747:22, the ADCE contacted the crew of VH-VZW to issue the go-around instruction. However, before the ADCE issued the instruction itself, the TSM said ‘wait’. The ADCE hesitated for a moment and, having initiated contact and needing to complete the communication, instructed the crew of VH-VZW to continue with the approach to land. The TSM later recalled that they had inadvertently spoken, but their intention was for the ADCE to continue with the go-around instruction. The ADCE then waited for further advice from the TSM, but the TSM did not say anything (the TSM recalled gesturing for the ADCE to continue). The ADCE recalled informing the TSM that they would proceed with the go-around instruction.
At 1747:34, the ADCE instructed the crew of VH-VZW to conduct a go-around. The instruction was acknowledged by the crew of VH-VZW which was now about 1.1 NM (2.0 km) from the runway 16L threshold. At 1747:36 the crew of VH-VZW initiated the go-around from an altitude of about 450 ft. (The ATSB determined that, had the go-around instruction been issued at the original intended time, VH-VZW would have been about 0.5 NM (0.9 km) further from the threshold and 160 ft higher than when the actual instruction was issued.)
At 1747:38, the ADCE issued a further instruction to the flight crew of VH-VZW, stating ‘passing 2,100 turn left heading 090’. The ADCE stated that they were aware of a requirement not to issue a turn instruction to VH‑VZW until it had reached the minimum sector altitude (MSA) of 2,100 ft (see Turn instructions at night below the minimum sector altitude).
Although the flight crew heard the instruction, they did not acknowledge it immediately due to the workload associated with the go-around procedure. They interpreted it as an amended missed approach instruction. As a result, the crew continued to fly the runway track as the aircraft climbed, rather than turning left onto a heading of 125° at 600 ft as was required by the published missed approach procedure (see Missed approach).
Meanwhile, VH-VZM was accelerating along the runway and had passed 87 kt. The captain of VH-VZM heard the go-around instruction issued to VH-VZW and they expected the aircraft to fly the published missed approach procedure and that this would provide sufficient spacing between the aircraft. The captain then monitored the traffic collision avoidance system (TCAS)[6] which displayed a ‘proximate traffic’ indication[7] 600 ft above VH-VZM (which was VH-VZW).[8]
At 1748:03, the ADCE asked if the crew of VH-VZW had received the instruction to turn left onto a heading of 090° on passing 2,100 ft, to which they responded that they had. The ADCE and the TSM visually observed the 2 aircraft as they climbed away from the runway. They also had a surveillance display showing the dispositions of aircraft in the vicinity of the airport. During this time the TSM no longer felt ‘comfortable’ with the separation between the 2 aircraft. As a result, the TSM recalled advising the ADCE that they should issue a safety alert and turn VH-VZW away from VH-VZM (see Reduced separation and safety alerts).
At 1748:17, the ADCE issued a safety alert to VH-VZW stating ‘safety alert traffic 12 o'clock low heading 140 if you're visual turn left now’. At 1748:24, the crew of VH-VZW initiated a left turn while climbing through 1,533 ft. The TSM recalled further stating to the ADCE that the aircraft needed to be turned further onto a heading of 060°.
At 1748:32, when VH-VZW was at an altitude of 1,710 ft and not climbing as fast as the ADCE expected, the ADCE issued a further instruction to the crew to turn left onto a heading of 060° to put the aircraft onto diverging flightpaths sooner. The ADCE determined that such an instruction carried less risk than permitting the scenario to continue until VH-VZW had reached the MSA. While VH-VZW was below the MSA when issued the instruction to turn, the ADCE was confident that the aircraft was above the highest obstacles in the vicinity. This instruction was acknowledged by the flight crew and the aircraft continued the left turn onto the new heading.
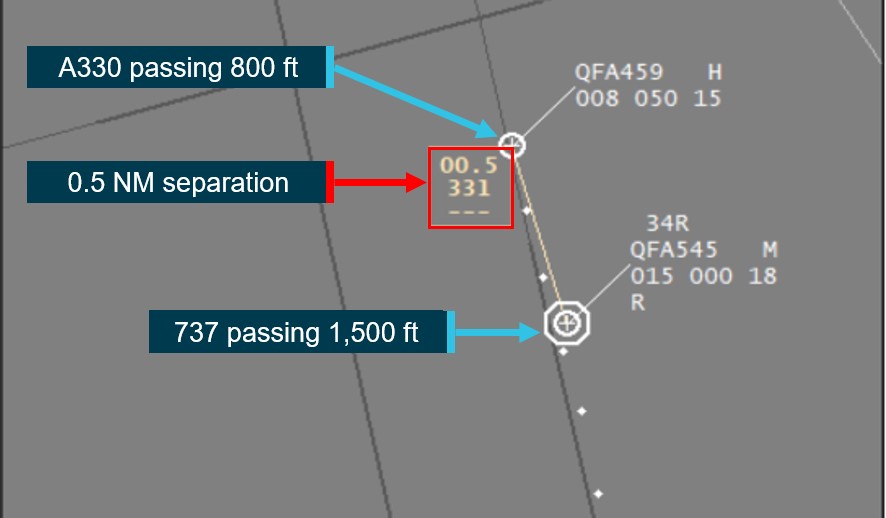
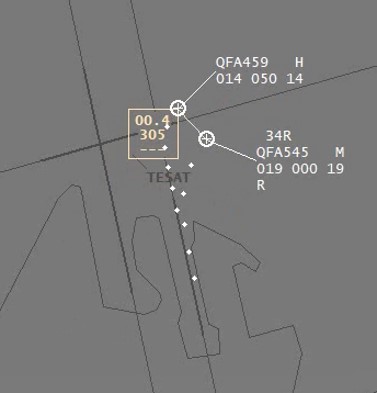
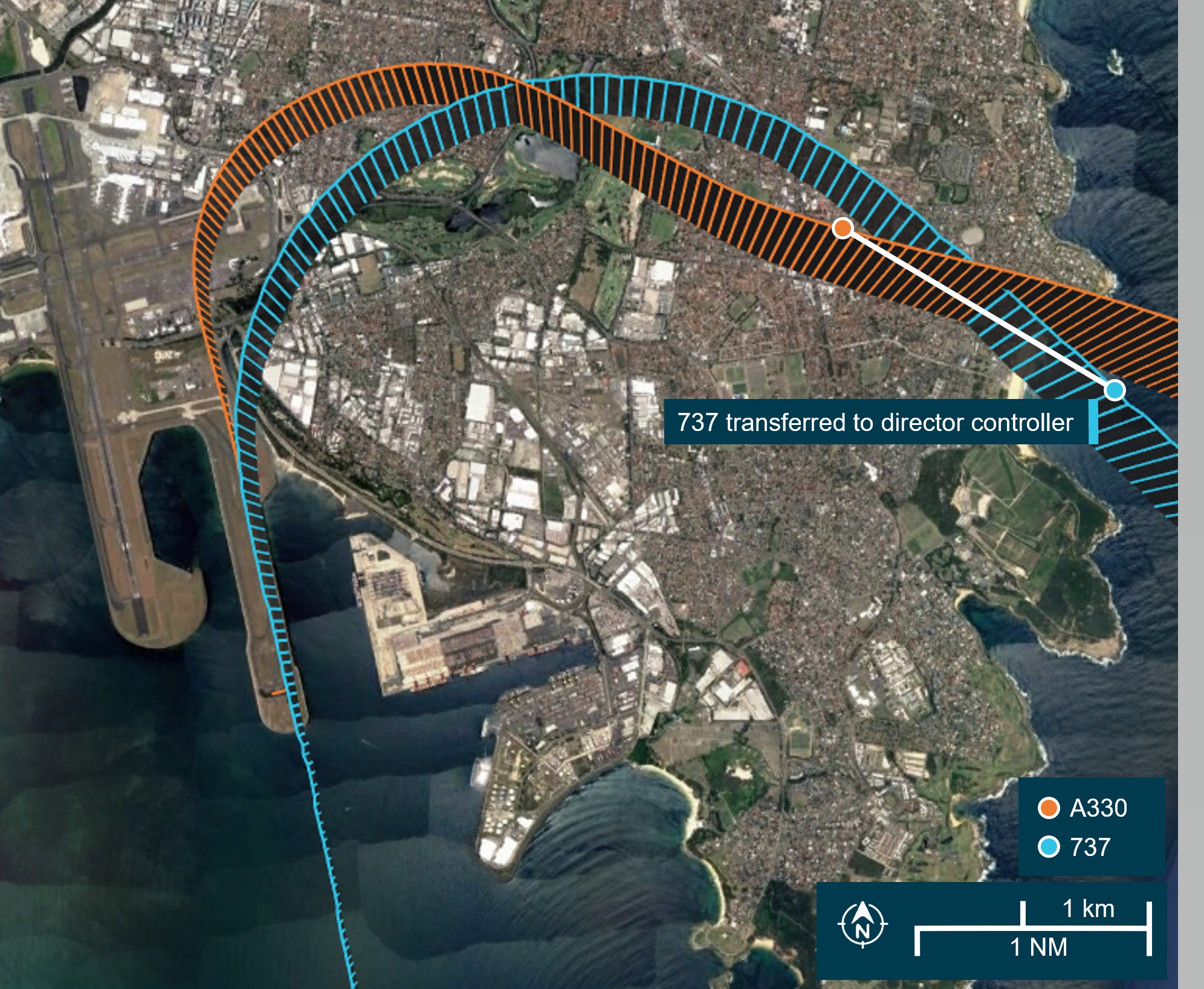
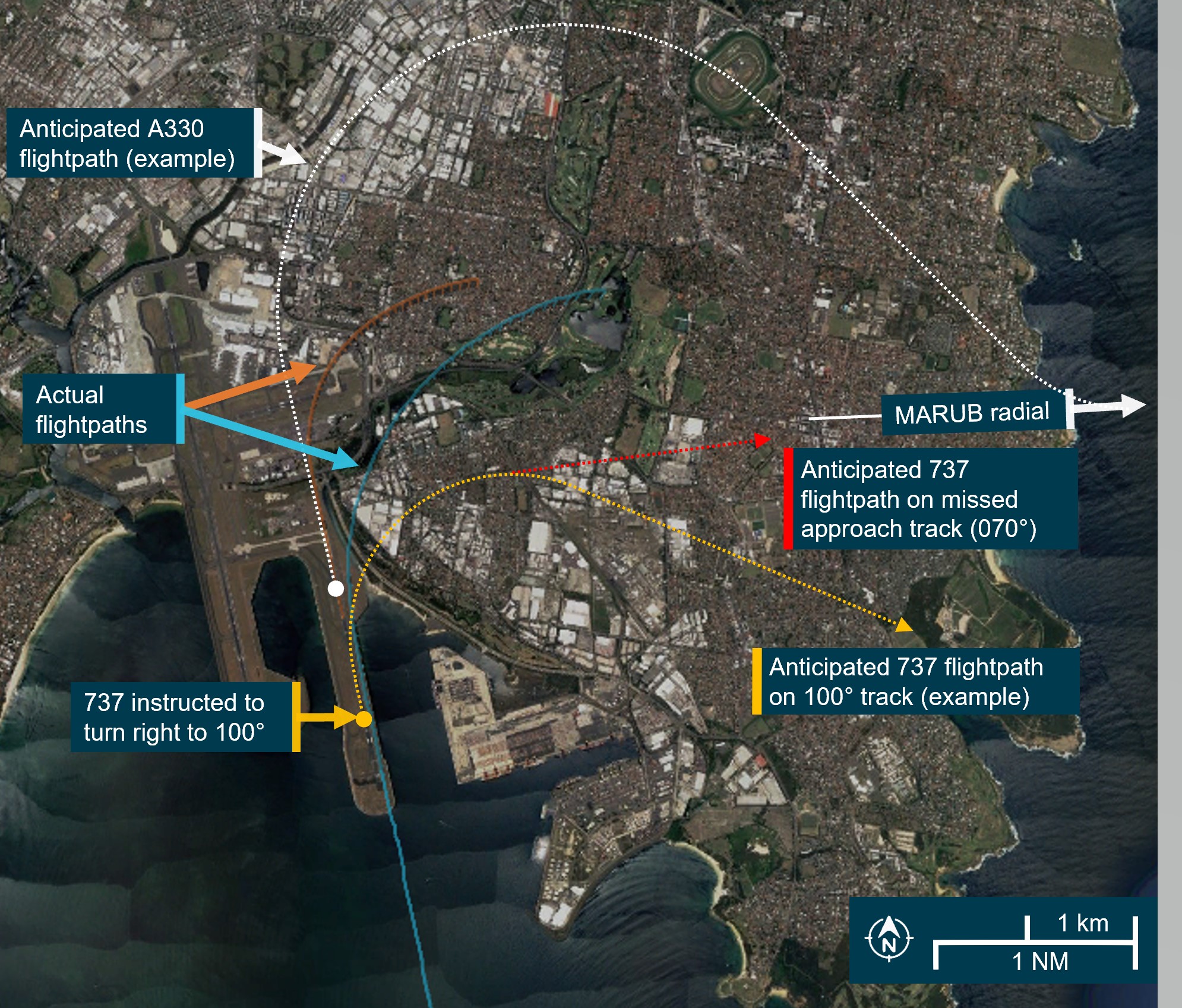
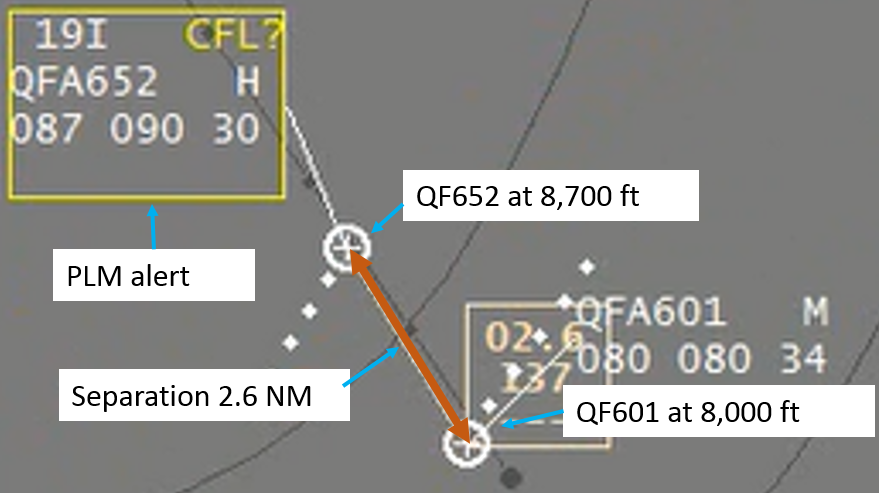
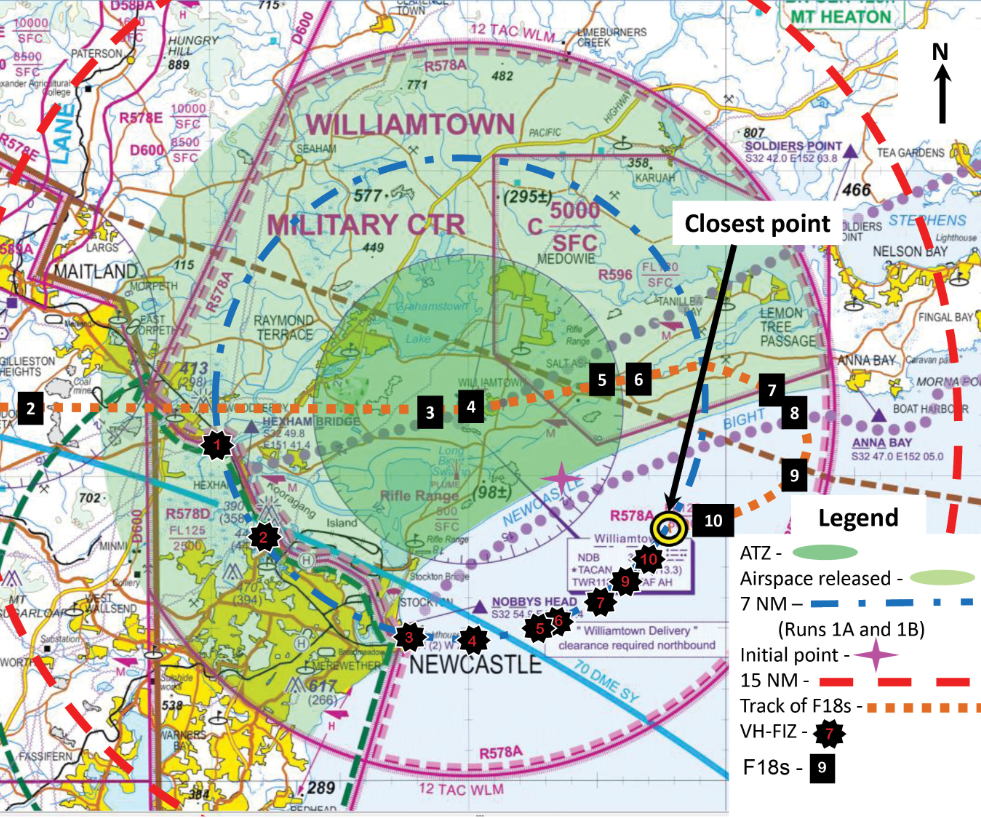
At 1748:38, the closest slant range between the 2 aircraft occurred, with separation reducing to 0.8 NM (1.5 km) horizontally and 330 ft vertically (Figure 1). Neither crew had visual contact with the other aircraft and no TCAS resolution advisory[9] or traffic advisory[10] was triggered. The controllers had both aircraft in sight throughout the occurrence, and the ATSB later assessed that the visual and surveillance information available to the controllers in the tower, accounting for the possibility of visual errors, was sufficient for visual separation[11] to be maintained.
Figure 1: Overview of aircraft flight paths
White lines link the locations of the two aircraft at the same point in time.
Source: Google Earth, annotated by the ATSB
With VH-VZW continuing to turn towards the east-north-east, the 2 aircraft began to diverge. At 1749:03, the ADCE transferred VH-VZM to the departure controller and the aircraft continued to its destination. At 1749:44, the ADCE transferred VH-VZW to the Sydney Airport director and the aircraft later landed on runway 16R.
Context
Personnel information
VH-VZM flight crew
Both flight crew held an air transport pilot licence (ATPL) aeroplane and Class 1 aviation medical certificate. The captain had a total of 12,413 hours of aeronautical experience, including 2,301 hours on 737 variants. The captain reported feeling ‘okay, somewhat fresh’ at the time of the occurrence. The first officer had 11,700 hours of aeronautical experience, including 7,800 hours on 737 variants. The FO reported feeling ‘very lively, responsive, but not at peak’ at the time of the occurrence.
VH-VZW flight crew
Both flight crew held an ATPL aeroplane and Class 1 aviation medical certificate. The captain had a total of 13,220 hours flight time, with 9,430 hours on 737 variants. They reported feeling ‘fully alert’ at the time of the occurrence. The FO had a total of 8,100 hours flight time, with 2,650 hours on 737 variants.
Aerodrome controller east
The ADCE had about 14 years experience as an approach and tower controller with the Royal Australian Air Force and then Airservices Australia. They had been operating in the Sydney Airport tower for about 3 years and held endorsements for the aerodrome controller and coordination roles. The ADCE’s last performance assessment (check) prior to the occurrence was completed on 2 March 2023 and they were assessed as competent. They reported feeling ‘alert’ at the time of the occurrence.
Tower shift manager
The TSM had about 10 years’ experience as an enroute and tower controller with Airservices Australia. They had been operating in the Sydney Airport tower for about 5 years and held endorsements for the aerodrome controller, surface movement controller, airways clearance delivery, coordination, and TSM roles. They had been a TSM for about 1 year. The TSM’s last performance assessment prior to the occurrence was completed on 17 March 2023 and they were assessed as competent. They reported that they had slept well and ‘felt fine’ at the time of the occurrence.
Fatigue analysis
Analysis indicated that the ADCE, TSM, and the flight crews of VH-VZM and VH-VZW were probably not experiencing a level of fatigue known to have an adverse effect on performance.
Sydney Airport
Syndey Airport has 2 parallel runways oriented 155°/335° magnetic (16L/34R and 34L/16R) and another runway oriented 062°/242° (07/25). At the time of the occurrence, the airport was operating in parallel runway mode with aircraft taking off and landing on runways 16L and 16R. The elevation of terrain to the east of runway 16L within a radius of 10 NM (18 km), is about 150‑350 ft.
Sydney Airport air traffic control
General information
The Sydney tower was located to the east of runway 16R/34L and south of runway 07/25. There were 8 Airservices Australia[12] personnel located within the Sydney tower at the time of the occurrence. This included the ADCE, who was responsible for providing traffic management to aircraft taking off and landing on runway 16L, and the TSM, who was responsible for the overall operation of the tower. According to Airservices procedures, the TSM was also responsible for the ‘supervision’ of controller activities and held ‘operational command authority’ (OCA) for the Sydney tower.
Supervision and operational command authority
The Airservices Australia National ATS administration manual (NAAM) outlined the procedures associated with the TSM’s supervision and operational command authority responsibilities.
Within the NAAM, the stated purpose of supervision was to ‘provide tactical management of risks while maintaining efficient air traffic operations’ and involved the ‘observation of air traffic service delivery and, where necessary, supporting, intervening, or directing activities within the area of responsibility’.
However, the procedures contained within the NAAM relating to the TSM’s operational command authority (OCA) responsibilities stated:
OCA does not give the holder the authority to instruct an operational controller to take certain actions such as directing a controller to issue an operational control instruction. The operational controller is always responsible for traffic separation but may accept advice from the OCA holder.
The operational command authority held by the TSM gave the role the ‘authority to make decisions on behalf of a unit’ (in this instance the Sydney tower). This authority was described by the TSM as involving a ‘duty of care’ for the overall safety of aircraft traffic managed by Sydney tower.
The NAAM required the TSM to 'initiate and manage necessary short-term mitigation actions’ when a situation occurs that ‘has or may cause a risk to the continued safe operation’ of the airways. These mitigations included workload management, reduction in task complexity, and additional support, observation or supervision. The controllers involved in this occurrence stated that, if the situation necessitated it, it was acceptable for a TSM to issue an instruction to a controller to deconflict an impending or actual unsafe scenario.
Air traffic separation
Visual separation
Throughout the occurrence, the ADCE was providing visual separation to VH-VZW and VH‑VZM. This form of separation required the controller to visually observe the aircraft under their control and apply an azimuth (horizontal) spacing between aircraft.
The Airservices Manual of air traffic services (MATS) stated:
When applying visual separation, consider.
a) aircraft performance characteristics, particularly in relation to faster following
b) aircraft and closure rates;
c) position of the aircraft relative to each other;
d) projected flight paths of the aircraft;
e) possibility of an ACAS [airborne collision avoidance system] RA [resolution advisory] due to closer proximity of operation;
f) known weather conditions; and
g) the possibility of visual errors.
Turn instructions at night below the minimum sector altitude
Aerodrome controllers providing visual separation at Sydney Airport at night or during instrument meteorological conditions were restricted from issuing turn instructions (vectors) prior to an aircraft having reached a minimum sector altitude (MSA)[13] of 2,100 ft.
This restriction was further communicated to Sydney Airport controllers in Airservices Australia standardisation directive DIR_22_0036 (issued 10 June 2022, expired 9 September 2022). This directive referenced the MATS which stated controllers were to ‘assign levels no lower than the applicable LSALT [lowest safe altitude][14] unless the pilot has accepted responsibility for terrain clearance’. The purpose of the requirement was to ensure the controller maintained responsibility for terrain clearance as pilots may not be able to see terrain and obstacles.
Separately, the MATS stated:
Do not allow anything in these instructions to preclude you [the controller] from exercising your best judgement and initiative when:
a) the safety of an aircraft may be considered to be in doubt; or
b) a situation is not covered specifically by these instructions.
Reduced separation and safety alerts
Airservices had a compromised separation recovery training package, which defined compromised separation as occurring when ‘an aircraft is, or without controller intervention will be, in unsafe proximity or at risk of a collision with another aircraft’. In situations where an unsafe proximity existed, a controller was required to issue a safety alert to draw a flight crew’s attention to the traffic scenario. A safety alert was required to be issued as a priority unless the flight crew had advised that action was being taken to resolve the situation or that the other aircraft was in sight.
The ADCE had undergone compromised separation recurrency training in May 2022. The purpose of the recurrency training was to ‘refresh the knowledge and skills’ of the controller to effectively identify and recover a compromised separation scenario. The training was required to be undertaken every 3 years and comprised a computer-based training module, which was generic to all locations, and 4 simulator sessions that involved scenarios specific to the Sydney Airport environment. The ADCE was assessed as competent during these simulator sessions.
Runway separation standards
Runway separation standards ensure sufficient separation between aircraft using the same runway. For an aircraft taking off ahead of an aircraft that is on final approach to land, as was the case for VH-VZM, the standard defined in MATS did not permit a take-off clearance to be issued until:
the arriving aircraft is sighted by the controller and is reasonably assured of landing; or
separation can be assured if the arriving aircraft conducts a missed approach.
For an aircraft landing behind a preceding aircraft that was taking off, as was the case for VH‑VZW, the standard defined in MATS did not permit the landing aircraft to cross the runway threshold until the departing aircraft was airborne and:
had either commenced a turn; or
was beyond the point on the runway at which the landing aircraft could be expected to complete its landing roll and there was sufficient distance to enable the landing aircraft to manoeuvre safely in the event of a missed approach.
Go-around and missed approach
A go-around refers to the action of aborting a landing from final approach or during the touchdown.
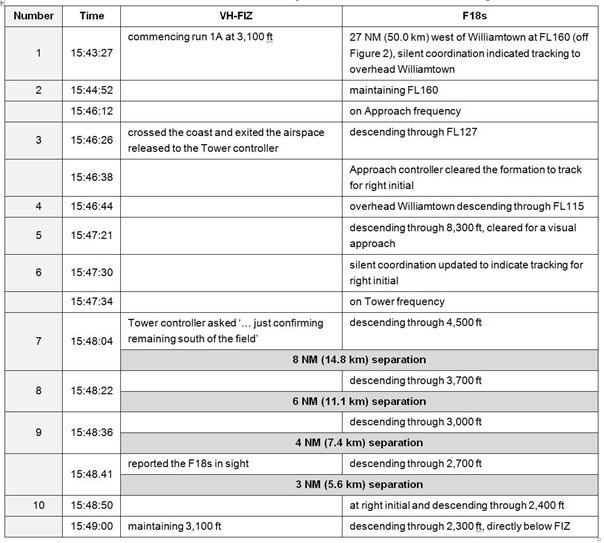
A missed approach procedure provides instrument flight rules[15] aircraft with terrain and obstacle clearance along the missed approach path during a go-around. The flight crew of VH-VZW were flying a GBAS landing system (GLS) approach for runway 16L. In the event of a go-around, the missed approach procedure required a flight crew to initially climb to 600 ft and then execute a left turn onto a heading of 125° (Figure 1). The crew were then required to climb to 3,000 ft or as directed by air traffic control.
Figure 2: Sydney GLS runway 16L approach chart with missed approach requirements (blue box)
Source: Airservices Australia, annotated by the ATSB
Related occurrences
ATSB study on loss of separation occurrences in Australian airspace (AR-2012-034)
The ATSB’s study on loss of separation events involving aircraft in Australian airspace (January 2008 – June 2012) found that ‘assessing and planning’ or ‘monitoring and checking’ errors were involved in the majority of individual controller actions that contributed to loss of separation occurrences. This involved the ineffective management of compromised separation before it became a loss of separation event, and controller actions associated with maintaining awareness of traffic disposition.
Unsafe proximity and radar vector below minimum vector altitude involving a Boeing 777‑31HER, A6-EBU, and two 737-838s, VH-VXS and VH-VYE, Melbourne Airport, Victoria, on 5 July 2015 (AO-2015-084)
On the evening of 5 July 2015, land and hold short operations (LAHSO) were in effect at Melbourne Airport, Victoria. During these operations, an Emirates Boeing 777 was cleared for an immediate take-off from runway 34 while 2 Qantas Boeing 737s were on approach to runways 34 and 27. This resulted in the crew of the Boeing 737 on approach to runway 27 initiating a missed approach, followed by the crew of the Boeing 737 on approach to runway 34 being instructed by air traffic control (ATC) to go-around. The Boeing 737 on approach to runway 34 was then radar vectored by ATC below the minimum vector altitude.
The ATSB found that:
The hazard associated with the inability to separate aircraft that are below the appropriate lowest safe altitude at night was identified but not adequately mitigated. This resulted in a situation where, in the event of a simultaneous go-around at night during land and hold short operations at Melbourne Airport, there was no safe option available for air traffic controllers to establish a separation standard when aircraft were below minimum vector altitude.
Airservices subsequently provided training in night operations during land and hold short operations at Melbourne Airport, and introduced a stagger strategy for Melbourne arrivals.
Close proximity involving Boeing 737, VH-VZO and Airbus A330, VH-EBJ at Sydney Airport, New South Wales, on 5 August 2019 (AO-2019-041)
In the evening of 5 August 2019, a Boeing 737 was on approach to land on runway 34R at Sydney Airport while an Airbus A330 had commenced a take-off from the same runway. Shortly after the A330 was cleared for take-off, the ADCE identified that the runway separation standard could not be assured and they instructed the crew of the 737 to go-around. During the subsequent missed approach and turn to the right, the 737 came into close proximity with the A330. Among other findings, the ATSB found that controllers had no procedural controls to draw upon to separate aircraft following similar outbound tracks when they were below the minimum vector altitude, and there were no compromised separation training scenarios involving aircraft below this altitude at night.
Following the occurrence, Airservices included compromised separation scenarios in the Sydney tower controller instructor guide, where an aircraft is operating below the minimum vector altitude at night, and in 2023 Airservices advised that the training program also now included a missed approach with a preceding departure in instrument meteorological conditions.
Safety analysis
The aerodrome controller east (ADCE) instructed the crew of VH-VZM to line up and wait on runway 16L. A take-off clearance could not be issued until a landing aircraft had vacated the runway. This aircraft took about 23 seconds longer to exit the runway than the ADCE had originally anticipated. This extra time meant VH-VZW, which was on final approach to land, was about 2.4 NM (4.4 km) from the threshold when the crew of VH-VZM was issued clearance to take off.
On receipt of the take-off clearance, VH-VZM took about 14 seconds to commence the take-off roll due, in part, to a permissible unserviceability affecting one engine’s performance. This delay further compressed the spacing between the 2 aircraft. Shortly after VH‑VZM commenced the take-off roll, the ADCE identified the spacing between the 2 aircraft had reduced to a distance that meant VH-VZW needed to go around to maintain the runway separation standard. The ADCE also had the option to not issue take-off clearance to the crew of VH-VZM or cancel it during the 14 seconds it took for the aircraft to commence the take-off roll, and this would have prevented the complication of having one aircraft taking off while another was going around.
Having decided to issue a go-around instruction to the crew of VH-VZW, the ADCE’s initial communication was inadvertently interrupted by the tower shift manager (TSM) who said ‘wait’. The TSM later stated that they did not intend to verbalise anything, and they meant for the ADCE to issue the go-around instruction. This verbal slip likely occurred at a time of high workload as the TSM attempted to assimilate the information associated with the traffic scenario.
The verbalisation of ‘wait’ by the TSM interrupted the ADCE’s management of the traffic scenario. While the TSM did not have the authority to direct the ADCE to issue a control instruction, the TSM was able to provide advice to the ADCE. Consequently, the ADCE deferred the go-around instruction for 12 seconds while they waited for the TSM to provide further guidance, which did not eventuate. This 12-second delay meant VH-VZW was 160 ft lower and 0.5 NM (0.9 km) closer to the threshold (and to VH-VZM) by the time the go-around instruction was finally issued.
Four seconds after instructing the crew of VH-VZW to go-around, the ADCE issued further instructions to the crew that required them to turn onto a heading of 090° at 2,100 ft. These instructions were provided to the crew at a time of high workload when VH-VZW had not yet reached 600 ft when they were meant to turn left onto a heading of 125° in accordance with the missed approach procedure. Consequently, the crew misinterpreted the instruction as cancellation of the missed approach procedure and they did not turn at this altitude. The timing of the additional instruction likely added workload compared with letting the crew undertake the go‑around manoeuvre, and the turn at 600 ft, before issuing any further turn instructions.
The TSM and ADCE monitored the 2 aircraft as they climbed away from the runway. During that time the ADCE issued a safety alert to the crew of VH-VZW to advise of the traffic ahead and then vectored the aircraft while it was below the minimum sector altitude. Although contrary to the Airservices Australia standardisation directive, the issuance of this instruction likely reduced the risk associated with the separation occurrence.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the separation occurrence involving Boeing 737, VH-VZM, and Boeing 737, VH-VZW, at Sydney Airport, New South Wales on 29 April 2023.
Contributing factors
The go-around instruction issued by the aerodrome controller was delayed by about 12 seconds due to an inadvertent interjection by the tower shift manager.
The instruction issued to the arriving 737 flight crew by the aerodrome controller subsequent to the go-around was interpreted by the flight crew as an instruction to cancel the published missed approach procedure and continue on the runway track before turning at 2,100 ft. Consequently, the 737 flight crew did not turn left at 600 ft as required by the procedure.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action
Airservices advised that it had or would undertake the following safety actions in response to this occurrence:
conduct a detailed analysis of landing runway occupancy times at Sydney, and possibly other major aerodromes, to determine expected runway occupancy times for different types of aircraft (including operator) and conditions (runway direction/wind/time of day/surface condition). This data to be disseminated to ATC [air traffic control] to assist when managing runway separation standards
Sydney tower to add defensive controlling techniques and minimum assignable altitudes applicable to go around scenarios, in particular at night or in IMC [instrument meteorological conditions]
conduct an assurance review examining go arounds at Sydney involving a second aircraft and requiring controller intervention. Specifically, analysing how separation and terrain clearance is being managed and possible reasons behind any unfavourable trending
standardisation directive disseminated to Sydney tower referring to MATS [manual of air traffic standards] 9.4.1.2.1 and outlining the importance of using the MSA [minimum sector altitude] of 2100 ft as the standard at night or in IMC as applicable to go around scenarios
standards to add night-time go around scenarios to compromised separation training
standardisation directive ATS_DIR_23_0037 disseminated to Sydney Tower referring to the NAAM [national air traffic services administrative manual] initial occurrence response requirements to be followed, and the importance of taking steps to assess the risk associated with the potential safety occurrence.
Sources and submissions
Sources of information
The sources of information during the investigation included:
captain and first officer of VH-VZW
captain and first officer of VH-VZM
aerodrome controller east
tower shift manager
flight data from VH-VZM and VH-VZW
air traffic control audio recordings and radar data
Airservices Australia
Qantas Airways
Civil Aviation Safety Authority.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
captain and first officer of VH-VZW
captain and first officer of VH-VZM
aerodrome controller east
tower shift manager
Qantas Airways
Civil Aviation Safety Authority
Airservices Australia.
Submissions were received from Airservices Australia. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky.
[2] An item of equipment that may be inoperative for a limited period until repairs can be made.
[3] The TOGA button changes various autopilot, autothrottle, and flight director settings to initiate a take-off or missed approach.
[4] Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[6] Traffic alert and collision avoidance system (TCAS): a type of airborne collision avoidance system that interrogates nearby aircraft and uses this information to calculate the relative range and altitude of this traffic. The system provides a visual representation of this information to the flight crew as well as issuing alerts should a traffic issue be identified.
[7] Proximate traffic: an alert issued when an aircraft is within a range of less than 6 NM and 1,200 ft, or a range of 6 NM if the traffic is not transmitting altitude information.
[8] There were no other aircraft in the immediate area.
[9] Resolution advisory (RA): a manoeuvre, or a manoeuvre restriction, calculated by an airborne collision avoidance system to avoid a collision. Pilots are expected to respond immediately to an RA unless doing so would jeopardise the safe operation of the flight.
[10] Traffic advisory (TA): an alert issued by an airborne collision avoidance system when the detected traffic may result in a conflict. Pilots are expected to initiate a visual search for the traffic causing the TA.
[12] Airservices is Australia's principal provider of air traffic services for civil airports and airspace.
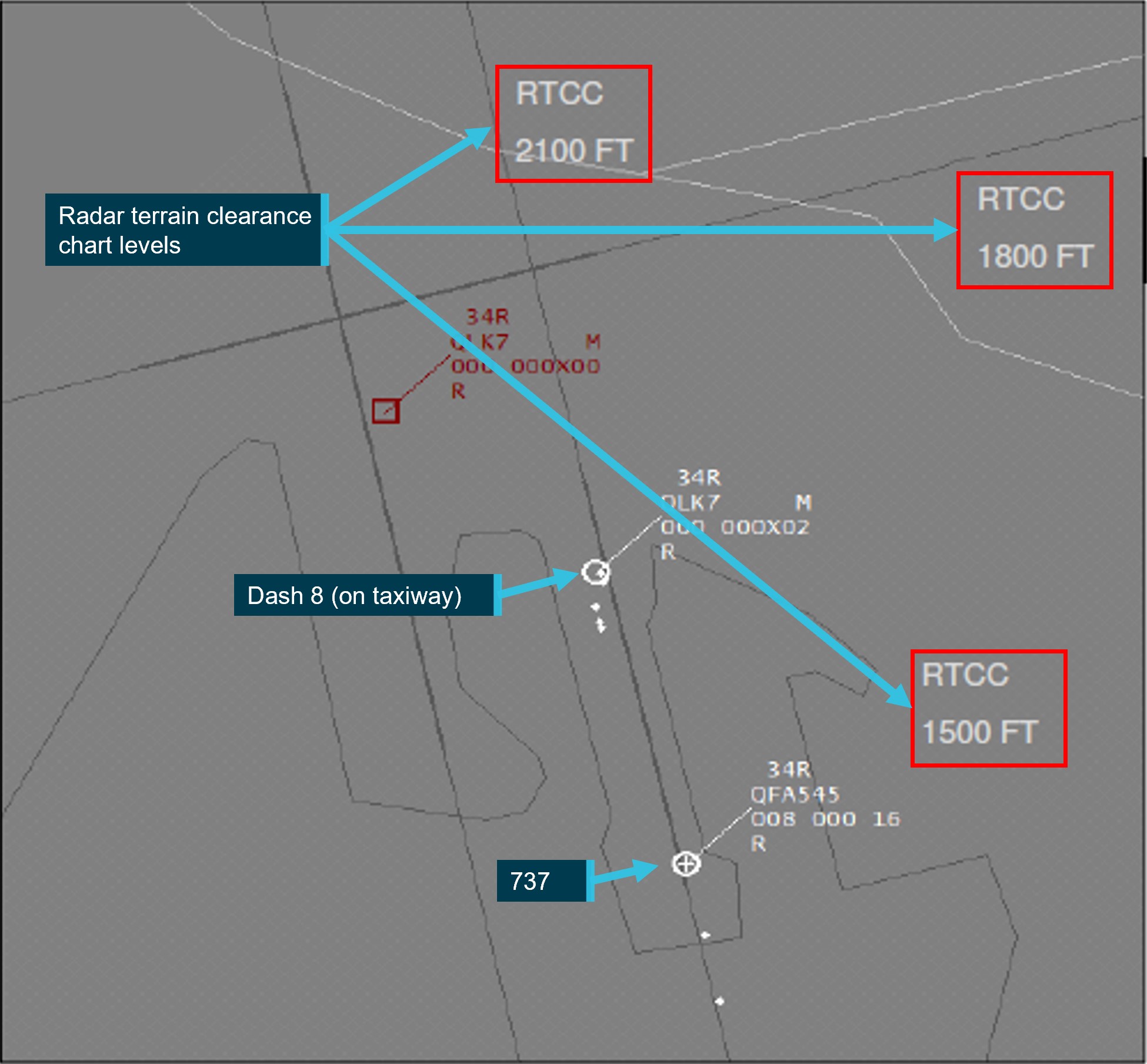
[13] Minimum sector altitude (MSA): the lowest altitude which will provide a minimum clearance of 1,000 ft above all objects in an area. Separately, the minimum vectoring altitude (MVA) was the lowest altitude a controller may assign to a pilot in accordance with a radar terrain clearance chart (RTCC), which was 1,500 ft in the area of the occurrence. In this context, the tower controllers used MSA as the minimum assignable altitude.
[14] The lowest altitude which will provide safe terrain clearance at a given place. LSALT includes MSA.
[15] Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft to operate in instrument meteorological conditions.
Occurrence summary
Investigation number
AO-2023-022
Occurrence date
29/04/2023
Location
Sydney Airport
State
New South Wales
Report release date
31/01/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Loss of separation
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
The Boeing Company
Model
737
Registration
VH-VZM
Serial number
34192
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
Departure point
Sydney Airport, New South Wales
Destination
Brisbane Airport, Queensland
Damage
Nil
Aircraft details
Manufacturer
The Boeing Company
Model
737
Registration
VH-VZW
Serial number
39359
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On the afternoon of 28 September 2022, a Boeing Company 787-9 (787), registered G-ZBKF, was being operated by British Airways as flight number BA16, on an air transport flight from Sydney, New South Wales, to Singapore. At the same time, an Airbus A330-202 (A330), registered VH-EBK, was being operated by Qantas Airways as flight number QF926, on an air transport flight from Sydney to Cairns, Queensland.
At approximately 1508 local time, BA16 was cleared for take-off from runway 16R to conduct the DEENA SEVEN (DEENA 7) standard instrument departure (SID). Shortly after, QF926 was also cleared for take-off conducting the same SID. The Departure controller cleared both aircraft, in sequence, to climb to flight level 280 via the SID.
During the departure, the following aircraft climbed faster than the controller anticipated and turned towards the next waypoint inside the preceding aircraft, resulting in a loss of separation.
What the ATSB found
The ATSB found that the actual climb performance of the A330 was greater than the climb performance of the 787 which was not expected, or identified, by the controller due to their focus on other aircraft. This resulted in the A330, while complying with the SID, turning inside the leading 787, resulting in the loss of separation.
The ATSB also found that the design of the DEENA SEVEN SID did not provide a positive method of providing separation assurance to aircraft with different performance characteristics. As the aircraft had to satisfy 2 separate conditions prior to turning, there was no way of ensuring aircraft would turn at the same distance from the airport. That is, separation could not be assured.
What has been done as a result
Airservices Australia advised that the DEENA SEVEN SID has been redesigned to remove the conditional requirements of the procedure. The change has been approved and planned to be released as part of the Western Sydney International (Nancy-Bird Walton) Airport project. At the time of writing Airservices Australia was developing a timeline for the implementation of the redesigned SID. As such, the ATSB will continue to monitor the safety issue and provide website updates.
Safety message
Maintaining separation in high traffic terminal areas, such as Sydney, requires that both controllers and flight crews remain vigilant, maintain open communications, and use the available systems and tools to minimise the risk of errors. When sequencing departures, controllers should consider a number of factors, including how the flight duration (and the associated fuel load), will likely affect aircraft climb performance.
Standard instrument departures are designed to expedite the safe and efficient flow of air traffic operating from airports through the use of specific routings, levels, speed restrictions and waypoints. Where a SID, with limited designed separation assurance is used, it is important that air traffic controllers regularly monitor individual aircraft performance rather than rely on expected flight characteristics.
The Sydney Airport automatic terminal information service (ATIS)[1] indicated that parallel runways were in use, including simultaneous independent departures[2] from runways 16R and 16L.[3]
At approximately 1508 local time, BA16 was cleared for take-off from runway 16R by the Sydney tower controller. They were cleared to conduct a DEENA SEVEN (DEENA 7) standard instrument departure (SID)[4] (Figure 1) from runway 16R and to climb to 5,000 ft.
The DEENA 7 SID required an aircraft to turn right as soon as practicable after take-off, towards the DUNES waypoint[5] and then turn left to track 152° towards the DEENA waypoint. The aircraft was required to have passed DEENA and climbed above 6,000 ft prior to turning right towards the ANKUB waypoint. If the aircraft had not reached 6,000 ft at DEENA, there was a requirement to continue on a heading of 152° until passing an altitude of 6,000 ft, before turning towards ANKUB.
Passing 1,500 ft, the flight crew contacted the departure controller (Departures) and advised them that they were a heavy aircraft[6] on climb to 5,000 ft, departing via the DEENA 7 SID. Departures advised the flight crew the aircraft was identified on radar and instructed them to climb via the SID to flight level (FL) 280.[7]
Figure 1: DEENA SEVEN standard instrument departure (SID) from runway 16R
Source: Airservices Australia, annotated by ATSB
At approximately 1511, and with 6.3 NM spacing behind BA16, QF926 departed from runway 16R, also cleared on a DEENA 7 SID. During the initial climb, the flight crew contacted Departures advising that they were a heavy aircraft, passing 1,500 ft on climb to 5,000 ft, cleared on a DEENA 7 SID. Departures subsequently cleared them to climb to FL 280 via the SID.
BA16 climbed through 6,000 ft at around 25 km from Sydney Airport and initiated a turn to ANKUB in accordance with the SID. QF926 passed DEENA approximately coincident with climbing through 6,000 ft and initiated a turn to ANKUB at approximately 20 km from the airport, also in accordance with the SID (Figure 2).
Figure 2: Flight tracks of both aircraft during their departure from Sydney
Qantas Q926 is depicted in orange and BA16 is depicted in green.
Source: Google Earth with Flight Radar 24 tracks and annotated by ATSB
As QF926 was turning, the controller detected that the aircraft had climbed faster than they had anticipated and instructed QF926 to stop their climb at 9,000 ft, to which the flight crew advised they would do their best. The controller then instructed BA16 to expedite their climb through 10,000 ft.
The controller subsequently advised the flight crew of QF926 that there was a 787 above their aircraft, and they would step climb their aircraft underneath the 787. The Qantas flight crew advised they had sighted the higher aircraft.
There was a loss of separation standards (see the section titled Required separation) between the two aircraft with the minimum vertical separation reducing to 600 ft and lateral separation reducing to 2.4 NM.
The flight crew in BA16 later advised that they had received a traffic alert and collision avoidance system (TCAS)[8] traffic advisory[9] during the event and the first officer subsequently visually identified the A330. They also advised they were informed by air traffic control of the traffic, however this was not recorded on the departures frequency.
The controller had worked as a controller from 2008 and had moved to Sydney in 2015 where they had qualified in both the Sydney Approach Director and Departures positions. While they mainly worked in the Approach Director position, they were rostered in the Departures position regularly to remain current in that role.
They had conducted compromised separation training in their last departures refresher training session in June 2022.
The controller advised that they expected the A330 would have a comparative climb performance to the 787. Hence, they instructed them to follow the 787. Qantas typically utilised the A330 on international routes, however, more recently had been utilising the A330 on domestic routes, including Sydney to Cairns, with correspondingly lower fuel loads and higher climb performance.
The controller then proceeded to assess other traffic in the area. Specifically, they were assessing a track for an aircraft, on descent from FL 280 to Shellharbour to ensure separation between this aircraft and an Airbus A380, which was in the list to depart runway 16R. They were also assessing the departure tracks for other aircraft due to depart from runway 16L and coordinating a media helicopter, overflying the airspace at 500 ft, with the Bankstown Airport tower controller. The controller advised they considered their workload to be manageable at the time.
At the time, auto-release departures were in progress at Sydney Airport. This procedure allowed the tower controller (Tower) to depart aircraft without prior coordination with the departures controller (Departures). Departures had a list of aircraft on their console which were due to depart. These aircraft were listed in order of departure from the runway they were using, but the Tower controller could depart the aircraft from either runway in the order which allowed best use of the runways.
Tower was required to ensure there was a minimum separation between the aircraft of 5 NM when aircraft were departing from runway 16R. When using the DEENA 7 SID, Tower cleared the aircraft to climb to 5,000 ft via the SID, this ensured that departing aircraft continued on a heading of 152° and would not initiate a turn unless they received a further clearance from Departures.
The required separation standards at Sydney are specified in the manual of air traffic services (MATS). The manual specified that the separation standard in the Sydney terminal control unit (TCU) was 3 NM lateral or 1,000 ft vertical separation. However, the wake turbulence standards between 2 heavy aircraft, required a minimum of 4 NM separation where aircraft were departing using the same runway, which was the case for this departure.
The A330 departed with the required spacing behind the preceding B787.
The controller advised they did not receive a short-term conflict alert (STCA) on their console during the event. A replay of the recorded surveillance data indicated the STCA was displayed on a number of occasions. However, Airservices advised that the replay was not a reproduction of the controller’s screen at the time. The parameters for a STCA in the TCU environment are that within the following 60 seconds the aircraft will infringe 2.1 NM lateral separation and or 600 ft vertical separation. In this case, as the separation reduced to 600 ft and 2.4 NM in a turn, it is possible that due to the dynamics of the event, the STCA may not have shown on the controller’s console. However, the ATSB was unable to determine whether the controller received a STCA on their console.
According to MATS, where a controller becomes ‘aware that an aircraft is in a situation that places it is unsafe proximity to…other aircraft’, the controller should issue a ‘safety alert’. They should also use the term ‘avoiding action’ prior to instructions when in the controller’s judgement, the aircraft ‘is in a situation that places it at risk of a collision with another aircraft under surveillance’.
Airservices Australia advised that in response to the replanning of the airspace in the Sydney area due to the establishment of the Western Sydney International (Nancy-Bird Walton) Airport, which is due to open in 2026, the DEENA 7 SID has been redesigned.
In the last 10 years, across Australia, there have been 8 occurrences of a loss of separation reported to the ATSB involving aircraft cleared on a SID where a following aircraft has climbed faster than the preceding aircraft.
Of these, 6 occurrences were at Sydney Airport and 5 of these involved the DEENA 7 SID. Of these, 1 occurred in 2012, 1 in 2019, 1 in 2020, and 2 in 2022.
During the departure of two heavy aircraft conducting the DEENA SEVEN standard instrument departure (SID), the controller assessed that the following Airbus A330 would have a similar climb performance to the leading Boeing 787, without considering that the A330 was conducting a domestic flight and would therefore have a significantly lower fuel load and better climb performance than the preceding heavily‑loaded 787. The controller cleared both aircraft, in sequence, to climb to the same level. The controller then became distracted, planning the separation between 2 other aircraft and did not detect the variation in climb performance between the departing A330 and 787.
As the actual climb performance of the A330, on a domestic route, was greater than the climb performance of the 787 on an international route, the separation reduced. When the controller detected the closing aircraft, they instructed both flight crew to take action to increase the separation between their aircraft. During the occurrence, it is likely the controller did not receive a short-term conflict alert (STCA) warning however, they did suspect there had been loss of separation and did not provide a safety alert or advise that the instruction was an avoiding action.
The use of SIDs ‘enable the safe and efficient processing of instrument flight rules[11] aircraft … from airports’ (Airservices Australia) and will ‘deconflict potentially conflicting traffic by the use of specific routings, levels, speed restrictions and check points’ (Skybrary). They are particularly useful in high traffic airspace such as departing Sydney Airport. However, according to Airservices Australia, SIDs do not provide longitudinal separation between aircraft which are following in trail with another aircraft, with controller action ensuring the maintenance of separation.
Despite this, the design of the DEENA SEVEN SID (and possibly others) did not provide a positive method of providing lateral separation assurance to departing aircraft with differing climb performance. As the aircraft had to satisfy 2 separate conditions prior to turning, there was no way of ensuring aircraft would turn at the same distance from the airport. As such, lateral separation could not be assured.
Airservices Australia advised that the DEENA SEVEN SID had been redesigned to remove the conditional requirements of the procedure. At the time of writing, the change had been approved and was planned to be released in the first implementation package for the Western Sydney International (Nancy-Bird Walton) Airport project. However, no timeframe for the release of the package was provided.
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of separation involving Airbus A330, VH-EBK, and Boeing 787, G-ZBKF near Sydney Airport, New South Wales on 28 September 2022.
When clearing two aircraft on the DEENA 7 standard instrument departure, the controller incorrectly assessed that they would have similar climb performance and became distracted and did not detect the relatively higher climb performance of the departing Airbus A330 aircraft. This resulted in the A330 turning inside the preceding Boeing 787 and a loss of separation standards with that aircraft.
The DEENA 7 standard instrument departure has no designed positive separation assurance method, making it susceptible to loss of separation occurrences. (Safety issue)
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
DEENA 7 Standard instrument departure had no positive separation assurance method
Safety issue description: The DEENA 7 standard instrument departure has no designed positive separation method, making it susceptible to loss of separation occurrences.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Involved air traffic controller
Airservices Australia
Civil Aviation Safety Authority
Qantas
Air Accidents Investigation Branch, United Kingdom
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Automatic terminal information service (ATIS): continuous broadcast of recorded aeronautical information. ATIS broadcasts contain essential information, such as current weather information, active runways, available approaches, and any other information required by flight crew.
[2] Simultaneous independent departures are simultaneous departures for aircraft departing in the same direction from parallel runways.
[3] Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
[4] Standard instrument departure (SID): an air traffic control (ATC) defined procedure, that simplifies departure tracking while also balancing terrain/obstacle avoidance, noise abatement and airspace management considerations.
[5] Waypoint: A defined position of latitude and longitude coordinates, primarily used for navigation.
[6] Wake turbulence separation is determined by aircraft maximum take-off weight. Aircraft with a maximum take-off weight of 136,000 kg or greater are categorised as heavy aircraft.
[7] Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 280 equates to 28,000 ft.
[8] Traffic alert and collision avoidance system (TCAS): a type of airborne collision avoidance system (ACAS).
[9] Traffic advisory (TA): an alert issued by an airborne collision avoidance system (ACAS) when the detected traffic may result in a conflict. Pilots are expected to initiate a visual search for the traffic causing the TA.
[10] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky
[11] Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR).
Occurrence summary
Investigation number
AO-2022-047
Occurrence date
28/09/2022
Location
near Sydney Airport
State
New South Wales
Report release date
03/03/2023
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Loss of separation
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Airbus
Model
A330-202
Registration
VH-EBK
Serial number
0945
Aircraft operator
Qantas Airways
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 22 January 2020, a Boeing 777 was being operated by United Airlines as regular public transport flight UA870 from Sydney, Australia to San Francisco, United States.
At about the same time, a GIE Avions de Transport Régional ATR 72 was being operated by Virgin Australia as regular public transport flight VOZ1153 from Sydney to Tamworth, New South Wales.
Sydney Airport was configured for parallel runway operations, including simultaneous independent departures. VOZ1153 departed from runway 34R to an assigned heading of 350º, just prior to UA870 departing from runway 34L. UA870 was required to maintain runway heading (335º) until reaching 1,500 ft, at which point the aircraft was cleared to turn left and track towards Richmond, northwest of Sydney. However, UA870 climbed straight ahead through to about 2,100 ft and then the aircraft turned to the right about 45º from the required heading, resulting in a loss of separation with VOZ1153. At their closest point of approach, the two aircraft were separated by 1,843 m (about 1.0 NM) laterally and 60 m (about 200 ft) vertically.
Air traffic control detected the loss of separation and issued interventional instructions to both aircraft. The required separation was re-established and both flights continued without further incident.
What the ATSB found
The ATSB found that the UA870 pilot flying was expecting a more simplistic procedure often provided to foreign crew departing Sydney for an oceanic route. The pilot flying then became confused regarding aspects of the flight management computer (FMC) coding generated to represent the actual departure clearance provided. This may have been due to an unfamiliarity with radar transitions from a standard instrument departure to an en route track. This led the pilot flying to incorrectly adjust the FMC prior to engine start, and resulted in the aircraft turning right after departure, bringing it into conflict with VOZ1153.
The pilot flying probably did not effectively communicate the changes made to the FMC to the crew. The FMC departure specific coding was also not effectively cross-checked by the pilot monitoring or relief pilots prior to take-off.
Safety message
The ATSB’s SafetyWatch program highlights broad safety concerns that come out of ATSB investigation findings and from the occurrence data reports by industry. One of these safety concerns is data input errors.
This occurrence illustrates the importance of procedural correctness, effective communication and crew coordination towards the conduct of safe flight operations. Any amendment to the flight management computer, particularly those applicable to the more critical phases of flight (departure and arrival procedures) should always be announced, and then carefully and independently verified by at least one other crew member. The incident also outlines that, when possible, air traffic controllers can potentially further assist foreign crew by proactively factoring the crew’s unfamiliarity when providing airways clearances.
Crew details
United Airlines 870
Captain
Senior FO
Observer 1 (FO)
Observer 2 (FO)
Total Flight hours
21,072
19,000
17,600
14,200
Flight hours on B777
4,309
3,500
2,500
2,600
Flight hours in last 90 days
166
350
175
148
Total instrument hours
11,000
18,500
500
Not available
Instrument hours last 90 days
100
350
3
Not available
Medical
Class 1
Class 1
Class 1
Class 1
Last simulator check*
13 Dec 2019
21 Aug 2019
28 Jun 2019
20 Jun 2020
*Note: In United Airlines, crew resource management (CRM) and threat and error management (TEM) is incorporated into training and evaluation events, or simulator checking activities.
The investigation
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, a limited-scope, fact-gathering investigation was conducted in order to produce a short summary report, and allow for greater industry awareness of findings that affect safety and possible safety actions.
The occurrence
On the early afternoon of 22 January 2020, a Boeing 777-300ER (777), registered N2333U, was being operated by United Airlines as regular public transport flight UA870 from Sydney, New South Wales to San Francisco, United States.
At about the same time, a GIE Avions de Transport Régional ATR 72-600 (ATR72), registered VH-FVQ, was being operated by Virgin Australia as regular public transport flight VOZ1153 from Sydney to Tamworth, New South Wales.
The Sydney Airport automatic terminal information service (ATIS)[1] indicated to all crews that parallel runway operations were in progress, including simultaneous independent departures[2] from runways 34L and 34R. The weather was fine, with excellent visibility, no cloud below 10,000 ft and a light wind from the northwest.
The flight crew for flight UA870 consisted of a captain and three first officers. The captain was the pilot flying (PF) and one of the first officers was the pilot monitoring (PM).[3] The remaining first officers occupied the two observers’ seats positioned directly behind the PF and PM on the flight deck.
Sydney air traffic control attempt to facilitate expeditious departures to all aircraft, particularly aircraft transiting over extended distances (oceanic crossings). This regularly involves a clearance via the SYDNEY ONE RADAR (SYD1) standard instrument departure (SID).[4] The PF had operated from Sydney Airport on a number of other occasions. While preparing for departure at the gate, after receiving the ATIS, but prior to receiving their pre-departure clearance, the PF configured the flight management computer (FMC)[5] for the SYD1 based on an expectation from prior experience.
At about 1330 Eastern Summer Time (ESuT),[6] Sydney clearance delivery (SCD) air traffic control (ATC) provided a different pre-departure clearance via VHF radio:
United eight seventy (UA870), delivery, cleared to San Francisco via DIPSO,[7] flight planned route, runway three four left (34L), Richmond five departure, radar transition, climb via SID to five thousand (5,000)…
The PM provided a truncated read back of the clearance to ATC, inadvertently not repeating the radar transition[8] component.
At the same time as the UA870 crew were preparing for their departure, VOZ1153 was cleared to depart via the SYD1 radar SID via runway 34R. This procedure required the ATR72 to maintain a heading of 350º after take-off, until directed otherwise by ATC.
The UA870 crew reviewed the RICHMOND FIVE (RIC5) SID chart (Figure 1). That chart included two distinct caution notes about the initial climb. The more detailed caution stated:
Parallel runway operations - DO NOT TURN RIGHT. Track 335⁰. At 1500 [ft] turn LEFT, track direct RIC NDB [Richmond], then follow transition instruction.
Figure 1: RICHMOND 5 Standard Instrument Departure (SID) from runway 34L
Source: Jeppesen (via United Airlines flight safety). Annotated by the ATSB.
The PF then re-programmed the FMC, replacing the SYD1 procedure with the RIC5. At this point, the PF reported being unsure regarding the coding specific to the two transition options (radar or Richmond) presented by the FMC.
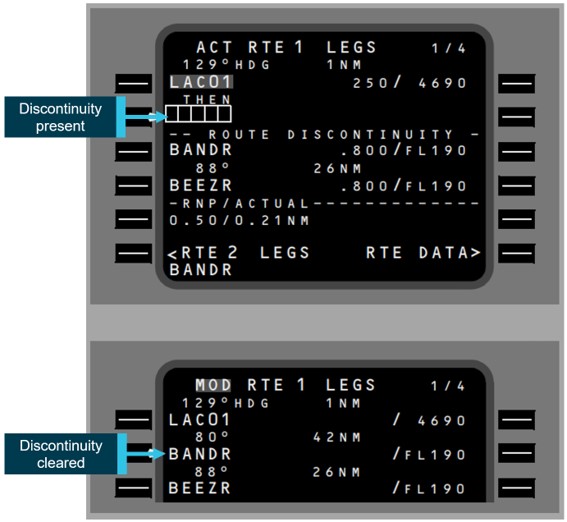
The radar transition option in the FMC included a deliberate discontinuity[9] (gap) in the waypoint[10] sequence (coding). The discontinuity represented the point where air traffic control would provide radar vectors to facilitate a re-join to the oceanic track (to San Francisco) after the aircraft passed 12 NM from Sydney (see Figure 1).
The PF then closed (removed) the discontinuity.[11] In effect, the PF had removed the pre-programmed radar transition procedure, which meant that after the 1,500 ft left turn, the next waypoint on the route was DIPSO, not 12 NM Sydney. The PF recalled communicating removing the discontinuity to the PM, but it was not acknowledged by the PM. The PM did not recall hearing about the coding change.
Later in the pre-departure preparation, the PM reported verifying the new departure in the FMC using the summary route (RTE) page. However, the PM did not review it using the more detailed LEGS page (see Flight management computer discontinuities).
While taxiing to the runway for take-off, the PM recalled that when completing the departure review[12] with the PF, they noted the FMC RTE page read:
Runway 34L, Richmond Five (RIC5), no transition
At 1421:41 the tower controller for runway 34R cleared VOZ1153 for take-off, and 42 seconds later, the tower controller for runway 34L cleared UA870 for take-off.
At 1422:29, VOZ1153 departed runway 34R. About 35 seconds later, as VOZ1153 was climbing through 1,500 ft, UA870 departed runway 34L. (The runway 34L threshold is about 1,000 m north [ahead] of the runway 34R threshold [see Figure 1].)
At about 1424:06, climbing through 1,417 ft, the UA870 crew were instructed to contact Sydney departures control.
At 1424:33, as UA870 was climbing through 2,120 ft, the Sydney departures controller detected that the aircraft was turning right and instructed the crew to immediately turn left, to a heading of 270°. The flight crew had also identified the incorrect turn to the right. The departures controller then issued a separate interventional instruction to VOZ1153 to turn right immediately, to a heading of 090°.
On receiving their instruction, the two UA870 pilots in the observers’ seats identified the traffic (VOZ1153) visually (right-hand observer) and via the traffic alert and collision avoidance system (TCAS)[13] display (left-hand observer).
Recorded flight data showed that the UA870 autopilot was disengaged about 3 seconds after the interventional instruction to UA870 was received, at an altitude of 2,160 ft. Due to the momentum of the 777, the aircraft continued turning right through a further 5 degrees to heading 018º, prior to the PF manually reversing the turn back to the left. The minimum distance between the two aircraft was 1.0 NM laterally and 200 ft vertically (Figure 2).
Both aircraft continued flight to their respective destinations without further incident.
Figure 2: Aircraft tracks showing closest point of approach
Source: Google Earth overlaid with United Airlines and Virgin Australia data. Annotated by the ATSB.
Context
Flight crew
The flight crew of UA870 was augmented[14] with two cruise in-flight relief pilots (also first officers), due to the duration of the flight and the operator’s flight crew fatigue management framework. Neither the PM or PF reported being fatigued or tired at the time of the incident. Both relief pilots reported minor tiredness at the time of the incident. All the flight crew reported having achieved two separate periods of sleep during their layover in Sydney. UA870 flight crew experience is summarised in General details.
Transition routes
SIDs are designed to allow pilots to navigate away from an airport with minimal radio communication with ATC (departures control). Charted transition routes facilitate the transition from the end of a basic SID to a location in the en route airways structure. In this case, the radar transition allowed for UA870 to join their route to San Francisco at waypoint DIPSO after departing Sydney via the RIC5 procedure.
Normally a transition route includes a course, altitude requirements and distances between waypoints along the transition. Some SIDs have multiple transitions. The Richmond 5 SID had two transition routes.
The radar transition segment relied on the Sydney departures controller providing radar vectors for the aircraft to follow back to the east, after the aircraft passed the ‘12 NM Sydney’ point, but prior to Richmond. The aircraft would then re-join their flight planned (oceanic) route to San Francisco. In the event that a radar vector was not provided by 12 NM northwest of Sydney, the autopilot would simply maintain the aircraft’s heading from that point, until a vector was provided to the crew, or the crew amended the FMC route. The procedure required the aircraft track to initially track to the west to allow for separation with aircraft departing simultaneously from the parallel runway (34R).
The presence of a route discontinuity is unusual in a departure or arrival procedure, but it serves to highlight to the flight crew that at the point of discontinuity, a further clearance or direction is required from ATC.
Flight management computer discontinuities
The PF uploaded the flight plan to the FMC via satellite datalink. Procedurally, the crew (usually the PF), then manually entered the SID based on the departure clearance provided, which is contained within the FMC memory.[15] The majority of procedural SIDs could then be joined to the uploaded route by removing the discontinuity created between the end waypoint defining the departure procedure and the first waypoint of the main route to their destination. This was the normal process dictated by the operator’s procedures, where it was emphasised that for most departures the remaining FMC discontinuities should be rectified (removed) using the FMC legs (LEGS) page (Figure 3).
Guidance was also provided that this should not be completed in isolation from the rest of the crew.
The PF reported some confusion with the coding specific to the radar transition component of the RIC5 SID. That is, misunderstanding the necessity for the pre-programmed discontinuity as it was depicted by the FMC, which represented the radar transition segment during which ATC would provide radar vectors.
A discontinuity can be viewed by either the FMC LEGS page or route (RTE) page. The RTE page is a summary page generated displaying significant waypoints and airways (routes) that, in sequence, define the coded route the aircraft is programmed to fly via either the autopilot, if engaged or the flight director, if flying manually. The RTE page does not contain the same level of detail contained via the FMC LEGS page (Figure 3).
The operator’s supplementary procedures regarding the FMC setup prior to departure also included the following warning:
Do not use the RTE page to repair discontinuities resulting from SID entries. Critical changes in departure ground track may result.
Figure 3: Example of a route discontinuity displayed via the B777 FMC LEGS page
Source: Boeing B777 supplementary procedures (via United Airlines)
United Airlines procedures
The operator’s procedural documentation included guidance and direction specific to departure preparation. They detailed the PF and PM tasks and responsibilities, including the requirement to conduct a pre-departure briefing. The crew were also required to conduct a comprehensive departure review, immediately prior to take-off, which included a final confirmation of the FMC departure route setup. These procedures highlighted the importance of verbalisation, independent review and cross-checking.
The operator also provided guidance specific to Sydney Airport departures, including tailored charts illustrating the RIC5 SID (detailing the radar transition procedure), specifically the requirement to not turn right.
The operator’s procedures also mandated that relief pilots were to remain at their designated stations (observer’s seats) on the flight deck from the commencement of the departure briefing until the aircraft was above flight level 180.[16] More generally, a number of important support duties were also defined for relief pilots including active participation in crew briefings (departure briefing and review) and a specific requirement to ensure compliance with clearances.
Air traffic control information
Separation standards[17] are used by air traffic controllers to manage air traffic safely. They refer to the minimum horizontal and/or vertical distance, or time apart, that aircraft operating in controlled airspace must maintain. When the separation between two or more aircraft is less than the standard, there is a loss of separation.
A surveillance separation standard is used when aircraft position information is derived from air traffic services’ surveillance systems (including radar). When aircraft are operating inside terminal area airspace, such as Sydney, controllers must maintain a minimum separation between aircraft of 3 NM (5.6 km) laterally or 1,000 ft vertically.
A runway separation standard is applied for aircraft taking off from parallel runways. Following take-off, separation is facilitated visually until a surveillance (radar) or vertical separation standard exists. Aerodrome controllers (ADCs) may reduce the radar separation minima in the vicinity of aerodromes when adequate separation can be provided using visual observation and each aircraft is continuously visible to the ADC. However, ADCs are not permitted to provide visual separation if the projected flight paths of the aircraft conflict.
When a significant loss of separation occurs, air traffic control is required to issue a safety alert[18] to notify pilots of information that is of a time-sensitive and safety-critical nature. It is important pilots understand the critical nature of these instructions and respond in a timely manner to ensure the safe conduct of flight.[19]
Traffic alert and collision avoidance system
Modern high-capacity transport aircraft such as the 777 and ATR72 are required to be equipped with an advanced traffic alert and collision avoidance system (TCAS).[20] TCAS is designed to prevent mid-air collisions between aircraft. TCAS operates independently of ATC by using on-board surveillance capability to detect other transponder-equipped traffic and provides:
Traffic display (proximate traffic) and traffic advisories (TA) for situational awareness of relatively close aircraft
Resolution advisories (RA) for very close aircraft with vertical guidance to resolve the threat.
Both TA and RA are generated based on the projected closest point of approach (CPA) or miss distance and the time to co-altitude (TAU). In general, the thresholds (time and distance) for CPA and TAU increase as altitude increases.
All RA are inhibited when below 1,000 ft (+/- 100) above ground level (AGL) and all TCAS aural alerts are inhibited when below 500 ft (+/- 100).[21] This is to ensure that alerts are not generated during the initial take-off climb for two reasons: to avoid distracting the crew and, because the aircraft is already flying close to the performance limit (body angle/attitude and thrust).
Safety analysis
Flight management computer – departure setup
The foreign captain was expecting to receive a clearance via the SYD1 standard instrument departure and had pre-programmed the FMC in anticipation of this and briefed the other crew accordingly. However, the pre-departure clearance provided by air traffic control was different (RIC5). This was likely due to the captain’s limited exposure to the varying Sydney-centric departure procedures (SYD1 versus RIC5). In addition, the clearance included the radar transition procedure, with which the captain was unfamiliar, due to the predominant use of procedural-based transitions in the United States. Anything non-standard in departures or arrivals can add additional complexity, but particularly for crew that have very limited experience with the location, such as long-haul foreign crew. Air traffic controllers have an opportunity to take into account the likelihood of a crew’s familiarity with the airport when issuing clearances to foreign crew.
The clearance meant the FMC needed to be re-programmed for the RIC5 procedure. During this process, the PF removed the discontinuity that was automatically generated in the FMC flight path, that is, the waypoint sequence to the cleared oceanic route. This would have been appropriate for many procedural transitions but not for a radar transition. The predominance of procedural transitions in the United States likely meant that the PF was focussed on removing the discontinuity (gap) in the FMC coding.
In this case, the purpose of the discontinuity was to represent controller-issued vectors as the aircraft tracked beyond 12 NM northwest of Sydney. In effect, the aircraft was cleared to 12 NM. From that point they were required to wait for a controller initiated radar vector to re-join their cleared oceanic route to San Francisco commencing at waypoint DIPSO (to the east). In removing the discontinuity, the aircraft was re-programmed to track directly to DIPSO after reaching the initial waypoint at 1,500 ft where the aircraft should have turned left (before they reached the 12 NM point). Ultimately, this resulted in a right turn and, therefore, the loss of separation.
Crew coordination
Effective crew coordination is fundamentally dependent upon effective communication. In order for cockpit crew members to share a ‘mental model’, or common understanding of the nature of events relevant to the safety and efficiency of the flight, communication is critical.[22] The operator’s procedures were clear and provided an established framework for the flight crew to communicate and coordinate their activities to ensure a safe and expeditious departure.
A number of opportunities existed not only for the PM, but also the crew positioned in the observers’ seats (in-flight relief pilots), to verify the FMC setup between the departure briefing and entering the runway prior to take-off. The operator’s procedures included a comprehensive process by which crew use different pages (information sources) within the FMC to ensure the departure clearance is reflected accurately by the computer coding (waypoint sequence).
The PM was not aware of the amendment to the radar transition (deletion of the route discontinuity), which indicated that the PF may not have clearly verbalised the change and/or ensured the PM heard and understood the change, in accordance with the operator’s procedures. By not clearly verbalising this misunderstanding or the amendments to the departure route setup, the PF did not provide an opportunity for the rest of the crew to contribute effectively.
However, there were further opportunities for the PM or relief pilots to discover this error. The PM verified the FMC set up, but only used the summary RTE page rather than the LEGS page with greater detail, and therefore the waypoint sequencing error was not detected. Further, in the departure review just before take-off, both the PF and the PM noticed the ‘no transition’ on the FMC RTE page, but no-one recognised this was not in accordance with the radar transition segment of the clearance.
Communication
Effective communications also includes with external sources such as air traffic control. Readbacks of clearances and instructions to crew in the aviation context serves two main purposes; acknowledgement of both the intent and content of the clearance, and to reinforce the message has been acknowledged and understood. In this case, the PM provided a truncated readback to ATC, which did not provide this assurance. The truncated readback was not challenged by the controller. As such, the controller did not have any assurance that the flight crew heard and understood that they were cleared for a radar transition. This increased the risk of errors to the FMC setup and could have led to further confusion during the initial climb.
Findings
Contributing factors
The pilot flying incorrectly amended the flight management computer (FMC) for the cleared departure.
The amended FMC setup was probably not effectively communicated to the crew or effectively cross-checked by the pilot monitoring or relief pilots.
Other factors increasing risk
The pilot monitoring did not complete a full readback of the radar transition component of the pre-departure clearance, nor did the Sydney clearance delivery controller insist on a full readback.
Other findings
The Sydney departures controller observed UA870 turning right and towards VOZ1153 and quickly issued unambiguous and immediate instructions to both aircraft to rectify the situation and re-establish the required separation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Sequence of events
On the night of 5 August 2019, at 1831:45 Eastern Standard Time[1], an Airbus A330-300 (A330) aircraft, registered VH-EBJ and operated by Qantas Airways, was cleared by air traffic control (ATC) for take-off from runway 34 right (34R) at Sydney Airport, New South Wales. At that time, a Boeing 737-800 (737) aircraft, registered VH‑VZO and operated by Qantas Airways, was on final approach to the same runway.
A trainee controller was operating the Sydney aerodrome controller east (ADC-E) ATC position, under the supervision of an on-the-job training instructor (OJTI).
The ADC-E controller assessed that there would be insufficient runway spacing between the aircraft and instructed the 737 flight crew to ‘go around’. As the 737 flight crew conducted the missed approach, a loss of separation occurred between their aircraft and the departing A330. Flight data showed that separation between the aircraft reduced to about 0.43 NM laterally and about 500 ft vertically (Figure 1).
Figure 1: A330 and 737 flight paths and indication of the area of minimum separation
Source: Google earth overlaid with Qantas Airways flight data. Annotated by ATSB
The ADC-E controller reported that he had both aircraft in sight. In an attempt to increase separation between the two aircraft, he instructed the 737 flight crew to turn further right. The 737 was then at about 980 ft, which was below the minimum vectoring altitude (at night). As both aircraft converged, the A330 flight crew received a traffic advisory alert from their aircraft’s airborne collision avoidance system (ACAS). The A330 first officer, who was pilot flying,[2] then saw the 737 in close proximity and, in response, reduced the aircraft’s angle of bank to reduce the turn towards the 737. The captain of the A330 made a radio transmission to advise the ADC-E controller that it was ‘very close’. The controller then issued an instruction to the A330 flight crew to turn left.
The A330 climbed to 5,000 ft and continued to Melbourne without further incident. The 737 climbed to 3,000 ft and was issued radar vectors for a second approach to runway 34R. It landed without further incident a short time later.
Table 1 provides a more detailed summary of the sequence of events.
Table 1: Summary of key events
Time
Event
1831:04
The ADC-E instructed the A330 flight crew to line up runway 34R. The 737 was on final approach at about 2.8 NM.
1831:10
The ADC-E instructed the 737 flight crew to maintain minimum speed. The 737 flight crew responded that they were already at minimum speed.
1831:21
The ADC-E instructed the A330 to expedite lining up and to be ready for an immediate take-off. The ADC‑E was waiting for a turboprop aircraft, which had just landed on runway 34R, to taxi clear of the runway.
1831:45
Once the turboprop aircraft was clear of runway 34R, ADC-E cleared the A330 for immediate take-off.
1831:58
The ADC-E assessed that the runway separation standard would not be maintained at the time the 737 crossed the threshold of runway 34R. He instructed the 737 flight crew to go around. The A330 was still in its take-off roll and the 737 was at about 400 ft.
1832:30
The 737 was climbing through about 920 ft still on runway track (335°). The A330 was becoming airborne on runway track (335°).
1832:38
The ADC-E instructed the 737 flight crew to turn right onto heading 100°. Flight data showed the 737 flight crew commenced the right turn when passing about 1,300 ft AGL. At that time the aircraft was approximately 1,500 m north of the runway threshold. The A330 was in a climbing right turn tracking on the MARUB 6 standard instrument departure. The projected flight paths of the two aircraft were then converging.
1832:50
The A330 flight crew received an ACAS traffic advisory alert (‘TRAFFIC TRAFFIC’). The A330 first officer looked out the right cockpit window and sighted the 737 above in a climbing turn and in close proximity.
1833:03
The ADC-E instructed the 737 flight crew to turn further right onto heading 120°.
1833:09
The ADC-E instructed the 737 flight crew to climb to 3,000 ft.
1833:17
The A330 captain made a radio transmission saying ‘that was very close’.
1833:23
The ADC-E instructed the A330 to turn left heading 100°. Both aircraft were then on diverging flight paths.
Standard instrument departures and approaches
Standard instrument departures (SIDs) and instrument approaches are charted procedures that flight crews must follow when departing or landing at suitably equipped aerodromes.
ATC had cleared the A330 flight crew to depart from runway 34R on the MARUB 6 SID (Figure 2). The design of that SID required flight crew to climb on the runway track (335°) to 500 ft and then turn right to intercept the 075° track to waypoint MARUB.
Figure 2: MARUB 6 standard instrument departure from runway 34R
Source: Qantas Airways
Prior to descent into Sydney, ATC had cleared the 737 flight crew to conduct a global navigation satellite system landing system (GLS) approach to runway 34R. In the event of a go-around, Airservices Aeronautical Information Publication Australia (AIP) 2.14.2 (Go Around and Missed Approach Procedure in VMC) stated that at Sydney visual go-arounds must be carried out in accordance with the GLS or instrument landing system (ILS) missed approach procedure for the runway the aircraft was using, or as directed by ATC.
When the ADC-E instructed the 737 flight crew to go around, the aircraft was descending through about 400 ft. The missed approach procedure for the GLS runway 34R required the flight crew to maintain the runway track (335°) until 600 ft and then turn right, track 070° and climb to 2,000 ft (Figure 3). Flight data showed the 737 flight crew commenced the right turn when climbing through about 1,300 ft AGL (above ground level). At that time the aircraft was approximately 1,500 m north of the runway threshold.
A missed approach procedure is designed for each instrument approach to provide aircraft with terrain and obstacle clearance during a go-around. A missed approach point (MAP) is a point where flight crew must initiate a missed approach if suitable visual references are not available to make a safe landing or the aeroplane is not in a position to make a safe landing.
For ILS and GLS approaches, the decision height (DA) in conjunction with the glide slope (G/S) is used to determine the MAP. The DA and MAP are annotated on the approach chart (Figure 3).
From the MAP, flight crews are required to navigate their aircraft in accordance with the applicable published missed approach procedure unless directed otherwise by ATC.
Figure 3: GLS approach runway 34R
Source: Qantas Airways annotated by ATSB
The MARUB 6 SID runway 34R and the missed approach flight path for the GLS approach runway 34R both required flight crew to make an early right turn and track to the east of Sydney Airport.
As in this occurrence, should an aircraft be departing on the MARUB 6 SID at the same time an aircraft conducts a go-around from runway 34R, both aircraft will track out to the east. There is potential that those flight paths will conflict and require intervention from ATC in order to ensure separation is maintained between the aircraft.
Aircraft flight management systems
Modern commercial aircraft are generally fitted with a flight management system (FMS) or similar system. A FMS uses a variety of sensors to determine the aircraft’s current position and then sends guidance commands to the aircraft control systems to navigate it along the flight path programmed by the flight crew.
An FMS has a worldwide navigation database that is coded with published instrument procedures including missed approach procedures. The navigation database allows an FMS to create a continuous display of navigational data to flight crew. Vertical navigation guidance can also be coded and displayed. Any discrepancies in a navigation database may lead to flight crew not following the correct flight path.
Air traffic control information
Separation standards refer to the minimum distance or time apart that aircraft operating in controlled airspace and at Class C[3] airports must be kept. These are outlined in the Manual of Standards for Air Traffic Services and air traffic controllers use them to safely manage air traffic.
Air traffic controllers must keep aircraft separated vertically or horizontally. When the separation between two or more aircraft is less than the standard, there is a loss of separation.
A surveillance separation standard is used when aircraft position information is derived from air traffic services’ surveillance systems (including radar). When aircraft are operating inside terminal area airspace, such as Sydney, controllers must maintain a minimum separation between aircraft of 3 NM laterally or 1,000 ft vertically. That standard of separation may be reduced by a tower controller when using visual observation.
A runway separation standard is applied for aircraft landing and taking off from the same runway. The standards required that an aircraft landing behind a departing aircraft cannot cross the runway threshold until the preceding aircraft is airborne and:
has either commenced a turn, or
is beyond the point on the runway at which a landing aircraft could be expected to complete its landing roll and there is sufficient distance to enable the landing aircraft to manoeuvre safely in the event of a missed approach.
In this case, the ADC-E ensured runway separation standard was not infringed by instructing the 737 flight crew to go-around.
Aerodrome controllers (ADCs) may reduce the radar separation minima in the vicinity of aerodromes when adequate separation can be provided using visual observation and each aircraft is continuously visible to the ADC. However, ADCs are not permitted to provide visual separation if the projected flight paths of the aircraft conflict.
In this case, the ADC-E and his supervising OJTI stated they had the two aircraft sighted and applied visual separation. At night or in instrument meterological conditons, ATC maintains responsibility for terrain clearance when an aircraft is being radar vectored. When the ADC-E issued a radar vector (at night) to the 737, the aircraft was still below the minimum vector altitude, therefore terrain separation was not maintained.
When a loss of separation occurs, compromised separation recovery procedures are required to be applied to reduce the risk of a collision. A controller is required to issue safety alerts to pilots of aircraft as a priority when a controller becomes aware that aircraft are considered to be in an unsafe proximity to each other. In this case, no safety alert was issued by either the ADC-E or OJTI as both controllers considered visual separation existed.
The ADC-E trainee was an experienced controller. He had previously worked as an ADC in another tower and had a surface movement controller rating at Sydney. At the time of the occurrence, he had neared the end of his training for the Sydney ADC-E position, with his performance check to obtain his rating scheduled for the next day. Both the ADC-E and OJTI had completed compromised separation recovery training.
Further investigation
The investigation is continuing and will include examination of:
design and risk assessment of MARUB standard instrument departures and missed approaches from runway 34 right
air traffic control procedures, controller training and controller actions
737 and A330 operator’s procedures and flight crew actions
coding of flight management system navigation databases
further analysis of flight data recordings and ATC recordings.
______________
The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003 and is derived from the initial investigation of the occurrence. Readers are cautioned that new evidence will become available as the investigation progresses that will enhance the ATSB's understanding of the accident as outlined in this preliminary report. As such, no analysis or findings are included in this update.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
At Sydney Airport in the early evening of 5 August 2019, the crews of 3 aircraft were using runway 34R in various phases of flight:
de Havilland Canada Dash 8 operated by QantasLink, nearing the end of the landing approach
Boeing 737 operated by Qantas, on the final segment of an independent visual approach
Airbus A330 operated by Qantas, awaiting instructions and clearance to line up and take off and make a right turn to track to the east via the MARUB SIX standard instrument departure (SID).
This traffic was managed by an aerodrome controller (ADC) position in the Sydney air traffic control tower that was occupied at the time by a controller in the late stages of training for the ADC role under the supervision of an on-the-job-training-instructor (OJTI).
When the Dash 8 had landed and taxied off the runway, the trainee ADC issued a clearance to the A330 crew for an immediate take-off, and they complied. Assessing that there could be insufficient runway separation between the A330 on the take-off roll and the anticipated arrival of the 737 at the runway threshold, the trainee ADC instructed the 737 crew to go around (conduct a missed approach).
The 737 flight crew initiated the missed approach procedure by climbing on the runway heading but climbed through the mandatory turn altitude. The 737 turned when instructed by the trainee ADC. Meanwhile, the A330 followed the SID track by turning right shortly after passing the departure end of the runway, and the two flight paths began to converge.
As the 2 aircraft were turning right and climbing, the A330 flight crew received a traffic alert from the onboard traffic collision advisory system. Shortly after this, the A330 first officer sighted the 737.
As the respective departure and missed approach procedures both involved climbing from a low level and tracking/heading to the east, the aircraft came into close proximity. Nevertheless, the controllers maintained sight of both aircraft throughout the sequence and the risk of a collision was low.
In the absence of compliant methods to separate the aircraft at night, the trainee ADC attempted to establish horizontal separation by instructing the 737 crew to turn onto a heading that was divergent from the A330 outbound track.
In the early stages of the respective procedures, the separation between the aircraft reduced to about 0.42 NM (800 m) laterally and about 508 ft vertically. This was categorised as a loss of separation.
What the ATSB found
The loss of separation and close proximity between the 737 and the A330 was the culmination of a series of events that, individually, would only be minor concerns but collectively resulted in a significant incident.
When the 737 was transferred to the ADC from the approach controller, the spacing between it and the landing Dash 8 ahead was less than permitted without coordination between the controllers. In addition, the 737’s speed during some of the final approach was higher than the approach design specified and the flight crew did not advise the ADC. These factors increased the risk of compromised runway separation and associated go-around.
The trainee ADC’s mental model of the developing traffic situation did not fully account for the effects of the 737’s delayed and relatively wide turn, and they expected the A330’s flight path to be further from the 737. Partly as a result of this, the trainee ADC’s actions were not optimal even though they did reduce the extent of the close proximity between the two aircraft. No safety alert or avoiding action advice was given to either flight crew to notify them of their proximity and thereby increase their situational awareness, particularly that of the 737 flight crew who could not visually sight the A330. The trainee ADC also did not modify the A330’s projected flight path, which would have increased the distance between the aircraft and re-established a separation standard sooner.
The on-the-job training instructor (OJTI) was not confident that runway separation could be achieved between the A330 cleared for take-off and the 737 on final approach or that the turn instructions issued to the 737 in the missed approach were sufficient mitigation. However, the OJTI did not provide effective prompts and did not intervene, mindful that at this point in the training, the trainee ADC was meant to be demonstrating the ability to work without instructor intervention.
The ATSB identified safety issues relating to the management of the MARUB SIX SID and the missed approach procedure for runway 34R directing aircraft onto similar outbound tracks. This could require controller intervention to maintain separation. In daytime, although this was potentially problematic, controllers were permitted to vector the aircraft. At night, however, controllers had no procedural controls to draw upon to separate aircraft in this situation when they were below the minimum vector altitude, and there were no compromised separation training scenarios involving aircraft below this altitude at night.
Furthermore, although these issues were known among Sydney controllers generally and Airservices had identified and addressed similar issues at other airports, those at Sydney remained unaddressed. The ATSB considered that this was partly due to the use of operational risk assessments as a high-level representation of threats and not for specific threat scenarios.
The ATSB also made other findings that were not found to be contributory to the occurrence: the tower shift manager (TSM), in a supervisory role, was fully engaged in a controller function and was not aware of the go-around and development of the compromised separation until after the event; air traffic control transfer after the occurrence; and the location of a relevant navigation waypoint in the 737’s flight management computer was incorrect.
What has been done as a result
In 2020, Airservices conducted a risk assessment on the runway 34R missed approach procedure and the MARUB SIX SID procedure, and on the distances between successive arrivals. Subsequently, Airservices implemented redesigned the missed approach procedures for Sydney’s runway 34R to provide an increased likelihood that distance will be maintained with another aircraft departing on a SID from the same runway. The ATSB urges Airservices to apply its expertise and data to monitor the safety outcomes on an ongoing basis so that the lowest-risk designs can be identified and implemented in the long term.
Additionally, in 2020 Airservices advised that compromised separation scenarios where an aircraft is operating below the minimum vector altitude were to be included into the Sydney tower controller instructor guide at night, and in 2023 Airservices advised that the training program also now included a missed approach with a preceding departure in instrument meteorological conditions. Airservices advised that it was working to have the same scenario during night operations included in the compromised separation recovery simulator training for all capital city towers.
Airservices also conducted several further safety actions including improved risk management processes to address specific threat scenarios, issuing a standardisation directive on spacing for aircraft arrivals, established a focus group to foster an increased understanding of shared risk factors among different operational groups at Sydney, and actions to improve the operational availability of tower shift managers in the supervisory role. All safety issues identified by the ATSB in relation to this occurrence have now been adequately addressed.
Qantas conducted several safety actions relevant to the occurrence including updating the missed approach coding in its 737 flight management computers, incorporated related scenarios into cyclic training sessions, and updated its flight data analysis program to more closely monitor approach speeds and traffic collision avoidance system data.
Safety message
Flight path design principles ensure the safety and protection of aircraft, passengers and crew as well as communities under flight paths. Aircraft mostly fly predictably and consistently along arrival and departure routes that have strategic separation by design. This increases awareness of the traffic situation for both pilots and controllers, reduces the need for human intervention and reduces pilot and controller workload at critical times. Where routes converge, such as at a runway, strategic separation is no longer possible. It is also not possible to provide strategic separation of an aircraft conducting a missed approach with one taking off from the same runway. Nevertheless, routes should still require minimal intervention by air traffic controllers to prevent a loss of separation.
The airspace around Sydney Airport is complex: the use of parallel runways limits the options available for separation assurance, and it can be busy. Controllers are expected to maintain an orderly traffic flow with minimal delays while still safely managing separation. There will be times when controllers misjudge runway separation or flight crews don’t conform to procedures, resulting in the need for a missed approach or other intervention.
Missed approaches generally result in a high flight crew workload, particularly when they are manually flown, and sometimes lead to errors. Non-standard missed approaches and unexpected navigation modes further increase the risk of error.
In this occurrence, a series of individual errors and decisions made by flight crews and controllers gradually reduced margins to a point where the two aircraft came within close proximity. Although events like this are uncommon, they will occur from time to time and systems should be designed to minimise the likelihood of a more serious outcome.
At Sydney Airport in the early evening of 5 August 2019, the crews of 3 aircraft were using runway 34R in various phases of flight:
de Havilland Canada Dash 8 operated by QantasLink, nearing the end of the landing approach
Boeing 737 registered VH-VZO and operated by Qantas, on the final segment of an independent visual approach
Airbus A330 registered VH-EBJ and operated by Qantas, awaiting instructions and clearance to line up and take off and make a right turn to track to the east via the MARUB SIX area navigation (RNAV) standard instrument departure (SID).
The airport was operating with parallel runway operations using a runway configuration of 34L and 34R for arrivals and departures. At the time, there were no other aircraft in the area directly relevant to the occurrence. The Sydney automatic terminal information service broadcast the wind was from 30° at 12 kt with a crosswind of 10 kt. The conditions were clear and it was in the early evening after last light.[1]
The above traffic was managed by air traffic control (ATC) in the Sydney Tower in the ‘aerodrome controller – east’ (ADC) position, responsible for operations using runway 34R and the airspace east of the airport. This position was filled by two people:
a controller who was in the late stages of training for the ADC role and who managed traffic in the vicinity of the airport (trainee ADC)
an on-the-job-training-instructor (OJTI), who was assisting and supervising the trainee ADC, and held the overall responsibility for the provision of safe air traffic services by the ADC position.
When the Dash 8 had landed and taxied off the runway, the trainee ADC issued a clearance to the A330 crew for an immediate take-off, and they complied. Assessing that there could be insufficient runway separation between the A330 on the take-off roll and the anticipated arrival of the 737 at the runway threshold, the trainee ADC instructed the 737 crew to conduct a missed approach.
The 737 flight crew initiated the missed approach procedure by climbing on the runway heading but did not commence the mandatory right turn on passing 600 ft. The 737 turned when instructed by the trainee ADC. Meanwhile, the A330 followed the SID track (MARUB SIX) by turning right shortly after passing the departure end of the runway, and the two flight paths began to converge (Figure 1).
Both aircraft continued turning right and climbing. The A330 flight crew then received an audible traffic collision advisory system (TCAS) alert (‘TRAFFIC TRAFFIC’). The A330 first officer looked out the right rear flight deck window and saw the 737 above in a climbing turn and in close proximity. The aircraft came within about 0.42 NM horizontally and 508 ft vertically, with the two aircraft abeam of each other and turning right.
The trainee ADC issued further instructions to both aircraft. Before the minimum required separation standard was met, but with the separation increasing as the 737 accelerated ahead of the A330, the trainee ADC transferred the 737 to the approach controller.[2]
The first aircraft in the approach and landing sequence for runway 34R was a De Havilland Canada DHC-8 (Dash 8) turboprop aircraft, operated by QantasLink. Its flight crew made contact with Sydney tower (the ADC) at 1827:55.
The second aircraft in the arrival sequence was a Boeing 737, registered VH-VZO, operated by Qantas Airways as scheduled passenger transport flight QF545 from Brisbane, Queensland to Sydney, New South Wales.
The captain was the pilot monitoring (PM)[3] and the FO was pilot flying (PF).
Prior to descent, ATC issued the flight crew with a clearance for the ‘BOREE ONE ALPHA’ area navigation (RNAV) arrival to runway 34R. This standard instrument arrival (STAR) comprised a series of altitude limits and waypoints that diverted aircraft inbound from the north to the east of the airport to fly parallel to the runway in a southerly direction until ATC provided radar vectors to intercept the northerly approach path (335°) of runway 34R.[4]
The 737 flight crew were also cleared to conduct an independent visual approach (IVA)[5] to runway 34R and programmed the flight management computer (FMC) with the GBAS[6] landing system (GLS) runway 34R instrument approach procedure (a GPS-based type of instrument approach). This provided guidance for a straight-in approach to a point on the runway threshold, published as waypoint RW34R, on the typical glide-path angle of 3°.
For a missed approach during this IVA, the crew were required to follow the instructions on the runway 34R approach chart (Figure 2). If a missed approach was initiated at or after the missed approach point, at about 0.5 NM from the runway (corresponding to the approach path intersecting with the decision altitude[7] of 220 ft), flight crews were to maintain the approach track (335°) until a mandatory right turn at 600 ft onto a heading of 070°.[8] The specified level-off altitude was 2,000 ft or as directed by ATC. If the missed approach was initiated before the missed approach point, flight crews were expected to maintain the approach track until reaching the missed approach point, then follow the procedure.
In accordance with standard operator procedures, the flight crew completed an arrival and approach briefing before descent. According to the crew, they reviewed all of the standard items, including the approach chart.
The captain recalled checking that the missed approach procedure loaded in the FMC was consistent with the approach chart. Both flight crew members later reported that they were familiar with the missed approach procedure for runway 34R and had discussed the risk of inadvertently climbing above the 2,000 ft level-off altitude, which was lower than typical at other locations.
They also discussed the requirement to turn right in a missed approach. The flight crew did not discuss how a missed approach would be flown with regard to the autopilot flight director system (AFDS)[9] modes, or whether the autopilot would be engaged, or how they would manage configuration changes during the required low-level manoeuvring.
The FO mentally noted that the GLS approach had speed restrictions but the flight crew did not discuss the required speeds. As the STAR did not join the GLS runway 34R approach, the flight crew observed a discontinuity between the two procedures in the FMC route legs page (in a GLS approach, the aircraft follows a predetermined approach path and angle). This meant that there was no active waypoint for AFDS guidance. There was no standard procedure for the crew to resolve the discontinuity.
During descent, the captain contacted Sydney air traffic control (the approach controller) and reported being visual with runway 34R in sight. The approach controller was responsible for the arrival sequence prior to transfer of aircraft to the aerodrome controller. The controller advised the ATSB that it was a normal day and they did not recall any details of the approach sequence of the Dash 8 and 737.
Figure 2: Sydney GLS runway 34R approach chart with missed approach requirements defined by blue boxes and approach speed requirements highlighted in yellow
Source: Qantas Airways, annotated by ATSB
The approach controller issued the flight crew a series of radar vectors to intercept the final approach for runway 34R. The FO selected the aircraft’s AFDS lateral mode to heading select (HDG SEL) to maintain the assigned headings.
After engaging heading select mode the flight crew did not update the route legs page in the FMC. As a result, the active FMC waypoint (the one to which the FMC would guide the flight crew or autopilot in LNAV) remained behind the aircraft’s position when it later passed through the waypoint (see 737 automatic flight system).
3The approach controller later cleared the flight crew for an independent visual approach (IVA).
Passing 4,300 ft, at 1827:19, the 737 flight crew selected flaps 1. At 10 NM track distance from the runway 34R threshold the aircraft was decelerating through 200 kt (the IVA required speed was 160–185 kt).
Descending through 2,300 ft, the aircraft was fully established on the approach with the autopilot and autothrottle engaged.
At 1830:05, as the 737 was passing about 1,850 ft and about 6.2 NM from the threshold, the approach controller instructed the flight crew to contact Sydney tower (a role carried out by the trainee ADC).
At this time, recorded data showed that the Dash 8 was 4.5 NM (8.4 km) ahead of the 737. Successive arrivals were to be at least 5 NM (9.3 km) apart unless there was prior coordination between the two controllers (see Surveillance separation).
The flight crew of Airbus A330, registered VH-EBJ, was operating scheduled passenger transport flight QF459 for Qantas Airways from Sydney to Melbourne, Victoria. The captain was the PM and the FO was the PF.
The A330 crew was cleared to depart via the MARUB SIX RNAV departure (Figure 3). This was a commonly-used standard instrument departure (SID) for jet aircraft taking off from runway 34R and tracking south. On reaching 500 ft, flight crews were required to make a right turn onto a south-easterly heading to intercept an easterly track (075°) from the airport to waypoint MARUB.[10] From there, aircraft were turned right onto a southerly track and a further right turn after passing 10,000 ft.
At 1824:58, the trainee ADC cleared the A330 to taxi to the holding point at the southern end runway 34R.
Figure 3: Sydney SID MARUB SIX RNAV departure plate
The trainee ADC cleared the Dash 8 to land at 1830:08. At 1830:21, when the 737 was 5.3 NM (9.5 km) from the runway 34R threshold, the flight crew selected flaps 15 and landing gear down. At 1830:24 the 737 flight crew established contact with the ADC. The aircraft was descending through 1,200 ft on a stable approach in landing configuration with flaps 30 and both the glideslope and localiser hold modes engaged. The 737 was gaining on the Dash 8 which was about 4.1 NM (7.5 km) ahead.
At 1830:31, the aircraft passed waypoint OLSOG, 4.8 NM (8.6 km) on the extended runway centreline, decelerating through 180 kt (with no wind). The approach chart (Figure 2) required flight crews to be 150–160 kt at this point, and if unable to comply, crews were to advise ATC. The 737 flight crew did not do so.
The Dash 8 was ahead of the 737 continuing its approach to runway 34R. The trainee ADC and OJTI both recalled that the Dash 8 appeared slower than a typical Dash 8 during approach and landing and then when vacating the runway. Radar data showed the ground speed of Dash 8 averaged 100 kt in the minute leading up to it crossing the runway 34R threshold. Airservices reported that the typical speed for a Dash 8 is 120–140 kt over the threshold.
At 1831:04, as the Dash 8 crossed the runway 34R threshold, the trainee ADC instructed the A330 flight crew to line up and wait on runway 34R (Figure 4Figure 4).
Figure 4: Position of the 737 when the A330 was instructed to line up
Source: Google Earth, annotated by the ATSB
At this time, the 737 was 3.3 NM from the runway 34R threshold, fully configured for landing (gear down and flaps 30), and was decelerating through 153 kt (Figure 5).
Figure 5: Representation of an ATC display when the A330 crew was instructed to line up showing location of the A330, Dash 8 and 737 aircraft and an exemplar separation measurement (light yellow).[11]
Source: Airservices Australia, annotated by the ATSB
The OJTI recalled that when the trainee ADC instructed the A330 to line-up in preparation for a departure, they glanced at the traffic display and noted that the 737 on approach was about 3.5 NM from the runway. At the time, the OJTI considered the gap to be ‘ambitious’ but if the preceding Dash 8 turned off early and the right phrases were used for an immediate take-off it should be expected to work.
At 1831:10, the trainee ADC instructed the 737 flight crew to reduce to minimum speed. The captain responded that they were at minimum speed. Flight data recorded that at that time the 737 was about 3.1 NM from the runway threshold with an airspeed of 155 kt and reducing, which was slightly above the selected approach speed and the minimum approach speed.[12]
The Dash 8 had landed but was still on the runway. At 1831:20 the trainee ADC instructed the A330 flight crew to expedite the line-up and be ready for an immediate departure. The captain responded that they were ready (for take-off).
At this time, the 737 was about 2.7 NM from the runway threshold with an airspeed of about 152 kt. The 737 captain recalled mentioning to the FO ‘this is not going to work’ and mentally preparing for a potential missed approach. The FO disconnected the autopilot and autothrottle at 1832:24 in preparation for a manually flown go-around should it be required.
At 1831:45, with the Dash 8 vacating the runway via the first available exit (T2), the trainee ADC advised the A330 flight crew, ‘on 34R cleared for immediate take-off’ (Figure 6). The 737 was now 1.8 NM from the runway threshold with a ground speed of 140 kt. The A330 FO pushed the power levers forward for take-off once the aircraft was lined up at 1831:54.
Figure 6: Sequence from A330 clearance for take-off
Source: Google Earth, annotated by the ATSB
The OJTI recalled they did not expect the trainee ADC to issue the take-off clearance but this was not discussed with the trainee. They asked the trainee if the runway separation standard would be met, to which the trainee replied ‘no’.[13] The OJTI also recalled asking the trainee ‘if you send [the 737] around, what are we going to do?’
At 1831:58, the trainee ADC instructed the 737 flight crew to ‘go around’ (conduct a missed approach). Initially, that instruction was mistakenly issued to the A330 (‘Qantas 459’) before immediately being corrected to the 737 (‘Qantas 545’). At 1832:02, the 737 captain read back the instruction. The 737 was descending through about 400 ft and was 1.2 NM (2.2 km) from the runway 34R threshold.
At this time the A330 was accelerating past 60 kt. The A330 captain recalled hearing the trainee ADC issue the 737 a go-around instruction and expected the take-off clearance to be cancelled. The A330 captain also recalled being aware of the potential conflict between their planned departure track via the SID and the 737 concurrently on the 34R missed approach. However, no further instruction was given by the controller, and the A330 flight crew continued the take-off in accordance with their clearance.
The trainee ADC later advised the ATSB that cancelling the A330 take-off clearance was an option but there would be risk involved. The OJTI considered that as the A330 was accelerating and it was difficult to visually assess speed at night, it would not be appropriate to cancel the take‑off clearance.
There was a tower shift manager (TSM) on duty in the tower, who performed direct supervision of the operating environment, and was required to support, intervene, or broadly direct activities. During this time the TSM was assisting a surface movement controller[14] and was not actively supervising or aware of the developing traffic scenario on runway 34R. The OJTI wanted to report the missed approach to the TSM, as procedures required, but gaining the TSM’s attention would require leaving the trainee ADC unsupervised.
At 1832:03, at about 350 ft and about 1.0 NM (1.8 km) from the runway threshold, the 737 flight crew commenced a manually-flown go-around and missed approach procedure. The FO pressed the take-off/go-around (TOGA) button[15] and called for the captain to select flaps 15, which the captain actioned at 1832:08. Once a positive climb was established the FO called for the landing gear to be selected up, and this was actioned by the captain.
At 1832:15, the 737 overflew the missed approach point while climbing through 400 ft, tracking on the runway heading. The aircraft passed through the mandatory missed approach turn altitude (600 ft) at 1832:21. The FO later stated that they believed the missed approach point was still ahead of the aircraft’s position and therefore delayed commencement of the right turn. The FO also recalled expecting the navigation mode to change from TOGA to lateral navigation (LNAV) and command the right turn, but that did not happen. The flight director lateral guidance instead maintained the runway track.
Passing about 600 ft the FO called for flap 5. The captain later reported hesitating before retracting the flaps because of an outdated procedure where flap retraction could only be commenced above 1,000 ft. The captain set flap 5 at 1832:23, and the FO commenced acceleration while still maintaining runway track.
At 1832:28 and accelerating through 160 kt, the 737 passed the pre-programmed missed approach point in the FMC (incorrectly located at the runway 34R threshold; see Runway 34R missed approach procedure) and was climbing through 860 ft to the right of the runway. The A330 had just commenced rotation.
The OJTI recalled they were aware that two aircraft departing on the MARUB SID and missed approach track concurrently would potentially conflict due to the inherent design of the two procedures. As a way of prompting a response, the OJTI asked the trainee ADC where the A330 was going to be tracking. The trainee ADC described the tracking of aircraft on the MARUB SID, which indicated to the OJTI that the trainee had understood they were going to have to apply tactical separation by adjusting the missed approach tracking of the 737 to increase the spacing with the departing A330.
The TSM was still assisting the other controller and remained unaware of the missed approach and developing conflict.
At 1832:31, passing about 920 ft, the 737 flight crew retracted flaps to flaps 1 while continuing to maintain runway track. The A330 was about 0.7 NM (1.2 km) ahead and beginning to climb.
Immediately after this, the trainee ADC instructed the 737 flight crew to turn right to heading 100°, thinking at the time that this would provide divergence from the A330 that was going to intercept the 075° radial. The trainee’s expectation was that the 737 would turn well before the crossing runway and be manoeuvring south of the 075 radial. The trainee ADC did not issue a traffic alert or a safety alert.[16]
The OJTI later reported that while the trainee’s choice of action would not have been the OJTI’s ‘first choice’ they expected the trainee to manage it. The OJTI was mindful that, at this point in the training, the trainee ADC was meant to be demonstrating the ability to work without instructor intervention. The OJTI later reported that they would have preferred the trainee ADC to cancel the A330’s SID and issue its flight crew a heading to the right of the runway centreline (such as 030°), but the OJTI did not communicate this to the trainee.[17]
The 737 was then at about 980 ft, which was below the minimum vectoring altitude (MVA) of 1,500 ft in this area (see Compromised separation). The turn instruction did not include phrasing to indicate the safety or urgency of the situation (such as traffic ahead) and responsibility for terrain clearance could not be assigned to the flight crew. A visual separation standard was still being applied between the two aircraft (see Air traffic control recorded data).
At 1832:37, about 1.1 NM (2.1 km) past the missed approach point and climbing through about 1,100 ft, the 737’s autopilot was engaged, the lateral mode was changed to heading select, and it commenced turning off the runway track (335°). The 737’s bank angle reached 25° (a standard rate turn) at 1832:51 and a steady turn at an average 210 kt was maintained until 1833:42; this gave an average turn radius of about 1.4 NM (2.6 km).
Due to the high nose attitude and increased workload during the climbing turn the flight crew did not see the A330, which was 0.6 NM (1.2 km) ahead of them and just passing the departure end of the runway at an altitude of about 350 ft.
The trainee ADC recalled that, at this point, there was quite a bit of distance between the two aircraft and the 737 looked like it was starting to turn south of the 075 radial. According to the trainee, for most of the time they were looking out the windows and able to see the aircraft clearly and judge speed, distance, and angle of bank. In addition the trainee ADC was looking at the radar display for speed and height.
The OJTI later reported they were monitoring the aircraft visually and were confident that the aircraft would not collide.
The A330 flight crew recalled that they were aware of the other aircraft being behind them conducting the missed approach procedure. The A330 FO looked for the 737 at about 1832:41, expecting it to have made an earlier right turn in accordance with the published missed approach procedure, but was unable to see it.
At 1832:44, passing about 650 ft, the A330 FO, who was PF, commenced a right turn to track in accordance with the MARUB SID. The FO later stated that after passing the turn altitude (500 ft) they delayed making the turn by a few seconds in the knowledge that the 737 was behind them.
The A330’s rate of climb at the initiation of the turn was about 2,800 ft/min. The A330 reached its average bank angle through the initial part of the turn (23°) at 1832:52 with an average airspeed of 141 kt and turn radius of about 0.7 NM (1.3 km). That is, as both aircraft turned, the A330 was turning tighter and travelling slower than the 737.
At 1832:50 the A330’s traffic collision avoidance system (TCAS) began to generate a traffic advisory[18] (TA) visual and aural annunciation. At this point the aircraft were 0.5 NM (0.9 km) and 600 ft apart. In response, the A330 FO verbalised the TA and confirmed that they had control in accordance with Qantas procedures. Figure 7 shows the position and flight paths of the aircraft through this period, and Figure 8 shows how an ATC display might appear if a controller measured the separation at this point.
Figure 7: Concurrent right turns and close proximity
Source: Google Earth, annotated by the ATSB
Figure 8: ATC display showing both aircraft at the time of A330 TCAS TA
Image represents a typical ATC display but is not necessarily representative of the display shown to any controller at the time of the occurrence. The separation measurement was manually added during a later replay of the occurrence and is approximate.
Source: Airservices Australia, annotated by the ATSB
The FO looked for the 737 again but was still unable to see it. A few seconds later the A330 FO saw the 737 in close proximity out the rear flight deck window towards the right rear quarter. In response, the FO reduced the aircraft’s angle of bank to widen the turn further away from the 737. Recorded data showed the rate of turn decreasing at 1833:06.
The FO advised the captain that ‘the 737 is very close’. In response, the captain reportedly instructed the FO to continue climbing at maximum rate, do not accelerate, and keep climbing until they were through 4,000 ft. The 737 captain recalled observing a TCAS TA alert but could not remember hearing an aural alert.
Throughout this period the trainee ADC was coordinating with the approach controller about the 737’s missed approach and anticipated track and altitude. The OJTI reported being confident that the 737 would pull ahead of the A330 in the turn. At 1833:03:
Separation between the aircraft had reduced to a minimum of about 0.42 NM (0.78 km) horizontally and about 508 ft vertically. At this time, the two aircraft were approximately abeam of each other and turning right. The A330 was climbing at about 1,900 ft/min and the 737 was levelling off at the altitude required by the approach chart (2,000 ft).[19]
Intending to increase the separation distance, the trainee ADC instructed the 737 flight crew to turn further right to 120°. Its heading was about 022° at the time.
The trainee ADC later reported that the A330 made an earlier and tighter turn than other widebody jet aircraft typically make (although still complying with the SID). This had unexpectedly brought the A330 closer towards the 737’s anticipated track.
At 1833:09, the trainee ADC issued a further instruction to the 737 crew to climb to 3,000 ft.
At 1833:17, the A330 captain made a radio transmission to the ADC, stating ‘that was very close – you could have asked us to do a heading’. At around this time, the A330’s TCAS TA ceased.
Intending to stop the A330’s turn, the trainee ADC issued an instruction to the A330 flight crew to turn ‘left’ to 100°. Initially, the trainee ADC did not cancel the SID clearance as was required before issuing vectors. After the A330 captain advised that the A330 was following a SID, the trainee ADC instructed the A330 flight crew to cancel the SID and turn ‘left’ to 100°.
The A330’s heading was about 070° at the time, almost directly behind the 737, with both aircraft turning right. The A330 was accelerating slowly through 158 kt while the 737 was maintaining about 205 kt before accelerating further; as a result, the distance widened.
Figure 9: Indicative ATC display at 1833:03 (the time of the closest horizontal distance)
Image represents a typical ATC display but is not necessarily representative of the display shown to a controller at the time of the occurrence. The separation measurement was manually added during a later replay of the occurrence and is approximate.
Source: Airservices Australia, annotated by the ATSB
The two flight paths then crossed with the 737 about 0.8 NM (1.5 km) ahead of the A330 (Figure 10). The trainee ADC asked the 737 flight crew to contact the approach controller at 1834:03 without first coordinating with the approach controller. At this time the two aircraft were about 1.2 NM (2.2 km) and 400 ft apart. This was less than the surveillance separation standard required for the transfer without coordination.[20]
The 737 climbed to 3,000 ft and was issued radar vectors for a second approach to runway 34R, landing at 1841. The A330 climbed to 5,000 ft and continued the planned flight to Melbourne.
Airservices Australia is Australia's principal civil air navigation service provider (that is, the provider of air traffic services for civil airports and airspace). The functions of Airservices are outlined in the Air Services Act 1995 and include the provision of air navigation services, aeronautical information, and aviation rescue and fire fighting services. The Manual of air traffic services (MATS)[21] stated the objectives of air traffic services were to:
prevent collisions between aircraft;
prevent collisions between aircraft on the manoeuvring area and obstructions on that area;
expedite and maintain an orderly flow of air traffic;
provide advice and information useful for the safe and efficient conduct of flights; and
notify appropriate organisations regarding aircraft in need of search and rescue aid, and assist such organisations as required.
This section details the context around the air traffic services aspects of the occurrence, including objectives and functions of Airservices and the manner in which they were applied, the involved personnel, separation standards, and flight path design. Unless otherwise specified, document references are from the version current at the time of the occurrence.
The trainee aerodrome controller (ADC), along with the on-the-job training instructor (OJTI), were controlling aircraft landing and departing on runway 34R at Sydney Airport from the Sydney air traffic control (ATC) Tower. At the time of the occurrence, the trainee ADC was completing their last shift before a performance assessment (check) for initial grant of the ADC rating that was scheduled for the next day.
The controller had joined Airservices and started initial tower training in 2012. On completion of training, the controller was stationed for about 4 years in the tower of a regional airport.
In November 2017, the controller commenced training for the surface movement control role at Sydney tower. The controller operated in this role until training was commenced for the Sydney tower ADC role in April 2019.
Training records indicate that the controller was judging spacing (for departures between arriving aircraft) well and had been advised to always have an ‘out’ (contingency plan). As the training progressed, the controller was instructed to make those decisions with less reliance on confirmation from the various OJTIs.
In regard to missed approaches, training records show that the controller was advised that ensuring separation from the preceding departure was more important than advising the departure controller about it. Also discussed was instructing aircraft to turn during missed approaches below minimum vectoring altitude (MVA) at night and compromised separation phraseology.
Two routine performance assessments were carried out by different check controllers in May and June 2019 to ascertain training progress. In general, the controller was found to be at the expected competency level for the respective stages of training.
Both check controllers noted that traffic volume during each assessment was relatively light and further experience in more challenging traffic and weather conditions (including at night) would be beneficial. There was no recorded concern about traffic sequencing or application of separation standards, although it was noted on the first assessment that the controller was a bit more conservative with traffic spacing than necessary.
On 23 July 2019, the controller began a 3-day performance assessment (check) conducted by a check controller as a prerequisite for granting of an aerodrome controller rating for the west, east, and coordinator functions in Sydney tower. The assessment report recorded that during the first 2 days the controller was able to process the traffic in a safe and expeditious manner. This was in the context of favourable weather conditions but relatively fast approaches (due to winds above 600 ft) and receiving aircraft that had reduced spacing at the time of transfer (less than the required 5 NM spacing).
The check controller also noted in the report that there is a ‘fine line’ between maximising the departure rate while ensuring separation, and that there is a need to always have a ‘way out’ – especially at night or in instrument meteorological conditions. This was prompted by an example of ‘bare’ (minimum) runway separation standard between departing and landing aircraft on runway 34R, with advice that if the crew of the approaching aircraft conducted a missed approach from short final approach, it would have been difficult to ensure separation if the departing aircraft was tracking via the MARUB standard instrument departure (SID).
During the check, the controller was questioned about a range of local procedures that could be implemented in different scenarios at Sydney. The check controller assessed that the controller’s knowledge was inadequate for issue of the rating and the check did not progress to Day 3. As part of a new training plan, the controller completed some additional classroom theory and was scheduled for 5 training shifts before another check, that was scheduled for the day after the occurrence.
The controller advised there had been some interruptions to the ADC training due to personal circumstances leave and there had been constraints on study outside of work hours. Although the controller described the training program as disjointed, it was completed within the average time frame for this rating of 12 weeks and none of the OJTIs had commented that there was any change to the controller’s skills on return from leave.
A review of the trainee ADC’s training records identified that one OJTI was involved in the initial practical training then was intermittently involved in subsequent training along with 8 other OJTIs. The controller advised the ATSB that, in their opinion, a variety of trainers could be positive as they can offer multiple perspectives and can address different areas, but there was a lack of continuity that probably hindered some aspects of the training.
Following the unsuccessful check, another OJTI was rostered for the additional training shifts. This was the same OJTI who was supervising the trainee ADC during the occurrence. The trainee considered this to be a positive phase of the training.
On 11 and 12 June 2019, the controller had completed practical emergency refresher training with a check controller in the Airservices tower simulator. This included a compromised separation exercise involving runways 16L/R by day. The check controller recorded that it was a good result and valuable part of the ADC training.
On the day of the incident, the controller recalled wanting the training process to be complete. Although recalling not feeling the pressure to perform or the upcoming check itself, after conversations with other people the trainee felt the check ‘was weighing in the back of [their] mind’.
On-the-job training instructor
The OJTI who was supervising the trainee ADC at the time of the occurrence had about 7 years previous experience as a tower and approach controller in the United States. After moving to Sydney, the OJTI converted the US qualifications and held all of the ratings for Sydney tower except shift manager. The OJTI endorsement was obtained in February 2019 and the OJTI had been a training instructor for one other controller prior to the occurrence.
On 12 and 13 June 2019, the OJTI had completed practical emergency refresher training with a check controller in the tower simulator. This included a compromised separation exercise involving runway 16L/R by day.
The OJTI was aware that the trainee ADC had been unsuccessful in the first performance assessment (check) because of knowledge deficiency rather than practical controlling skill. The OJTI was assigned to provide additional training to prepare the trainee for a performance assessment (check) that was scheduled for the day following the occurrence. If any intervention was required on the day of the occurrence, the OJTI was aware that the check would be postponed.
Prior to the day of the occurrence, the OJTI had supervised the trainee ADC on 3 shifts, all within the preceding week. The records indicate that the trainee was performing well with no requirement for the OJTI to provide prompts during controlling. In those previous training shifts, there were no missed approaches and the OJTI was confident in the trainee’s gap selection. As part of the training, the OJTI and trainee ADC reviewed minimum vector altitudes and some ways to manage missed approaches at night.
The tower shift manager (TSM) was a supervisory position responsible for the tactical management of risk while maintaining efficient air traffic operations. The purpose of supervision in the air traffic management context is to provide tactical management of risks while maintaining efficient air traffic operations. To achieve this, the TSM was required to directly supervise and maintain situation awareness of the immediate operating environment. Where necessary, the TSM role included supporting, intervening, or directing activities.
A TSM did not have authority to direct a controller to issue an operational instruction (the operational controller may accept advice from the TSM, but is always responsible for traffic separation).
Other aspects of the TSM role included management of controller resources across positions, providing ad hoc assistance to controllers, and administrative tasks. Ad hoc assistance tasks included to support the workload of the surface movement controller and provide break relief for other controllers as required.
The TSM had been in air traffic control since 1981, primarily in various roles at Sydney, and had been operating in the tower since 2004. Most of the shifts were conducted in the TSM role.
At the time of the occurrence, the TSM was temporarily engaged in the coordinator role for a surface movement controller. In that role, the TSM used a computer to locate and pre-activate the flight plans of taxiing aircraft. During busy periods, this allowed the surface movement controller to focus on monitoring ground traffic visually. The coordinator roles were not usually specially staffed, and as a result, this task was routinely done by the TSM during the afternoon/evening peak period.
A review of both the OJTI and trainee’s roster and sleep information found there was a low likelihood the trainee and OJTI were experiencing a level of fatigue known to have an adverse effect on performance.
Air traffic control (ATC) audio recordings and radar data records were obtained from Airservices. The audio recordings provided radio communications between controllers and flight crews. Radar data records provided aircraft position, speed and altitude information.
Separation is the concept of using approved separation standards, associated conditions and procedures to ensure spacing between aircraft is never less than a prescribed separation minimum. The Manual of air traffic services (MATS) defined separation as:
…the concept of ensuring aircraft maintain a prescribed minimum from another aircraft or object, whilst meeting the associated condition(s), and requirements of the standard, as specified in MATS.
In this context, the minimum separation can be measured in horizontal and/or vertical distance, or by time. Separation standards are a means to ensure separation between aircraft, the ground and protected airspace using longitudinal, lateral, vertical, and visual criteria and minima. The separation standards applicable to this occurrence are detailed in the following sections.
A 'loss of separation' was defined by Airservices as:
An infringement of prescribed minimum separation: - between aircraft - between aircraft and objects, or - between aircraft and Prohibited or Restricted Areas, or airspace reservations.
A related concept was ‘inadequate separation assurance’ (ISA) which Airservices defined as:
A traffic scenario where separation exists but: - the conflict is not identified, and/or - separation is not planned or is inappropriately planned, and/or - the separation plan is not executed or is inappropriately executed, and/or - separation is not monitored or is inappropriately monitored.
An ATS surveillance system can include information from radar, ADS-B,[22] or any other system that enables ATC to identify and locate aircraft.
The horizontal separation minimum based on ATS surveillance information is 5 NM (9.3 km), which may be reduced to not less than 3 NM (5.6 km) if the aircraft are under the control of a terminal control unit or associated control tower.
The Airservices Sydney operational procedures[23] detailed minimum aircraft separation distances for arrivals and departures at Sydney Airport. When runways 34L and 34R were in use for arrivals and departures, the terminal control unit (TCU)[24] was required to ensure the distance between successive arrivals was no less than 5 NM when transferred to the tower. This distance could be reduced after prior coordination between the TCU and tower.
In its safety investigation into the occurrence, Airservices found that:
The Sydney Tower and TCU [were] not consistently managing the arrival sequence spacing in accordance with the requirements of Sydney Operational Procedures. While tower controllers are able process departures with less than the required arrival spacing, this reduces the time available to process departures and achieve a runway standard. This increases the potential use of aircraft go-arounds as a risk mitigation strategy.
The Airservices report also stated:
While Sydney Operations are continuing to address the issues [regarding arrival sequence spacing], tower controllers have become habituated to the inconsistencies.
Within the tower’s airspace, successive arrivals and departures needed to be kept 3 NM apart. There was no separate restriction on spacing between aircraft departing from and arriving to the same runway, except for the runway separation standard (see Runway separation). When visual separation could not be applied between an aircraft departing from one runway and an aircraft executing a missed approach from the other runway, controllers were to ensure that the missed approach course diverged by at least 30° from the departure course unless another separation standard applied.
Runway separation standards are to ensure that a runway area is not occupied by another aircraft or obstruction when air traffic services (ATS) clear an aircraft for take-off or landing. The standards outline the requirements for separation of aircraft operating to and from runways and the required distances, expressed in units of time or distance, between departures and arrivals in a number of configurations, on the same, crossing or parallel runways.
When an aircraft was landing behind a preceding departing aircraft, controllers were instructed to:
Apply the ‘landing behind a preceding departing aircraft’ standard to fixed wing aircraft, provided that you do not permit the landing aircraft to cross the runway threshold until the preceding aircraft is airborne and:
a) has either commenced a turn; or
b) is beyond the point on the runway at which the landing aircraft could be expected to complete its landing roll and there is sufficient distance to enable the landing aircraft to manoeuvre safely in the event of a missed approach.
An aerodrome controller could only issue a landing clearance after:
a) the aircraft has commenced final approach of a straight-in instrument approach or has been sighted by the tower controller: i) on the late downwind leg of the circuit pattern; ii) on base leg; or iii) on final in the case of a straight-in visual approach;
b) a visual check of the landing path has been completed; and
c) no obstructions or collision risk exists.
When the runway was occupied by a preceding aircraft landing or taking off, controllers were instructed that they may:
… clear an aircraft to land only if there is reasonable assurance that the prescribed separation standard will exist when the aircraft crosses the threshold to land.
The ATSB estimated that the 737 would have required a landing clearance by about 1832:15, and at the time at which the 737 would have crossed the threshold (about 1832:26), the A330 would have just been passing the first runway exit and about to lift off.
Wake turbulence[25] standards must be applied for aircraft departing or conducting a missed approach behind another aircraft. Separation in a surveillance-equipped tower environment such as Sydney was generally based on time and/or distance criteria.
Wake turbulence separation was determined by grouping aircraft types according to maximum take-off weight and wake turbulence characteristics. The maximum take-off weight of the A330 placed the aircraft in the heavy category and the 737 in the medium category. Between these two types, with the heavier aircraft ahead, a distance separation minimum of 2 minutes or 5 NM was generally applicable.
A wake turbulence standard was not required between an aircraft landing behind an aircraft taking off on the same runway. If the landing aircraft, however, conducts a missed approach behind one departing, the aircraft in the missed approach is now considered a departing aircraft. Consequently, a controller should issue a wake turbulence caution to the flight crew of the following aircraft when less than the applicable wake turbulence standard exists.
Visual separation is a means of spacing aircraft through the use of visual observation by a tower controller. The use of visual separation allows a reduction in separation from that required when using a procedural or surveillance standard.
A tower controller was permitted to use visual separation if:
the aircraft were continuously visible to the controllers
the projected flight paths did not conflict
there were wide margins when judging relative distance or height, and
there was no possibility of aircraft being in close proximity.
To visually separate aircraft, controllers were instructed to primarily use azimuth (horizontal angle). Other considerations included:
The MATS noted that visually determining the relative distance of aircraft in close proximity can be in error or affected by optical illusions.
The ATSB investigation (AO-2015-084) discussed limitations of using visual separation at night, specifically a controller’s judgement of distance being limited by the physiology of the human eye.
In July 2013, the United States National Transportation Safety Board (NTSB) issued a safety recommendation to the Federal Aviation Administration (FAA). It raised safety concerns about use of visual separation to resolve aircraft conflicts at airports where ATC procedures permitted independent take-off and landing operations on separate, non-intersecting runways with intersecting arrival or departure paths. In these circumstances, with different geometry to the Sydney occurrence, ATC were unable to ensure safe separation in the event of a missed approach. The NTSB stated:
The separation standards … require that potential conflicts be resolved as part of the tower controller’s initial decision on when to issue takeoff clearances to two departing aircraft [on converging, non-intersecting runways]. However, the NTSB notes that there is no requirement for controllers to provide the same protections for the potential go-around flightpath of a landing aircraft even though, in the event of a go-around, the arriving aircraft effectively becomes a departure. Conflicts such as those described in this letter would have been clear violations of FAA safety and separation standards had the scenarios involved two aircraft departing the airport rather than one arrival and one departure. There appears to be no safety justification for treating the situations differently.
Because of the nature of the geometry of the encounters and the unexpected nature of the go-arounds, it was not possible for the ATC tower controllers to issue effective control instructions to ensure that the aircraft avoided each other. Therefore, visual separation procedures could not be successfully applied or asserted as an adequate means of resolving the conflicts. The NTSB is concerned that in these events, ATC was not able to ensure the safe separation of aircraft. Instead, separation was established by resorting to impromptu evasive maneuvers by pilots during critical phases of flight. The NTSB concludes that the lack of specific separation standards, similar to those defined in paragraph 3-9-8 of FAA Order 7110.65, “Air Traffic Control,” applicable to departing aircraft and aircraft conducting a go-around from non-intersecting runways where flight paths intersect, facilitates hazardous conflicts and introduces unnecessary collision risk.
Therefore, the National Transportation Safety Board makes the following recommendation to the Federal Aviation Administration:
Amend Federal Aviation Administration Order 7110.65, “Air Traffic Control,” to establish separation standards similar to the provisions of paragraph 3-9-8 between an arriving aircraft that goes around and any combination of arriving or departing aircraft operating on runways where flight paths may intersect. (Safety recommendation A-13-024).
In response to the safety recommendation, the FAA responded that:
…the FAA amended paragraph 10-3-14, Go-Around/Missed Approach, to require the implementation of procedures to ensure that an arrival that executes a go-around does not conflict with a departure off the non-intersecting converging runway, and for facility management to define tools that could assist in the locally developed procedures.
The NTSB closed the recommendation with the status ‘Closed-Acceptable action’.
Separation assurance can be either strategic or tactical. Strategic separation assurance includes the development of air traffic practices to reduce the likelihood of aircraft coming into conflict, particularly where traffic frequency congestion may impair control actions. Tactical separation assurance is an activity conducted by the controller that includes traffic planning and conflict avoidance. Where two routes converge, such as at a runway, strategic separation is not possible; nevertheless, routes are designed to optimise separation while being tactically managed by air traffic controllers.
To achieve the first objective specified in the MATS (avoiding collisions between aircraft), ATS have preventative defences in place to assure aircraft remain separated, and recovery defences when separation is comprised or lost. The MATS described the responsibilities for aircraft separation for ATS as follows:
Provide separation
Provide separation using approved separation standards, associated conditions and procedures ensuring spacing between aircraft is never less than a prescribed separation minimum.
Assure separation
Assure separation through the process of assessing traffic, identifying conflicts, planning to ensure separation, executing the plan and monitoring the situation to ensure the standard is not infringed.
Maintain separation
Where the type of separation or minimum used to separate two aircraft cannot be maintained, establish another type of separation or another minimum prior to the time when the current separation minimum would be infringed.
The separation standard may vary depending on a number of factors, including the type of airspace in which the aircraft are operating, and may specify horizontal or vertical distances, or separation based on a flying time between two aircraft passing the same location.
Controllers proactively plan to avoid conflict between aircraft, rather than to wait for or allow a conflict to develop before its resolution.
Sydney Airport is a major international airport which facilitates international, domestic, and regional aircraft movements. It has two parallel runways that are oriented 16/34, separated by about 1 km, and another runway oriented 07/25. The Sydney tower is located to the east of runway 16R/34L and south of runway 07/25.
The airport is located in a low-lying area adjoining Botany Bay. The elevation of terrain to the east of runway 34R within a 10 NM radius is generally no higher than 150 ft with some terrain to the north-east rising up to about 350 ft. The major obstacles rising to a maximum of 1,100 ft were buildings located in the city, about 5 NM (9 km) to the north-north-east of the airport.
Airservices provided 24-hour air traffic services at Sydney Airport. The Sydney Airport Demand Management Act 1997 (Cth) imposed, among other things, a maximum limit on the number of aircraft movements (landings and take-offs) at the airport in any 60-minute period of operation.
The on-duty controllers responsible for the management and sequencing of arrival and departure aircraft inside the Sydney terminal control area were located in the Terminal Control Unit (TCU). That unit operated from a building located at Sydney Airport, separate to the tower.
The on-duty controllers responsible for all aircraft and vehicle movements on taxiways, runways and in the immediate vicinity of the airport were located in the tower. They were responsible for 4 NM around the airport and separation was primarily on a visual basis supplemented by radar displays.
At the time of the occurrence, the air traffic control mode at Sydney was parallel runway operations with independent visual approaches (IVA) to runway 34L and 34R. Independent departures were in effect from runway 34L and 34R.
Arrivals to runway 34R were managed by the approach and director controllers in the TCU before being transferred to the ADC to a boundary approximately 4 NM from the runway 34R threshold and at or below 500 ft.
Independent visual approaches (IVA) allowed two aircraft to be on final approach to parallel runways at Sydney in visual meteorological conditions (VMC). Depending on the meteorological conditions, an IVA could be initiated from a circuit or from an instrument approach once a pilot was visual (could see the runway).
The Aeronautical information publication (AIP) Australia outlined important instructions and advisory information to pilots for the conduct of an IVA. Once ATC cleared a pilot for an IVA the requirements of the procedure must be followed.
Pilots were instructed to fly accurate headings when being vectored for final approach and that it was imperative to intercept the final approach path without overshooting the assigned runway centreline.
Another requirement was that pilots must operate at approach speeds of 160–185 kt when 10 NM from the runway threshold and 150–160 kt when 5 NM from the runway threshold. ATSB analysis of track distance indicated that the 737 was at about 200 kt at 10 NM and 180 kt at 5 NM.
At most major airports flight crew navigate their aircraft along flight paths which are known as standard instrument departures (SIDs) and standard terminal arrival routes (STARs). SID and STAR flight paths provide controllers and flight crew with:
separation standards built into the airspace design for departing and arriving aircraft
improved flight path predictability
reduced complexity and workload for pilots and controllers.
At Sydney, in most cases flight path design used open STARs, which did not join directly with instrument approach procedures. Open STARs required the director controller to provide radar headings to link the STAR with final approach.
According to Airservices, the MARUB SIX SID had been published and in operation since about 1997.
The Airservices National ATS procedures manual (NAPM) provided guidance to all controllers on their duty of care requirements. It outlined that all controllers who are aware of information of an unsafe situation or potential unsafe situation are expected to take all necessary action to remove that risk. It was also expected that the extent of the action required will be driven by professional judgement given the circumstances and would include an assessment of the likelihood of the event occurring and the potential severity of the outcome.
The Airservices National ATS administration manual (NAAM) provided guidance on supervision and operational command authority (OCA). It stated the purpose of supervision in operational environments:
…is to provide tactical management of risks while maintaining efficient air traffic operations. Supervision involves observation of air traffic service delivery and, where necessary, supporting, intervening or directing activities within the area of responsibility. The supervisor is responsible for managing airspace and traffic to ensure safety and maximise network efficiency.
The Sydney tower shift manager (TSM) position held OCA and was therefore required to perform direct supervision of the operating environment within Sydney Tower’s area of responsibility. Direct supervision required the TSM to be physically present within the immediate operating environment and maintain situational awareness of that environment. The NAAM stated:
Where supervision is provided in the delivery of ATS services the supervisor must:
a) monitor the environment and maintain situational awareness of the factors affecting the safety risks and hazards within the environment being supervised;
b) identify threats within the operational environment and ensure adequate, effective risk controls are in place to ensure safe service delivery;
c) prioritise tasks based on the level of risks being managed;
…g) issue Withdrawal of ATS Privilege (ATS-FORM-0009) to relevant employees for which they are responsible when circumstances are considered to be (or to possibly be) compromising to the safety and/or efficiency of the overall operational service.
The NAAM included a limitation in the exercising of OCA, in stating that:
OCA does not give the holder the authority to instruct an operational controller to take certain actions such as directing a controller to issue an operational control instruction. The operational controller is always responsible for traffic separation, but may accept advice from the OCA holder.
Airservices advised the ATSB that the supervisor (TSM) could not have assisted with the provision of safety alerts or wake turbulence caution.
Air traffic control training comprised theoretical, simulator and on-the-job components. On-the-job instruction is conducted in the workplace by specially trained instructors (OJTI).
While conducting training, an OJTI would hold overall responsibility for the provision of a safe and efficient air traffic service, as a trainee would either be not licenced or not endorsed.
During the training period, a trainee would be given increasing levels of responsibility for the control and separation of aircraft, but the OJTI must monitor the trainee’s performance and ensure that any errors or omissions that may impact safety can be corrected in a timely manner. Intervention strategies for an OJTI range from questioning the trainee, to suggesting an alternate course of action, to directing the trainee, and finally to intervening by taking over or overriding the trainee.
Airservices defined a progressive ‘prompting hierarchy’ to be applied by OJTIs to allow a trainee to develop the required skills throughout the development of a safety situation while ensuring it will be effectively managed:
1. Asking – situation awareness/monitoring When prompting at this level, [an] OJTI is trying to determine if the trainee has detected that there is something in their environment that needs their attention.
2. Suggesting – decision making (prioritising) When prompting at this level, [an] OJTI is assisting the trainee to prioritise their attention appropriately to the emerging situation.
3. Directing – decision making (planning) When prompting at this level, [an] OJTI is providing the trainee with the specific solution or plan to the safety critical situation. The trainee is implementing the directed instruction from the OJTI and at this stage, the plan is the OJTI’s.
4. Taking over (execution) At this level of prompting, [an] OJTI has taken over the execution of the plan as there is no longer an opportunity for the trainee to act to safely resolve the situation.
Direct intervention was considered a ‘last resort’ and only used to ensure safety. To facilitate this, the communication system enabled the OJTI to override the trainee’s transmissions.
On the night of the occurrence, the OJTI was cognisant of compromising the assessment and considered that any level of intervention would result in a failed assessment for the trainee ADC.
Separation of aircraft is considered to be compromised when separation standards have been infringed, or where separation assurance is absent to the extent that a breakdown of separation is imminent.
In accordance with the MATS, controllers were required to:
… give first priority to separating aircraft, issuing safety alerts and providing directed traffic information as provided by this manual. Perform first that action which is most critical from a safety standpoint.
The MATS required that, except in certain circumstances, controllers issue a safety alert prefixed by the phrase 'SAFETY ALERT' when they become aware that an aircraft is in a situation that places it in unsafe proximity to another aircraft.
The MATS required a controller to issue traffic avoidance advice, prefixed by the phrase 'AVOIDING ACTION', to an aircraft that is receiving an ATS surveillance service and in the controller’s judgement is in a situation that places it at risk of a collision with another aircraft under surveillance.
The phraseology to be used by ATC when providing safety alerts and avoiding action was contained in the AIP. An example of a generic traffic alert is:
(Callsign) AVOIDING ACTION, TURN LEFT/RIGHT IMMEDIATELY (specific heading, if appropriate), and/or CLIMB/DESCEND (specific altitude if appropriate), TRAFFIC (provide position of traffic).
It was permissible for a controller to abbreviate safety alerts and traffic avoidance advice phraseologies to ensure timely provision of advice.
In daytime, vectoring aircraft at low altitudes was permitted because flight crews could visually maintain adequate height to avoid ground and obstacle collisions. To do this, controllers could assign terrain clearance responsibility to the flight crews.
The MATS stated that a controller could only provide an instrument flight rules (IFR) aircraft with a vector in visual meteorological conditions (VMC) by day.
At night when radar vectoring, the controller needed to retain the responsibility for ensuring terrain clearance is maintained as pilots may not be able to see terrain and obstacles. For this reason, controllers were generally not permitted to vector aircraft below a minimum vectoring altitude (MVA) at night.
The MVA was the lowest altitude a controller may assign to a pilot in accordance with a radar terrain clearance chart (RTCC). The MVA (minimum RTCC) was 1,500 ft in the area the 737 flight crew was initially vectored (Figure 11).
In response to recent occurrences at surveillance towers where tower controllers had vectored aircraft conducting a missed approach without complying with the MATS requirements, Airservices issued a standardisation directive to all surveillance towers (including Sydney), effective 18 June 2019. The Airservices safety investigation report stated:
The directive reiterated that tower controllers are not permitted to vector or provide an uncoordinated vector in IMC [instrument meteorological conditions] conditions or at night unless prior coordination through the relevant TCU and that tower controllers may only assign terrain clearance to the pilot when vectoring, in VMC [visual meteorological conditions] by day.
When controllers become aware that an aircraft is in unsafe proximity to terrain or an obstacle they are required to issue a safety alert to the pilot.
In addition to the occurrence controllers, the ATSB interviewed several other Sydney tower controllers from Sydney tower to understand their view of how they would deal with a similar situation as the occurrence. The general view was that in line with the requirement for controllers to provide a duty of care in an unsafe situation, their professional judgement was that the least-risk option to aircraft was to issue vectors below MVA at night and issue a safety alert terrain to the flight crew. These controllers were aware this was not in accordance with the MATS but commented that it had become a normalised solution to the hazard.
Figure 11: Extract of replayed ATC display showing 737 location when its crew was instructed to turn right (from 800 ft) and relevant radar terrain clearance chart (RTCC) levels
Source: Airservices Australia, annotated by the ATSB
Do not allow anything in these instructions to preclude you [the controller] from exercising your best judgement and initiative when:
a) the safety of an aircraft may be considered to be in doubt; or
b) a situation is not covered specifically by these instructions.
Similarly, the Airservices National ATS Procedures Manual stated:
Upon becoming aware of information such that it would be reasonable to conclude that an unsafe situation has, or may occur, it would be expected that all necessary action is taken to remove that risk.
Note: The extent of the action required will be driven by professional judgement given the particular circumstances and would include an assessment of the likelihood of the event occurring and the potential severity of the outcome.
Compromised separation recovery training was required for all ATC endorsement training courses. This comprised a training workshop and a simulator exercise. The learning outcomes for the compromised separation training workshop were:
identify the critical sector/unit hot spots for compromised separation and unsafe proximity
describe critical actions and responsibilities in the event of compromised separation or unsafe proximity, including phraseology and with reference to sector/unit specific scenarios
identify aircraft performance considerations critical to resolution of sector/unit specific situations.
Points to be covered included the requirements for safety alerts or traffic avoidance information, and the issuance of accurate timely and well delivered instructions to de-conflict. This training workshop was assessed by the on-line compromised separation training package.
Along with 4 other emergency training sessions, the compromised separation simulator exercise was conducted by a check controller at the Airservices tower simulator. This was a practical application of the topics from the training workshop, and was based on parallel runway 16L/R operations by day.
Following this initial training, tower controllers were required to complete the knowledge-based online training package annually and the skills-based simulator training at least every 3 years.
At the time of the occurrence, Airservices had no compromised separation recovery training scenarios for conflicts on the MARUB SID / runway 34R missed approach procedure, or for compromised separation scenarios where aircraft were below the MVA at night at Sydney.
Airservices designs flight paths in compliance with Civil Aviation Safety Authority (CASA) regulations and standards, and International Civil Aviation Organization (ICAO) standards and recommended practices (SARPs). CASA has mandated that flight path design in Australia must comply with the ICAO SARPs for instrument flight procedure design, except where varied by Australian legislation/manual of standards.
In accordance with Civil Aviation Safety Regulations (CASR) Part 173, CASA has certified Airservices as an organisation permitted to design approach and departure procedures for aircraft operating under instrument flight rules (IFR). The certification process requires a chief designer to manage flight path design and a team of qualified designers.
International Civil Aviation Organization publications
When designing flight paths consideration is given to multiple elements outlined in ICAO publications Procedures for air navigation services – Aircraft operations (PANS-OPS, ICAO Doc 8168) and Procedures for navigation services – Air traffic management (PANS-ATM, ICAO Doc 4444). These include terrain and obstacle clearance, wake turbulence, meteorological conditions, aircraft performance, climb gradients, descent profiles, speeds, rate of turn, angle of bank (turning movement) and the airspace available to safely contain the procedure. Operationally significant design criteria are specified on the charts for each procedure.
Australian legislation
The Air Services Act 1995 requires that Airservices:
In exercising its powers and performing its functions, must regard the safety of air navigation as the most important consideration.
Subject to subsection (1), [Airservices] must exercise its powers and perform its functions in a manner that ensures that, as far as is practicable, the environment is protected from:
(a) the effects of the operation and use of aircraft; and
(b) the effects associated with the operation and use of aircraft.
The latter subsection required, among other things, consideration of elements such as environmental impact (including noise) and community impact associated with flights around airports.
Long Term Operating Plan
Airservices also needed to follow Ministerial directions including, in the case of Sydney Airport, a direction to follow the Long Term Operating Plan (LTOP).[27]
The Ministerial direction meant that Airservices must ensure that, subject to safety and weather conditions:
as many flights as practical use flight paths over water or non-residential areas where aircraft noise has the least impact on people
the rest of the air traffic is spread or shared over surrounding communities as fairly as possible
runway modes (patterns of aircraft movement) change throughout the day so individual areas have some respite from aircraft noise on most days.
In practice, these requirements limited the options available for the design and operation of flight paths such as SIDs and missed approach paths, although the Ministerial direction emphasised that ‘the safety of aviation operations is not to be compromised.’
Among the ‘main matters raised relevant to the Ministerial direction’ were ‘concerns of individuals and community groups about flight paths over specific areas, including flight corridors to the north’ of Sydney Airport. The LTOP stated:
[Outbound runway 34R tracks] were designed to make use of the open golf course area, and the shortest route to the sea, to facilitate over water tracking, and to avoid the ‘obstacle clearance area’ posed by the city. Additionally, the design had to satisfy the requirement of the independent parallel runway separation standard, which dictates a turn of a minimum of 15 degrees to the east from runway heading.
When runway 16L/34R was built in the mid-1990s, take-offs to the north from runway 34R were initially not permitted. From 19 October 1996, Airservices introduced new procedures to further reduce the number of overflights of the areas that had been exposed to the greatest levels of aircraft noise. The LTOP stated:
The first procedure involves take offs to the north from the new parallel runway (runway 34R) and turning east as soon as safely practicable, following existing flightpaths out to sea.
Sydney flight paths generally direct aircraft departing from runway 34R to the east, while aircraft departing from the parallel runway 34L are directed to the north and west. This distributes the noise of departures from each runway across different areas.
Flight Safety Foundation guidance
The Flight Safety Foundation is an international non-profit organisation that provides impartial, independent, expert safety guidance and resources for the aviation and aerospace industry. It identifies global safety issues, sets priorities and serves as a catalyst to address these concerns through data collection and information sharing, education, advocacy and communications.
The Go-Around Decision Making and Execution Project: Final Report to Flight Safety Foundation (Blajev and Curtis, 2017) recommended that:
An ATS agency responsible for instrument approach procedure design should ensure that straightforward go-around procedures are available and published for each runway. These go-around procedures should be designed in consultation with pilots who are representative of those who will be expected to use them.
Implementation advice for the Flight Safety Foundation recommendation regarding a missed approach point design included:
- a low (eg. Below 2,000 ft) first stop altitude and an early turn in a missed approach procedure should be avoided.
- procedural de-confliction of the missed approach path from other traffic and from the risk of exposure to wake turbulence, especially on late go-arounds, should be provided
- environment restrictions – especially noise-abatement restrictions – must not affect the design of missed approach procedures if their imposition would compromise safety standards.
Prior to the publication of a flight path, Airservices ensures that flight path designs are compliant with the CASR through, among other requirements, designs carried out by qualified designers in accordance with ICAO Doc 8168. CASA then conducts flight validations to ensure procedures are safe and flyable and that they meet applicable design standards.
For instrument approach procedures, the missed approach design provides a minimum obstacle clearance to aircraft climbing along the specified missed approach path. This ensures aircraft are protected from obstacles and terrain when conducting a missed approach providing the aircraft remains on the missed approach procedure track.
Safety risk management includes hazard identification, safety risk assessments and safety risk mitigation. The ICAO Safety management manual stated:
The SRM [safety risk management] process systematically identifies hazards that exist within the context of the delivery of its products or services. Hazards may be the result of systems that are deficient in their design, technical function, human interface or interactions with other processes and systems. They may also result from a failure of existing processes or systems to adapt to changes in the service provider’s operating environment.
Organisational investigations of safety occurrences and hazards are an essential activity of the overall risk management process in air traffic services. Investigations identify latent system deficiencies and missing or inadequate defences for which corrective safety action can be taken to ensure continuous improvement to an organisation’s entire safety system.
The Airservices risk management and mitigation measures of local Sydney tower hazards were recorded in the Sydney tower operational risk assessment (ORA). ORAs were managed and reviewed in accordance with the requirements of the Airservices SMS. They were described by Airservices as ‘a higher level representation of the threats and barriers and one artefact reviewed as the outcome of safety risk management activities’.[28]
The Airservices ORA review procedure described the roles and responsibilities for the identification, assessment, and management of hazards/threats. Furthermore, it described when ORA reviews should be conducted, stating:
- Reviews driven by changes to practices, procedures and/or equipment (referred to as 'ad hoc' reviews) which are conducted at the time of any such change.
- Comprehensive reviews conducted at periods not exceeding 24 months from the previous comprehensive review.
Airservices ORAs were based on the ‘bow-tie’ model as a risk evaluation method to analyse and demonstrate causal relationships in high-risk scenarios such as a mid-air collision. Risk in bow-tie methodology is elaborated by the relationship between hazards/threats, top events, and consequences. Controls are used to display what measures an organisation has in place to control the risk. Controls can be proactive and reactive. A third control classification is escalation control which is used to manage escalation factors. Escalation factors are certain conditions that can make a control fail.
Identification of conflict scenarios
The ATSB examined all 10 Sydney tower ORAs for item ‘H-01-Conflict in the air’ from 2012 to 2019. At the time of the occurrence the most recent review was Sydney tower ORA (H-01-Conflict in the air) version 6.1, dated 3 July 2019. It identified a top event of ‘Inappropriate or lack of control action or advice’ with the hazard of ‘Conflict in the air’. The threats contained in the ORA relevant to this occurrence were:
controller incorrectly applies standards or procedures
independent parallel departures
missed approach (go-around)
unexpected pilot action
loss of separation with obstacle (terrain)
loss of separation (including runway separation).
The ORAs did not include specific scenarios involving loss of separation. More specifically, the ORAs did not include the potential MARUB SID / runway 34R missed approach conflict as a threat or escalation factor. Additionally, the Sydney tower ORA did not contain the hazard of compromised separation when aircraft were below the MVA at night.
Evaluation of risk controls
Each of the threats had identified defensive barriers to prevent the associated threat from realising the top event and subsequently the hazard. Most of these barriers were procedural in nature and included supervision, compromised separation rules and procedures, the issuing of safety alerts, and pilot action.
Airservices advised ATSB that threats associated with aircraft concurrently following the MARUB SIX SID and runway 34R missed approach procedures were ‘known’ and that the risk was ‘effectively managed.’ Airservices reasoned that ‘there had not been an occurrence history or operational assurance activities that had identified systemic risk control shortfalls’ with the management of MARUB SIX SID and runway 34R missed approach traffic scenarios to indicate that the level of risk was not as low as reasonably practicable.
The Civil Aviation Safety Authority (CASA) has the responsibility of oversighting and ensuring Airservices maintained and operated its ATS functions in accordance with the Manual of Standards for CASR Part 172 and approved procedures in the MATS. This oversight consisted of regulatory audits of Airservices functions such as air navigation service delivery and flight path design management, and the Airservices SMS.
CASA completed a surveillance audit on Sydney Tower in July–August 2018, one year before the occurrence. The report stated:
The surveillance team reported two (2) Safety Findings and three (3) Safety Observations.
The first Safety Finding related to the Operational Risk Assessment (ORA) not being updated to track ongoing A-SMGCS [advanced surface movement guidance and control system] faults.
The second Safety Finding related to the Business Continuity Plan (BCP) not being reviewed in accordance with the document.
The Safety Observations related to:
- occurrence rates on Runway 16R - standardisation of stop bar protocols - lighting intensity of an advertising sign.
Runway 16R is a runway to the west of and parallel to runway 34R and refers to operations in the opposite direction. Regarding the runway 16R occurrence rates, the CASA report stated:
Sydney Tower CIRRIS[29] data confirms aircraft landing behind a departing aircraft on Runway 16R are involved in an increased number of go arounds and Loss of Separation (LOS) events. The occurrence rate is noted as being higher for Runway 16R compared to other Runways at Sydney.
A secondary impact of increased go rounds is the loss of an additional landing slot, thereby negatively impacting airport efficiency and increased ATC workload and complexity.
Observations and reports from personnel interviews at Sydney defined this situation as an increased latent risk.
CASA recommends that Airservices review and investigate the underlying reasons behind the increased go round / LOS occurrences for arriving aircraft behind a departing aircraft on Runway 16R.
Airservices advised the ATSB that in the 2019 calendar year, there were 348,730 movements at Sydney and within the Airservices occurrence reporting system there were 349 reports where ‘go around’ was recorded as the primary occurrence type. However, due to limitations in recorded data and the type of occurrences that were required to be reported, it was not possible to obtain detailed data on related occurrences at Sydney involving aircraft concurrently following the MARUB SIX SID and runway 34R missed approach procedures and the level of controller intervention, if any, that resulted.
Of 9 Airservices controllers interviewed by the ATSB, 8 indicated that the MARUB SIX SID and the runway 34R missed approach procedure was a recognised concern. Some discussed the absence of compliant options to resolve a potential conflict as being problematic. One controller interviewed by the ATSB estimated that intervention due to the potential for conflict between the MARUB SIX SID and runway 34R missed approach procedures occurred 10 to 20 times in a year (day and night).
A search of ATSB occurrence records from 2013-2022 did not identify any other losses of separation associated with aircraft concurrently using the MARUB SIX SID and a missed approach from runway 34R.
On 5 reported occasions, including the one under this investigation, an aircraft on approach to runway 34R conducted a missed approach due to a potential conflict with another aircraft taking off from the same runway. All were initially reported to the ATSB as a missed approach; the occurrence under investigation was revised to include the loss of separation category after further enquiries from the ATSB based on the Qantas reports. No flight path data for the other occurrences were available at the time of review.
The ATSB research report Loss of separation between aircraft in Australian airspace – January 2008 to June 2012 (AR-2012-034) found that ‘assessing and planning’ or ‘monitoring and checking’ errors were involved in most individual controller actions that contributed to loss of separation (LOS) occurrences. Ineffective management of compromised separation before it became a LOS was categorised as an assessing and planning error. Monitoring and checking errors included controller actions associated with maintaining awareness of traffic disposition.
In addition, the ATSB research found that of the LOS occurrences in which ATC actions were contributory, about one quarter involved communication errors. These included not passing traffic information to pilots once separation was compromised. The research found that task demands were the most common type of local condition identified in LOS occurrences where controllers were involved – in particular, high workload and distractions. Common in all ATC environments, these local conditions were more common in the tower environment.
On 18 May 2015, there was a series of LOS occurrences and vectors issued to flight crew below the minimum vector altitude (MVA) in the airspace around Adelaide Airport, South Australia.[30] An Airservices safety investigation into the occurrences identified the following safety issues:
Compromised separation training for controllers at Adelaide Tower did not incorporate scenarios where aircraft were below the minimum vector altitude at night.
The updated Intervention Techniques and Prompting initial qualification training was not provided to existing OJTIs or workplace assessors. Additionally, the relevant refresher training module had not been updated.
There were no defined explicit requirements, including the required phraseology, for coordinating the transfer of separation responsibility between controllers.
Airservices subsequently advised that each of the safety issues had been addressed and all related safety actions had been completed. The ATSB reviewed the Airservices report, safety issues and safety actions. Based on this review, the ATSB considered it was very unlikely that further investigation would identify any systemic safety issues and discontinued the investigation.
In October 2011, at night at Melbourne Airport, Victoria and during land and hold short operations (LAHSO), an aircraft on final approach to land on runway 34 conducted a missed approach while another aircraft was landing on runway 27. LAHSO allowed for simultaneous landings on crossing runways, with the requirement that one aircraft stops well before the intersection of the runways. As the aircraft in the missed approach was below the MVA, the controller was unable to issue a radar vector to ensure separation. The occurrence was reported but the ATSB did not investigate.
On the evening of 5 July 2015, with LAHSO in effect at Melbourne Airport, a Boeing 777 was cleared for an immediate take-off from runway 34 while two Boeing 737s were on approach to runways 34 and 27. This resulted in the crew of the 737 on approach to runway 27 initiating a missed approach, followed by the crew of the 737 on approach to runway 34 being instructed by ATC to go around. The 737 on approach to runway 34 was then radar vectored by ATC below the MVA.
Civil Aviation Safety Authority response
On 2nd November 2015 CASA wrote to the ATSB and Airservices listing a number of key concerns involving Melbourne operations, which included:
the requirement for IFR aircraft to remain on the published missed approach procedure until reaching the lowest safe altitude
the procedural restrictions on ATC not to issue turn instructions applicable while the aircraft is below the MVA during a missed approach at night that takes the aircraft outside the protections of the published missed approach
the limitations on the ability of ATC to provide effective separation to aircraft at night based on visual observation
the limitations on pilots of IFR aircraft to see and manoeuvre to avoid one another at night
the lack of demonstrated training competency of air traffic controllers in the handling of night-time compromised separation.
In the same correspondence CASA also stated:
… the (air traffic management) system should not rely, as a primary means of defence, on vectoring or heading changes for (instrument flight rules) category aircraft at night that are below the appropriate minimum altitude.
ATSB investigation
The ATSB investigation[31] into the 2015 occurrence reported that:
…since 2011, Airservices Australia had been aware of the hazard associated with the inability to separate aircraft that were below the appropriate lowest safe altitude at night but had not adequately mitigated it. This resulted in a situation where, in the event of a simultaneous go-around at night during LAHSO at Melbourne Airport, there was no safe option available for air traffic controllers to establish a separation standard and to ensure a mid-air collision did not occur when aircraft were below minimum vector altitude. Though Airservices Australia had implemented a number of preventative controls prior to this occurrence in response to concerns expressed by the Civil Aviation Safety Authority (CASA), a recovery control was not implemented until 2016.
The ATSB identified a safety issue, stating that ‘the hazard associated with the inability to separate aircraft that are below the appropriate lowest safe altitude at night was identified but not adequately mitigated.’ The ATSB also found that:
… the compromised separation recovery training provided to the air traffic controllers employed in the Melbourne ATC Tower did not include a night scenario for missed approaches during LAHSO.
Safety actions
In response to the occurrence, Airservices introduced:
a stagger procedure for arrival pairs to prevent unsafe proximity in the event of a missed approach
training for Melbourne ATC Tower controllers in compromised separation recovery at night during LAHSO
a safe sector to allow controllers to vector aircraft to a path clear of obstacles when below the MVA following a missed approach at Melbourne during LAHSO.
The safe sector at Melbourne had been assessed for obstacle clearance and found suitable for vectoring the aircraft below the MVA at night. CASA issued Airservices with a partial exemption to the MATS to allow this. The exemption only applied during LAHSO at Melbourne at night, and had certain conditions including that controllers could only vector aircraft when they were above 600 ft and only towards an internally-published region (the safe sector). Melbourne tower controllers also had to be trained in the use of safe sectors. The exemption was renewed at intervals and was current at the time of the Sydney occurrence.
In November 2015 Airservices advised CASA that it intended to roll out a national program to further enhance the knowledge and skills of tower controllers. The action would involve enhancements to night-time compromised separation training for risk situations.
To implement this, an Airservices standards manager emailed line training managers to include scenarios where aircraft are below the MVA at night in their respective training packages. However, the Airservices system for assigning safety-related tasks and assuring their completion (CIRRIS) was not used. Consequently, some Airservices line training managers, including those at the Sydney and Gold Coast airports, had not incorporated compromised separation scenarios where aircraft are operating below the MVA at night at the time of the Sydney occurrence.
Several Sydney controllers interviewed by the ATSB for the current investigation stated that the provision for controllers to use safe sectors would improve safety by providing compliant options to reduce the risk of unsafe proximity without increasing the risk of terrain/obstacle collision.
This section details the context around the flight operations aspects of the occurrence, including personnel, aircraft information, procedures, and flight crew training. Unless otherwise specified, document references are from the version current at the time of the occurrence.
Both 737 flight crew members held an air transport pilot licence (ATPL) aeroplane and Class 1 aviation medical certificate. They reported no recent or ongoing medical or personal issues likely to have influenced their performance.
The captain had about 19,017 hours of aeronautical experience, including 13,680 hours on 737 variants. The captain reported feeling alert at the time of the occurrence.
The first officer (FO) had about 7,710 hours of aeronautical experience, including 1,460 hours on 737 variants. The FO reported feeling a little tired at the time of the occurrence. They reported getting a normal amount of sleep in the nights before the occurrence. ATSB analysis indicated that the FO was probably not experiencing a level of fatigue known to have an adverse effect on performance.
Both A330 flight crew members held an ATPL aeroplane and Class 1 Aviation medical certificate and were appropriately qualified to conduct the flight.
The A330 captain had a total of 19,100 hours flight time, with about 335 hours on A330 variants. They reported feeling fully alert at the time of the occurrence.
The FO had a total of 12,105 hours flight time, with 2,945 hours on A330 variants. They reported feeling fully alert at the time of the occurrence.
ATSB analysis indicated there was a low likelihood that either A330 pilot was experiencing a level of fatigue known to have an adverse effect on performance.
The 737 flight management computer (FMC) contained a navigation database that included most of the information presented on navigation charts as well as additional data used for navigation. Lateral navigation guidance (LNAV) and vertical navigation guidance (VNAV) could be coded using the FMC and displayed on flight instruments.
Typically, flight crews can program the FMC with arrival routes that join runway approaches to provide continuous lateral navigation guidance. At Sydney, most of the STARs were open, which meant there was a discontinuity between the last waypoint of the STAR and the instrument approach. Once the aircraft reached the end of the STAR route and/or were vectored from the STAR to intercept the instrument approach, LNAV automatically disconnected.
A route discontinuity was displayed on the central display unit (CDU) with an alert message and associated message indications (Figure 12). A flight crew could resolve the discontinuity by entering an adjoining waypoint in the CDU. There was no requirement to do this.
Figure 12 displays an example route legs page with a route discontinuity present indicated by a break in the waypoints and the message ‘route discontinuity’. Also displayed is the joining of waypoints when the discontinuity is cleared.
Figure 12: Example flight management computer route legs page with discontinuity present (top) or cleared (bottom)
The 737 automatic flight system (autopilot) consisted of an autopilot flight director system and autothrottle, in conjunction with a flight management computer and mode control panel.
In normal autopilot operation, the flight director and autothrottle were controlled automatically to fly a pre-programmed and optimised flight path through climb, cruise, and descent.
To select the desired mode, flight crew pushed the applicable mode selector switches, which illuminated when active. Flight mode annunciations were displayed above the attitude indicator on the outboard display unit (primary flight display).
The engaged flight modes were displayed in green letters and armed modes were displayed in smaller, white letters beneath the engaged modes. A highlighting rectangle appeared around the relevant mode annunciation for a period of 10 seconds following mode engagement.
To manoeuvre the aircraft in a missed approach, the following modes could be used:
lateral navigation (LNAV)
heading select (HDG SEL)
go-around (GA).
A standard rate turn was at a 25° bank angle, and the flight crew could also select other bank angles up to 30°.
Lateral navigation mode
To engage LNAV in flight, an active route must be entered in the flight management computer. LNAV will automatically disconnect on reaching a route discontinuity or when other modes such as HDG SEL are engaged.
When LNAV mode is selected, flight director roll is commanded to intercept and track via the active route. This route can include airways, SIDs, STARs, instrument approach and missed approach path.
When conducting an instrument approach, following localiser (LOC) capture the roll (lateral) mode window will display LNAV in white (armed), providing the engagement criteria in flight is met. This visual display is the only indication to pilots that LNAV guidance will be available during a missed approach (Figure 13).
Figure 13: 737 indications on ground-based augmentation system landing system (GLS) approach displaying when LNAV becomes armed
Source: Qantas Airways, annotated by the ATSB
Heading select mode
The HDG SEL mode commands a turn to the heading selected by the pilot on the mode control panel and maintains that heading.
Go-around mode is engaged by pushing either of the take-off/go-around (TOGA) buttons. An autopilot go-around can be conducted in certain conditions or flight crew can carry out a manual flight director procedure.
In the manual procedure, with the first push of either TOGA button:
autothrottle (if armed) engages and advances thrust to produce 1,000 to 2,000 ft/min rate of climb
pitch mode engages in TOGA
flight director commands pitch 15 degrees nose up until reaching programmed rate of climb.
roll mode maintains existing ground track and, above 400 ft radio altitude, LNAV will engage (if TOGA to LNAV equipped and no route discontinuities after missed approach point).
Above 400 ft, the flight crew can terminate the go-around mode by selecting a different pitch or roll mode.
In accordance with regulatory requirements, the 737 and A330 were each equipped with an advanced traffic alert and collision avoidance system (TCAS). This system operated independently of air traffic control (ATC) by using on-board surveillance capability to detect other transponder-equipped aircraft. The relative position of aircraft were presented as coded symbols on the TCAS display with two levels of traffic alerting:
Traffic advisory (TA) for potential collision threats (40 seconds from closest point of approach) – aural message ‘TRAFFIC, TRAFFIC’, and TRAFFIC annunciation on the display
Resolution advisory (RA) for real collision threats (25 seconds from closest point of approach) – aural message with vertical guidance, and corresponding annunciation on the display.
In most encounters, two aircraft will declare the other to be a threat at slightly different times.[32]
All RA are inhibited below approximately 1,000 ft above ground level (AGL) and all TCAS aural alerts are inhibited when below approximately 500 ft. This is to ensure that alerts are not generated during certain phases including initial take-off climb and go-arounds for two reasons: to avoid distracting the flight crew at a critical phase of flight and, because the aircraft is already flying close to the performance limit (body angle/attitude and thrust).
An example TCAS RA indication showing the relative location of a ‘threat’ aircraft (in amber) on an Airbus navigation display is shown in Figure 14. In this display, the other aircraft is ahead, to the right, 600 ft above, and descending.
Qantas arranged for the A330 TCAS computer to be analysed. A review of the recorded data showed that during the occurrence the A330 received a TA without any RAs. The 737 flight data did not record traffic alerts.
Both the A330 and 737 were equipped with an enhanced ground proximity warning system (EGPWS). The purpose of the EGPWS is to warn the flight crew of potentially hazardous situations, such as a collision with terrain. It detects terrain collision threats and triggers aural and visual indications.
The AIP described the procedure for a missed approach (go-around) from a visual approach:
In the event that an aircraft is required to go around from a visual approach in VMC, the aircraft must initially climb on runway track, remain visual and await instructions from ATC. If the aircraft can not clear obstacles on the runway track the aircraft may turn.
The exception to the above procedure is that, at Sydney, visual go arounds must be carried out:
a. In accordance with the GLS or ILS missed approach procedure for the runway the aircraft is using, or
b. As directed by ATC.
In this case, the missed approach procedure for the GLS runway 34R approach (used by the 737 crew) required flight crew to maintain runway track (335°) and at 600 ft turn right, track 070° and climb to 2,000 ft (Figure 2).
The Jeppesen and Airservices instrument approach charts depicted the missed approach path for runway 34R tracking straight ahead until well north of the departure end of runway 34R before the right turn (Figure 2). Missed approaches initiated before or at the missed approach point will reach the mandatory 600 ft right turn well before the turn depicted on the chart.
That point in an instrument approach procedure at or before which the prescribed missed approach procedure must be initiated in order to ensure that the minimum obstacle clearance is not infringed.
For instrument landing system (ILS) and GLS approaches, the point of intersection of an electronic glide path with the applicable decision altitude is used to determine the missed approach point. The location of a missed approach point varied depending on a number of factors, and there was typically no fixed missed approach point in published approach procedures. However, operators could pre-program a missed approach point into aircraft navigation computers to help flight crews manage this phase of flight (particularly when commencing a missed approach before reaching the missed approach point); see Flight management computer missed approach waypoint.
In practice, the missed approach point is the last point that flight crew need to decide to conduct a missed approach when they have not made visual contact with the runway. However, missed approaches can be conducted after the missed approach point for other reasons, including obstructed runways or any issue making a normal landing difficult.
In the context of instrument approaches, the AIP stated:
In executing a missed approach, pilots must follow the missed approach procedure specified for the instrument approach flown. In the event that a missed approach is initiated prior to arriving at the MAPT [missed approach point], pilots must fly the aircraft to the MAPT and then follow the missed approach procedure.
The 737’s FMC uses predefined waypoints to navigate the aircraft along the approach and missed approach path. The location of the runway 34R threshold is marked in the FMC with waypoint RW34R.
The missed approach point is the point at which the glidepath intercepts the decision altitude. A reference missed approach point (where the nominal glidepath intercepts the decision altitude) was pre-programmed into the FMC so that flight crews could use it as guidance for following the missed approach procedure. The location of the reference missed approach point could vary depending on the approach type and chart.
After the occurrence, Qantas conducted a review of these waypoints for 9 different approaches to runway 34R and found that 8 of the waypoints programmed into the FMC were incorrectly located at the runway threshold instead of on the final approach path before the runway. These included the waypoint for the approach carried out by the 737 flight crew during the occurrence: it should have been about 0.5 NM before the threshold.
Several controllers interviewed by the ATSB advised there was a recognised variation of aircraft tracking via the runway 34R missed approach path.
Figure 15 shows a composite of recorded runway 34R missed approach tracking (in red) between July 2017 and March 2019 illustrating how the paths can cross or converge with typical aircraft tracks following the MARUB SIX SID (grey). A small number of tracks also crossed the ENTRA FIVE SID.
The OJTI reported that in their experience with similar situations to the occurrence, even with 5 NM spacing, a missed approach still results in conflict.
Figure 15: Aircraft tracks for runway 34R missed approaches (red) compared with tracks following the MARUB SIX and ENTRA FIVE SIDs (grey) from July 2017 to March 2019
Some of the variation in aircraft tracking, particularly for missed approaches, is likely to be due to control instructions issued. In addition, this diagram shows all departures and missed approaches, not just those that are concurrent, for which additional data was not available.
The Qantas 737 Flight Crew Operations Manual (FCOM) contained a procedure for the conduct of a missed approach. That procedure included the following actions required above 400 ft:
Above 400ft, verify LNAV or selected HDG SEL as appropriate [pilot flying]
Observe mode annunciation [pilot monitoring]
Verify that the missed approach route is tracked [both pilots]
The Qantas 737 Flight crew training manual (FCTM) provided supplementary guidance to flight crews on the management of all engines operating go-arounds and missed approaches. It provided the following advice when using the flight director:[33]
If a missed approach is required following a single autopilot or manual instrument approach, or a visual approach, push either TO/GA [TOGA] switch, call for flaps 15, ensure/set go-around thrust, and rotate smoothly toward 15° pitch attitude. Then follow flight director commands and retract the landing gear after a positive rate of climb is indicated on the altimeter.
The TO/GA roll mode maintains existing ground track. Above 400ft RA [radio altitude], verify that LNAV is engaged for airplanes equipped with the TO/GA to LNAV feature, or select a roll mode as appropriate.
Note: Route discontinuities after the missed approach point will prevent the TO/GA to LNAV function from engaging.
The FCTM also contained information on how to manage initial manoeuvring if required by a missed approach procedure. It stated:
If initial manoeuvring is required during the missed approach, do the missed approach procedure through gear up before initiating the turn. Delay further flap retraction until initial manoeuvring is complete and a safe altitude and appropriate speed are attained.
The Qantas Flight administration manual (FAM) described the preferred method for flight crew to manage automatic flight management systems. It highlighted that while automation can be a valuable tool for flight crew, a good understanding of the systems and an awareness of the flight modes was required.
To maintain a positive awareness of the automation system status, and to ensure that both flight crew had a shared understanding of any mode changes, standard operating procedures (SOPs) outlined in the FAM were to be applied. This included a number of standard calls and procedures.
The most relevant procedure to this occurrence was the verbalisation of any changes to the flight mode or autopilot status. In most situations that entailed a call by the pilot flying acknowledging that a change had occurred followed by a ‘checked’ confirmation call from the pilot monitoring. The flight crew did not recall verbalising these calls.
During recurrent simulator training and checking, pilots had opportunities to practice go-around procedures, including go-arounds with one engine inoperative, and with all engines operating. All Qantas pilots were required to demonstrate proficiency in go-arounds biannually. Qantas advised that in the 3 years prior to the occurrence there were no cyclic training go-around exercises conducted specifically on Sydney runway 34R for pilots on the 737 fleet.
The 737 captain recalled flying the runway 34R missed approach some years prior in the simulator. At that time there had been a number of aircraft overshooting the 2,000 ft level off altitude which increased risk of a loss of separation with overflying aircraft. As such, the training emphasis was on the threat being not capturing the low altitude level off.
The 737 FO advised that they had not flown the Sydney 34R missed approach procedure in the simulator and had only conducted one go-around in the aircraft. That go-around was conducted at Melbourne Airport in day VMC and the procedure required the pilot to fly straight ahead on runway track and climb to 4,000 ft.
The ATSB reviewed the 737 captain and FO’s training records and found both pilots had met the competency standard for one engine inoperative and all engines operating go-arounds.
Both the 737 and A330 aircraft involved in the occurrence were fitted with a flight data recorder (FDR) and cockpit voice recorder (CVR) as required by legislation.
The CVR data recorded during the occurrence was overwritten during subsequent operation of the aircraft. Both FDRs included data over the period of the occurrence.
On the night of 5 August 2019, aircraft landing and taking off from runway 34R were controlled from the Sydney air traffic control (ATC) tower via the ‘aerodrome controller (ADC) – east’ position. That position was operated by a trainee ADC and an on-the-job supervisor.
Following the landing of a Dash 8, the trainee ADC cleared the Airbus A330 to line up and take off while the Boeing 737 was on final approach to land. After realising that runway separation could not be assured, the trainee controller instructed the 737 to go around (conduct a missed approach). During the subsequent missed approach and turn to the right, the 737 came into close proximity with the A330 on its initial climb and turn to the right. This was classified as a ‘loss of separation’ under the ATSB’s occurrence classification system.
The loss of separation and close proximity between the 737 and the A330 was the culmination of a series of events that, individually, would only be minor concerns but collectively resulted in a significant incident.
This analysis first examines the development of the occurrence, and then discusses associated air traffic management and flight operations considerations.
The operational requirements for independent visual approaches (IVA) at Sydney and the instrument approach chart used by the flight crew detailed the speed control requirements for aircraft on approach.
In the initial parts of the approach the 737 flight crew operated at higher speeds than specified for the IVA. The aircraft was well above the maximum speed when 10 NM from the threshold and did not attain the required speed until after the trainee aerodrome controller (ADC) instructed the A330 crew to line up.
Although this did not have any detrimental effect on the 737’s operation (as the approach was stable), it contributed to the reduction of spacing between the 737 and the preceding Dash 8 and gave the trainee ADC less time to process the A330 departure. The flight crew did not advise air traffic control (ATC) of this increased speed, as required by the approach chart, and this probably affected the trainee ADC’s judgement of the amount of time available before the 737 would cross the runway threshold, as detailed in the following section.
Adherence to published approach speed limits aids to improve safety and efficiency by bringing more predictability to arrival sequences. This provides controllers with information used to manage separation standards between aircraft.
Aircraft arriving at Sydney Airport were sequenced for landing by the approach controller, who operated from the terminal control unit (TCU) at the airport. When aircraft were established on approach, they were transferred from the approach controller to the applicable aerodrome controller in the tower—in this case, the ADC position.
The local instructions applicable at the time specified the minimum distance between successive arrivals to runway 34R to be 5 NM. This distance could be reduced in some cases (not below 3 NM) if there was prior coordination between the approach and aerodrome controllers.
In this case, the spacing between the landing Dash 8 and the following 737 on approach was 4.5 NM when the 737 was instructed to contact the tower (ADC), and 4.1 NM when the ADC was first contacted. However, the approach controller had not coordinated with the trainee ADC for the transfer as required by the Sydney operational procedures.
The director controller did not later recall details of the arriving aircraft and operations in the TCU were described as normal. The sequencing of aircraft arrivals is dynamic and subject to a number of variables such as traffic density, aircraft performance, operator procedures, and environmental conditions.
In this case, the primary factor was the difference in aircraft performance as the aircraft in the approach sequence was a turboprop Dash 8 with a relatively low approach speed compared to the 737. Although the approach controller would have taken this speed difference into account, the Dash 8 was still slower than expected and the 737 was faster than specified for the independent visual approach. Had the 737 been 5 NM behind the Dash 8 and not 4.1 NM when the crew first contacted the ADC, there would likely have been enough additional spacing (about 0.9 NM) and time (about 25 seconds) for the A330 to take off without the 737 needing to conduct a missed approach: the A330 would have been crossing the departure end of the runway at about the same time the 737 would have reached the missed approach point.
Airservices found that Sydney TCU controllers routinely sequenced aircraft arrivals with less than the required 5 NM spacing without prior communication with Sydney Tower, and that this non‑conforming practice had been normalised. While some variability in aircraft spacing is expected in the dynamic Sydney terminal environment and ADCs are required to exercise their judgement as to the suitability of gaps for departures, provision of spacing within parameters generally reduces ADC workload and associated risk of traffic management misjudgements.
Although ADCs had access to radar position information for aircraft on approach, their primary focus was on visual separation of the aircraft on the runway and within 4 NM of the airport. As a result, ADCs may not have time to maintain an awareness of the distance between aircraft on approach. In that context, advance notice from the approach controller of less than 5 NM spacing (in accordance with operational procedures) would help an ADC to plan arrivals and departures and reduce the risk of compromised runway separation and associated go-arounds.
In visual meteorological conditions, the trainee ADC sequenced departing aircraft between arriving aircraft according to visual separation standards with supplementary information, mainly from the air traffic display. Although the distance between the arriving aircraft could be measured on the display, this was a dynamic parameter and required diversion of attention from the primary task of visual separation.
Controllers are expected to optimise traffic flow with minimal delays while still safely managing separation in accordance with the applicable standards. The standard most relevant at this point in the occurrence was the runway separation standard where, in simple terms, only one aircraft at a time was permitted to be on (or over) the runway.
It was permissible to instruct an aircraft to line-up for take-off behind a landing aircraft, but a take‑off clearance could not be given until the runway ahead was clear. In this case, the trainee ADC was required to anticipate the time taken for:
the preceding landing Dash 8 to clear the runway
the departing A330 to become airborne then turn or be clear of the runway required by the following 737
the following (landing) 737 to reach the runway threshold.
Although the 737 was at close to its minimum approach speed by the time the Dash 8 crossed the runway threshold, the spacing had reduced to 3.3 NM. If the approach controller had advised the ADC of the non-conforming spacing, or the ADC controllers were aware that the 737 was faster than the specified approach speed, the trainee ADC and OJTI would have been prompted to pay closer attention to the 737’s proximity when considering the plan for the A330’s departure. The trainee aerodrome controller’s judgement of the spacing between the Dash 8 and 737 was therefore likely affected by incomplete appreciation of their initial spacing and speed difference.
The trainee ADC and OJTI both reported being aware that the spacing between the arriving Dash 8 and following 737 aircraft was less than the specified minimum of 5 NM by the time the Dash 8 crossed the threshold. However, the trainee ADC must have still anticipated that there was a sufficient gap at this time to allow the A330 to depart. It is likely that, having formulated a plan to allow the A330 to take-off between the Dash 8 and 737, and in the absence of knowledge about the 737 not maintaining the specified speed, the gradual reduction in spacing as the Dash 8 approached had not been enough of a prompt for the trainee ADC to challenge their commitment to the plan.
To execute the plan, the trainee ADC expedited the departure of the A330 by lining it up to hold on the runway so the crew was ready to start the take-off roll as soon as the Dash 8 was clear of the runway. The trainee ADC did not consult with the OJTI before initiating the A330 departure and there was no obligation to do so.
In any case, once the Dash 8 was clear of the runway the trainee ADC issued a clearance to the A330 for an immediate take-off, and the crew complied.
As the A330 started to roll the trainee ADC’s attention turned to the 737 on final approach, and the OJTI asked whether the runway separation standard would be met. The trainee ADC correctly assessed that the A330 might not be clear before the 737 passed over the threshold, so instructed the 737 crew to go around (conduct a missed approach) to avoid a runway loss of separation.
This was about 12 seconds after clearing the A330 for take-off. At this point, the 737 was 1.2 NM (2.2 km) from the threshold and the A330 was rolling and accelerating through 60 kt. The trainee ADC had the option to instruct the A330 crew to reject the take-off but (reasonably) wanted to avoid the risks associated with rejected take-offs.
The OJTI advised it was difficult to visually assess aircraft speed at night and there was no speed data for aircraft on the runway. Based on judgement and experience, the OJTI did not intervene and cancel the A330’s take-off clearance because it might have increased the risk to safety of the aircraft.
From that point onwards, although infringement of the runway separation standard was prevented, there was an increased potential for conflict because the MARUB SIX departure and the missed approach procedure both involved low-level right turns onto similar easterly tracks. This required controller intervention. The trainee ADC and OJTI had to maintain separation visually (at night) by judging and anticipating the three-dimensional positions, speeds and flight paths of both aircraft; this was complicated by the fact that both were climbing and turning, both at different rates.
Issues around the procedure design and procedural constraints are addressed in Air traffic management considerations.
When instructed to go around (conduct a missed approach), the 737 crew was required to fly to the missed approach point and then follow the missed approach procedure for the runway 34R GLS approach unless otherwise advised by ATC. As specified on the approach chart, this was an initial track of 335° (runway bearing), then a mandatory right turn at 600 ft onto a 070° track, and climb to 2,000 ft.
As the aircraft would already be climbing before it reached the missed approach point, it would be expected that the aircraft would be above 600 ft at or soon after the missed approach point and then commence the turn. In this occurrence, however, the flight crew did not commence the turn until after this when at 1,100 ft, after they were instructed by the trainee ADC.
The 737 flight crew had an early awareness that separation from the rolling A330 would be marginal and they initiated the missed approach without delay. The initial actions were performed correctly. The crew had briefed the procedure for Sydney, which required the turn to be initiated after the landing gear and initial flap retraction, and for further flap retraction to be delayed. However, the first officer (FO) as pilot flying (PF) inadvertently followed the trained procedure for missed approaches (which was applicable to airports other than Sydney and did not involve an early turn). There were several contextual factors that likely contributed to this relatively late turn.
Missed approaches generally result in a high flight crew workload, particularly when they are manually flown like this one. Research has found that during missed approaches, there is an increase in the number of flight crew errors including flight path deviations (Dehais and others, 2017). Aspects of this missed approach that increased crew workload included a level-off altitude that was lower than typical, and the need for a turn soon after passing the missed approach point.
Another aspect of this missed approach was management of the automatic flight system. For operations at Sydney, Airservices used standard terminal arrival routes (STARs) that did not provide a continuous navigation path from the STAR to the approach. Therefore, in aircraft flight management computers (FMCs), there is a discontinuity in the route leg positions between last waypoint of the STAR and first waypoint of the runway instrument approach.
When the 737 flight crew programmed the assigned STAR and the runway 34R GLS approach they identified the FMC discontinuity. However, once the flight crew was assigned headings to intercept the IVA they did not update the FMC route legs page to have the active waypoint in front of the aircraft’s position. While there was no requirement for the flight crew to do so, this resulted in the lateral navigation (LNAV) mode not engaging during the missed approach.
The FO (as PF) saw that the LNAV mode did not automatically engage as expected when the aircraft climbed through 400 ft. Because LNAV was not engaged, there was no prompt for the FO to turn when reaching the missed approach point. The turn would normally be initiated at 600 ft after this point, but the FO was likely initially confused and distracted by the absence of LNAV, delaying the corrective action (turning manually or through the use of heading select and autopilot).
For the flight director to direct the turn the FO would have needed to select a roll mode such as HDG SEL (heading select). Because this was not done, the flight director guidance remained oriented to the runway track. For the same reason there was also no prompt to turn soon after this, when the aircraft overflew the flight management computer’s (FMC) actual pre-programmed missed approach point (incorrectly located at the runway threshold; see Runway 34R missed approach point coding).
The flight crew did not verify whether the missed approach route was being tracked in accordance with the published procedure. They were probably focussed on the aircraft’s configuration and speed, as well as the 2,000 ft level‑off altitude which they had previously identified as their main threat. The flight director guidance was commanding the FO to maintain runway track, which they followed until the trainee ADC instructed them to turn right about 15 seconds after they passed the missed approach point.
Automatic systems management and automation surprise can pose problems for flight crews. When modes are different from those expected for the flight phase or when modes are neither called out or checked, the flight path can deviate from what is expected. Distractions (such as hesitation over the misremembered procedure on the minimum altitude for flap retraction, and the navigation mode not changing as expected) probably also initially drew their attention away from the need to turn. In this context, and not yet completely certain about the required flight path, it would be reasonable to follow the flight director in the interim.
Another contextual consideration was the diagrammatic depiction of the missed approach on the approach chart. This showed a turn starting beyond the departure end of the runway rather than at or soon after the missed approach point as was probably intended. Although this diagram was not primary guidance for the missed approach procedure, and so unlikely to have contributed in this instance, it potentially provided the crew with a misleading mental model of when the turn would be expected to start.
In summary, the 737’s flight crew workload was high during the initial stages of the missed approach and the turn required by the procedure was not made until the crew were instructed by the trainee ADC. Distractions, an uncorrected route discontinuity, and potentially the depiction of the missed approach route on the approach chart well after the runway, were all potential factors.
Although the non-conforming missed approach alone did not affect the safe operation of the 737 and would not have been a concern in the absence of other traffic, the later turn positioned the 737’s flight path closer to that of the A330.
Throughout the missed approach sequence, the trainee ADC was applying visual separation. In the first phase of the missed approach, the 737 was travelling in the general direction of the tower, and it was after last light, which probably affected both controllers’ ability to visually determine the position of the 737 from the tower.
Another contextual factor was the historical variability in the location of the height-based right turn in the first part of the missed approach (Figure 15 and discussed further in Missed approach and departure procedures). This meant that the tower controllers could not develop a consistent visual reference to aid in their assessment of aircraft conformance to the runway 34R missed approach procedure (since other aircraft they saw likely turned at differing points).
In summary, it may not have been obvious at first that the 737 flight path was not conforming to the missed approach procedure.
From recent discussion of the scenario of an aircraft taking off concurrently with an aircraft going around from runway 34R, the trainee ADC was aware of the potential for compromised separation. The trainee ADC was also aware that an intervention might be required to preserve separation and that vectoring was not permitted at night below the MVA. Instead, the trainee ADC appropriately applied ‘best judgement and initiative’, which allowed controllers to work outside of prescribed actions when the safety of an aircraft may be considered to be in doubt, as in this case.
Observing that the 737 was not turning, the trainee ADC instructed the 737 crew to turn right onto a heading of 100°. This was about 9 seconds after the 737 passed through the 600 ft mandatory turn height, as described in 737 flight path during missed approach. By turning the 737 further than the default 070°, the trainee ADC was intending to direct the 737 onto a flight path that was divergent to the A330 in the process of turning to intercept the 075° radial. The trainee ADC’s likely mental model of the situation at this point is shown in Figure 16.
The trainee ADC’s instruction to the 737 to turn, soon after the aircraft passed 600 ft, was an important factor in keeping the two aircraft apart. However, in the absence of any other intervention, the instruction to turn would not prevent separation from being compromised. As the turn progressed, the 737 flight path was further to the north than the trainee ADC had anticipated due in part to the radius of turn (as a result of the 737’s increased speed since passing the missed approach point). The instruction to turn to heading 100° instead of the 070° specified by the procedure had no effect in the early part of the turn that was critical to separation.
Further, the trainee ADC did not issue the 737’s turn instruction using the phrase required for avoiding action, which would have alerted the 737 flight crew of the potential traffic conflict with the A330 and emphasised the reason for the instruction. As a result, their immediate response was not assured, and the turn was not made at the fastest possible rate. ATSB analysis indicated that a maximum-rate turn probably would have increased the minimum distance between the aircraft to about 0.55 NM (1.0 km). The trainee ADC also did not issue either flight crew with a safety alert to advise of the unsafe proximity situation.
Figure 16: Trainee ADC’s likely mental model of the approximate flight paths the aircraft were expected to take after issuing the instruction for the 737 to turn
Partial flight paths of the occurrence aircraft are shown for comparison (in faint orange and blue).
Source: Google Earth, annotated by the ATSB.
The trainee ADC’s separation model relied on the assumption that the flight path of the A330 would be further north than it was (prior to intercepting the 075 radial). The trainee ADC recalled that the A330’s turn was earlier and tighter than their recollection of other widebody jet aircraft taking off from that runway. Although that was their experience, the flight path was reasonably consistent with typical MARUB SIX departures (see Missed approach and departure procedures and Figure 15).
Although the 737 crew initiated the right turn about 6 seconds after the trainee ADC began issuing the instruction, the A330 also started to turn in accordance with the SID.
The A330 crew received an audible traffic advisory alert from the traffic collision avoidance system (TCAS) and the first officer sighted the 737. An alert was not generated by the 737 TCAS, probably because of differences in the calculations by each system. Shortly afterwards the separation between the aircraft reduced to 0.42 NM (800 m) laterally and about 508 ft vertically. This was the closest proximity during the occurrence.
As stated previously, the trainee ADC was applying visual separation in the terminal area. The Manual of air traffic services (MATS) allowed for visual separation of aircraft in the vicinity of aerodromes only when the projected flight paths of the aircraft do not conflict, with consideration of faster following aircraft, and with ‘wide margins’ when judging relative distance or height due to the possibility of visual errors. The ATSB considered that these conditions were not met, which makes the occurrence a loss of separation.
There are limitations to the human visual system at night (Gibb and others 2010). For example, in the absence of other cues, the apparent size of an object is related to its brightness rather than its image size. As a result, the judgment of distance is extremely difficult at night (Isaac and Ruitenberg 1999). The MATS stated that ‘visual determination of the relative distance of aircraft in close proximity can be in error or affected by optical illusion’.
In the context of having no time to plan for the conflict, the trainee ADC did not make a change, initially, to the flight path of the A330. Although the constraints of vectoring at night also applied to the A330, the trainee ADC had the option to instruct the A330 crew to turn to a more northerly heading. This would have reduced the risk of unsafe proximity without any significant terrain/obstacle collision risk.
About 30 seconds after assigning the initial turn instruction to the 737 crew, the trainee ADC instructed the crew to continue the right turn onto 120° to provide further separation. The 737’s heading was then passing through 022°, and with the disposition of the 2 aircraft and the A330 still turning, this instruction had no immediate effect on separation.
After a further 20 seconds and a transmission from the A330 flight crew to advise that they had passed ‘very close’ to the other aircraft, the trainee ADC instructed the A330 crew to turn left heading 100°. A left turn by the A330 at this time would have increased the gap further. In fact, this heading would have required a right turn from the A330’s current heading (about 070°), indicating that the trainee ADC thought that the A330 had turned further south than it had, and the instruction had limited effect. Nevertheless, the 737 was now ahead of the A330 and travelling faster so the spacing widened.
Following the loss of separation, the trainee ADC transferred the 737 to the approach controller without a separation standard having been established and without coordinating a transfer of separation responsibility with the approach controller. As a result, the 737 was under the control of the approach controller without a required surveillance separation standard.
The trainee ADC was operating under the supervision of a qualified on-the-job training instructor (OJTI) who was responsible for the safety and efficiency of the aerodrome control function for runway 34R. Although the OJTI had the authority to override the trainee ADC, any intervention would have resulted in deferral of the check planned for the next day. In addition, and based on the trainee ADC’s recent performance, the OJTI was expecting the trainee ADC to identify and manage traffic conflicts with minimal prompting and no intervention. The trainee ADC had been operating with similar expectations.
When the trainee ADC instructed the A330 crew to line-up then cleared them for an immediate take-off, the OJTI considered the sequencing of the A330 departure was ‘ambitious’ but this was not communicated to the trainee at the time because there was a possibility the plan could work and would be an opportunity for the trainee ADC to demonstrate a solution. Once the trainee ADC instructed the 737 crew to conduct a missed approach, the OJTI was aware that the aircraft would need to be separated and prompted the trainee ADC to focus on a resolution.
The OJTI reported they would have preferred the trainee ADC to cancel the SID and provide the A330 flight crew with a heading to the right of the runway centreline (such as 030°) to resolve the compromised separation but did not communicate this to the trainee. As described above, the trainee instructed the 737 crew to turn right to heading 100°. The OJTI recalled understanding the trainee’s logic for the instructions, but would not have chosen this strategy to resolve the situation and believed more azimuth could have been provided to the 737.
There were differing understandings between the trainee ADC and OJTI in managing the compromised separation situation. Communications effectiveness depends on shared assumptions, a shared mental model or shared situation awareness (Salas and others 1995). Research in mental models and shared awareness has found that information that is shared in strategic mental models allows team members to have common explanations of the meaning of task cues, make a compatible assessment of the situation, and form common expectations of additional task and information requirements. This shared level of situational awareness allows them to take appropriate actions, whether gathering additional information critical to making a decision, or implementing a particular procedure (Salas and others 1994).
As part of on-the-job instruction of Airservices controllers, a prompting hierarchy is used to guide the performance of the trainee. The purpose of the prompting hierarchy is to assist with determining the trainee’s readiness for a final check with the underlying premise that, in an air traffic control context, the OJTI is maintaining the traffic picture and commences prompting once a potential safety occurrence is identified, and they can then be certain that the trainee has identified the issue, and that the solution is satisfactory.
In this case, after the A330 was cleared for take-off, the OJTI asked the trainee ADC whether the runway separation standard would be met. This successfully prompted the trainee ADC to reassess the spacing between the two aircraft and led to the instruction for the 737 to go around.
The OJTI then prompted the trainee ADC to resolve the separation issue by directing the trainee’s attention to resolving the situation, asking ‘what are we going to do’ and to provide the aircraft with more horizontal separation. From this communication, the trainee ADC likely believed they shared the same understanding of the situation and had chosen the same solution, or at least a feasible one.
However, the OJTI did not use the higher levels to communicate to the trainee ADC the urgency of the situation, did not prompt the trainee ADC to share their mental model of the emerging traffic picture or confirm that the trainee ADC was projecting the flight paths accurately. This also meant that the trainee ADC may not have had sufficient prompts to question their interpretation of the developing situation. It is likely the OJTI was cognisant that the trainee ADC needed to demonstrate competence without intervention, and was reluctant to provide additional instructions to manage and recover from the compromised separation situation effectively.
The OJTI was monitoring the aircraft visually and was confident that they would not collide. However, for the separation of two aircraft at night, it is desirable to have a wide buffer to account for potential errors in judging and predicting flight paths, and the two controllers allowed the distance between the aircraft to decrease without further effective intervention.
As the situation developed and the A330 began turning towards the 737, the controllers’ ability to maintain visual separation began to be compromised and the controllers probably misjudged the proximity and direction of the two projected flight paths. This limitation may be illustrated by the trainee ADC’s instruction for the A330 to turn ‘left’ to heading 100°. With both aircraft heading away from the tower at this point, a left turn would have been an obvious solution to separate them, but this instruction indicated that the trainee ADC’s understanding of at least the A330’s flight path was erroneous. The error was not corrected by the OJTI.
Although the gap was widening by this point, it meant the A330 continued to turn towards the 737 instead of away as intended. While the OJTI’s judgement that the 737 would pull ahead of the A330 in the turn was correct, the separation by the time the flight paths crossed was still only about 0.8 NM (1.5 km) and any unanticipated variation in speeds or flight paths could have resulted in it reducing further.
In the time leading up to and immediately following the occurrence, the tower shift manager (TSM) was engaged in supporting another controller to reduce their workload. After the 737 crew was instructed to go-around, the OJTI wanted to notify the TSM in accordance with accepted practice but could not leave the trainee ADC unsupervised, and could not gain the TSM’s attention.
As a result, the TSM was not aware of the missed approach and separation issue until after the event. This limited the effectiveness of the TSM role as a risk control for the ADC controller position as they could not provide operational supervision to tactically manage the risk.
Airservices is required to design procedures in accordance with international technical standards and the primary principle of safety along with other considerations such as noise, environment, and flight operations and restrictions imposed through the Ministerial direction and Long Term Operating Plan. For safety assurance, segregation of aircraft flight paths reduces complexity and workload for pilots and controllers.
Although each instrument procedure separately met regulatory design requirements, the concurrent use of the MARUB SIX SID and the runway 34R missed approach procedure could result in converging flight paths, depending on the timing and radius of each turn as well as the relative speeds (Figure 17).
Figure 17: Potential aircraft tracks for runway 34R missed approaches compared with tracks following the MARUB SIX SID
Standard-rate turns are taken at 25° bank. All turns in blue, orange and white are shown with a constant 0.8-NM radius, which is a standard-rate turn at 160 kt, or a 1.4-NM radius, which is a standard-rate turn at 210 kt. The red turn has a constant 1.4-NM radius. Partial flight paths of the occurrence aircraft are shown for comparison (in faint orange and blue).
Source: Google Earth, annotated by the ATSB.
Generally, aircraft conducting a missed approach are required to turn once climbing through 600 ft once at or past the missed approach point. The turn point could change depending on the climb gradient and the location and height at which a missed approach is initiated and there was no clear limit on the extent to which an aircraft could continue on the runway heading before initiating the turn.
Missed approaches that commence the turn near the 737’s missed approach point would generally not come as close to the departure paths as in this occurrence, albeit still closer than the 3‑NM (5.6 km) separation standard (the blue track in Figure 17). However, this would require a missed approach to be initiated early enough before that point for the aircraft to have reached 600 ft. A more serious compromise could occur if the missed approach turn is initiated well after the missed approach point, and particularly if the missed approach turn is also wider than the other aircraft’s departure turn (for example taken at a higher speed). Both of these scenarios occurred in this case.
In general, the missed approach procedure was more likely to result in a wider turn than an aircraft on the MARUB SIX SID, because:
an aircraft conducting a missed approach was more likely to have a higher speed, because it would start accelerating from the landing speed and from an earlier point
there was no minimum bank angle required for the missed approach turn, whereas the MARUB SIX SID turn required a minimum 25° bank angle.
Recorded data indicated that the majority of missed approaches from runway 34R followed a similar path to that of the 737, either intersecting with or crossing the typical MARUB SIX SID track (Figure 15). Although there was some variation in where the missed approach turns began, most appeared to have been initiated from above the runway, as the 737 did in this occurrence. These tracks either merged with or came close to the MARUB SIX SID radial or crossed the typical departure track heading south-east to meet the MARUB radial.
Conversely, there was little variation in the MARUB SIX SID tracks, with most aircraft commencing the turn before crossing runway 07/25 and following a similar flight path to the A330 in this occurrence. The ATSB estimated the average track to intercept the MARUB radial was about 100°, resulting in the tracks converging with the runway 34R missed approach heading (070°) at a typical angle of 30°.
As stated previously, the extent of conflict depends on a number of factors. Approach spacing appears to be one of the most important. Air traffic controllers can allow for this by ensuring sufficient initial spacing between the aircraft to reduce the likelihood of a missed approach to prevent a runway separation issue and to reduce the potential for conflict if a missed approach occurs for other reasons. However, if approach spacing is reduced below the minimum, as it was in this instance and as Airservices reported was ‘habituated’ among Sydney controllers, a controller might judge that there is enough spacing to allow a third aircraft to depart between them, in which case:
the risk of a missed approach is increased due to the traffic ahead and
the risk of the runway 34R missed approach path then coming into conflict with the third (departing) aircraft on the MARUB SIX SID also increases due to the initial proximity of the following aircraft.
Therefore, spacing should only be reduced if the aircraft can still be kept apart with minimal, or no, intervention.
In addition, the Flight Safety Foundation (Blajev and Curtis, 2017) recommended avoiding missed approach procedures that had a low first stop altitude and an early turn. These characteristics were both present in the runway 34R missed approach procedure and probably contributed to the 737 flight crew’s workload in this occurrence, increasing the likelihood of a more serious loss of separation.
It is important to note that there were constraints on the manner in which Airservices were permitted to design the departure and missed approach procedures, particularly the Long Term Operating Plan and Ministerial direction associated with it. However, these documents also emphasised that ‘the safety of aviation operations is not to be compromised’ and this occurrence is an indicator that the current departure and missed approach procedures do compromise safety, at least to some extent.
Airservices stated there had not been an occurrence history that indicated systemic risk control shortfalls with the management of MARUB SIX SID and runway 34R missed approach scenarios to indicate that the level of risk was not as low as reasonably practicable. Although it was anecdotally reported that controller intervention due to the potential for conflict between the MARUB SIX SID and runway 34R missed approach procedures occurred 10 to 20 times in a year, and controllers interviewed by the ATSB generally recognised it as a known hazard, a search of the ATSB database found that no comparable occurrences had been reported. This would not account for some other events, such as those that do not result in a loss of separation (due to controller intervention) but were still a separation concern. Also, it was not possible to obtain detailed data on the level of controller intervention, if any, that resulted. Furthermore, low-incidence hazards are still important to control when there is a potential for a catastrophic consequence.
As a result of the potential for conflict with the concurrent use of the MARUB SIX SID and the runway 34R missed approach procedure, a controller needed to modify the flight path of one or both aircraft to maintain separation. The only resolution in this situation would be to issue headings and/or altitude instructions to one of the aircraft (that is, vector the aircraft) to establish divergent tracks and/or altitude spacing. During the occurrence the trainee ADC and the OJTI formulated separate resolution plans, both of which required aircraft to be vectored at low level.
However, this could be problematic at night because the MATS only allowed vectoring below the MVA in daylight. In daytime, vectoring at low altitudes was permitted because flight crews could visually maintain adequate height to avoid ground and obstacle collisions. To do this, controllers could assign terrain clearance responsibility to the flight crews.
Controllers interviewed by the ATSB stated that in line with the requirement for controllers to provide a duty of care in an unsafe situation, their professional judgement was that, when faced with this time- and safety-critical conflict situation, the least-risk option to aircraft was to issue vectors below MVA at night and issue a safety alert for terrain to the flight crew. These controllers were aware this was not in accordance with the MATS but commented that it had become a normalised solution to the hazard.
In the absence of effective, compliant options, these controllers have needed to break a rule under the cover of a general allowance to apply their ‘best judgement and initiative’ to ensure safety. Although the existence of this type of rule is appropriate and allows controllers to manage unforeseen situations using their initiative and experience, this type of rule should not be applied as a normalised solution. Instead, the underlying reasons for conflict should be removed (so that the situation does not, or is very unlikely to, arise) or controllers should be provided with compliant options to resolve them. If vectoring below the MVA is a normalised solution to a known, recurring problem, it needs to be effectively managed and controlled by Airservices at a systemic level.
In 2015, CASA advised Airservices that the air traffic management system should not rely, as a primary means of defence, on vectoring or heading changes below the MVA at night. However, the Airservices standardisation directive reiterating limitations on vectoring at night indicates that this was a tactic that controllers continued to employ, and that Airservices was aware of it. The underlying reasons for controllers to breach this requirement were apparently not identified and addressed, but likely included situations where separation was (or was going to be) compromised and controllers needed to intervene. These situations likely included the concurrent use of the MARUB SIX SID and runway 34R missed approach procedures.
A broadly similar issue had been addressed at Melbourne Airport in 2016 in response to a loss of separation involving a missed approach at night. The ATSB investigation identified that ‘in the event of a simultaneous go-around at night during LAHSO [land and hold short operations] at Melbourne Airport, there was no safe option available for air traffic controllers to establish a separation standard and to ensure a collision did not occur when aircraft were below the minimum vector altitude.’ In response to this occurrence, Airservices implemented strategies (permitted by CASA exemption) that permitted terrain clearance to be maintained when vectoring aircraft below the MVA at night, including controller training and the implementation of a safe sector.
Although related issues existed elsewhere, these safety actions only applied at Melbourne Airport and only under specific circumstances (during LAHSO operations at night).
According to Airservices, the MARUB SIX SID had been published and in operation since about 1997. As discussed above, the issue of the flight path design and reduced separation assurance between the MARUB SID and runway 34R missed approach procedures was generally recognised among Airservices controllers. This is consistent with this trainee ADC having discussed it with at least 2 trainers.
Airservices considered the risk to be effectively managed. However, as noted in previous sections, the ATSB identified a number of limitations with the management of risk for operations involving conflicts between aircraft on the MARUB SIX SID and the runway 34R missed approach. Accordingly, the investigation considered potential reasons why these problems existed and had not been addressed.
Airservices identified and managed risk through operational risk assessments (ORA), and had an ORA specifically for Sydney airport. The ORA identified a mid-air collision as a threat; however, it mostly did not list specific threat scenarios such as the potential conflict between the MARUB SIX SID and the runway 34R missed approach procedure. This suggests that any risk assessment for this scenario, and others, were not recorded and it was not possible to evaluate their validity.
The ATSB found that the generalised ORA defensive barriers had limited effectiveness in addressing risk. Specifically:
Supervision: During normal operations, the Sydney tower shift manager rosters undertook non‑supervisory tasks that restricted their ability to maintain direct supervision of the operating environment and therefore did not ensure the defensive barrier was available.
Compromised separation rules and procedures: Airservices did not have a prescribed procedure or training for managing compromised separation recovery when the aircraft was below MVA at night. In addition, a standardisation directive to controllers prohibited them from vectoring aircraft below the MVA at night.
Safety alerts: Safety alerts rely on the timely recognition and memory by the controller. In this occurrence, no safety alert for traffic proximity or terrain was issued by any controller to flight crew.
Pilot action: the TCAS traffic advisory (TA) and resolution advisory (RA) functions are inhibited at low altitudes, and there are limitations on the ability of pilots to see and manoeuvre to avoid one another at low heights, at night or in instrument conditions. In this case, the 737 flight crew had no knowledge of the intended departure tracking of the A330 via the MARUB SID and the aircraft attitude during the missed approach prevented both pilots from sighting the A330. Meanwhile, the A330 FO was only able to see the 737 when looking back during the turn after a TCAS TA had already activated, and the A330 captain would not have been able to see the other aircraft until after the conflict began resolving.
Previous ATSB and Airservices investigations had identified related safety issues at other locations (notably Melbourne and Adelaide) including scenarios that involve vectoring below MVA at night, compromised separation procedures, and controller training.
In November 2015, CASA wrote to Airservices regarding operations at Melbourne Airport, expressing ongoing concern with a number of issues. Some of these were relevant to Sydney operations and the scenarios discussed in the current report. While safety action was undertaken by Airservices and CASA at other Australian airports to manage local issues, the lessons were not applied on a national level, and not at Sydney Airport.
Airservices likely would have identified suitable risk controls for the MARUB SIX SID and runway 34R missed approach conflict, had it:
broadened the scope of lessons learned at other airports
considered the effects of routine controller non-compliance in the application of arrival spacing which increased the risk of missed approaches on runway 34R
identified variations in tracks of aircraft on the runway 34R missed approach including more northerly flight paths which increased the risk of conflict with aircraft departing on the MARUB SIX SID
considered the reasons for controllers knowingly making a non-compliant action to vector aircraft below the MVA at night to prevent a more serious loss of separation (the prevalence of which prompted a directive to controllers reiterating that this was not permitted)
formally identified and managed the risk.
This could have led to the identification of risk control and mitigation shortfalls and timely action taken to reduce risk. Through proactive and predictive hazard identification processes involving specific scenarios, it is probable that at least some of the risk controls associated with the MARUB SIX SID and runway 34R missed approach conflicts would have been improved, particularly in terms of compromised separation procedures at night.
Key aspects of this occurrence, including sequencing of arriving and departing traffic and recovery from compromised separation, were taught to controllers through classroom instruction and on‑the-job training, and ultimately checked. Although this trainee ADC’s training was reported to have been somewhat disjointed and lacking continuity of trainers (likely as a consequence of trainee or OJTI unavailability), there was no evidence to indicate any deficiencies with this training and the trainee ADC had demonstrated capability to manage traffic without missed approaches.
The trainee ADC had completed the required compromised separation training for Sydney Airport and was expected to be aware of the higher risk scenarios, recognise potential conflicts, and issue instructions for deconfliction and safety alerts to flight crews. Within the aviation industry, incorporating scenarios within training has been used extensively with flight crew (Fowlkes and others 1998). The potential for conflict between the MARUB SIX SID and runway 34R missed approach procedures had been discussed in the trainee ADC’s check about 2 weeks before the occurrence and reviewed with the OJTI prior to the occurrence.
Although the trainee ADC had been made aware of this potential conflict and challenge to keep aircraft separated, especially below the MVA at night, the delivery of this information relied on the individual trainers and, to some extent, whether relevant scenarios arose during training. This meant that trainees would not necessarily be exposed to this scenario or others requiring aircraft to be vectored when below the MVA at night. While it is not possible to present every conceivable variety of scenario, controllers should be presented with scenarios that they have a realistic chance of encountering and presents a significant risk, especially if the only option for resolution is non-compliant.
There are a number of potential benefits in providing tower-specific compromised separation simulator training. It could provide a valuable opportunity for controllers to apply and trial compromised separation recovery techniques, in a controlled training environment, for the airspace on which they are endorsed, and with aircraft types with which they are familiar.
In summary, although Airservices provided compromised separation recovery training for Sydney tower controllers, this did not include scenarios involving aircraft below the minimum vector altitude at night.
Following the occurrence, Qantas conducted a review of the 737 FMC database for Sydney runway 34R approaches. The review determined that in all but one instance, the location of the missed approach point was at the runway threshold, the same location as the published RW34R waypoint. This did not conform to the published instrument approach procedures, where the missed approach point would be along the approach path before the runway.
Detection of this discrepancy would only be highlighted to flight crew after a thorough check of the FMC data compared with the missed approach point as published on the chart for the approach being flown.
In the case of the runway 34R approach, the erroneous waypoint location could lead flight crew into delaying the commencement of the right turn (if already at 600 ft) by up to 0.5 NM for the GLS approach.
In this instance, given LNAV did not automatically engage, displacement of the missed approach point did not contribute to the occurrence. It did, however, have the potential to confuse the flight crew and might explain some of the non-conforming missed approach paths recorded by Airservices.
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the close proximity involving Boeing 737 VH-VZO and Airbus A330 VH-EBJ at Sydney Airport, New South Wales, on 5 August 2019.
The spacing between the landing Dash 8 and the following 737 on approach reduced to less than 5 NM without the required coordination between the approach controller and aerodrome controller position prior to transfer.
After the missed approach was initiated, the on-the-job training instructor’s prompts to the trainee aerodrome controller were at the lower level of the prompting hierarchy and did not reflect the potential criticality of the situation or elicit an effective response.
Although Airservices Australia applied operational risk assessments to high-level threats, it did not formally assess and manage the risk of specific threat scenarios. As a likely result, Airservices did not formally identify and risk manage the threat of separate aircraft concurrently carrying out the MARUB SIX standard instrument departure and a missed approach from runway 34R at Sydney Airport, even though it had been a known issue among controllers generally. (Safety issue)
The tower shift manager (TSM) was fully engaged in a controller function and was not aware of the missed approach and development of the compromised separation until after the event. This negated the TSM role as a risk control and increased the risk that a compromised separation would not be managed effectively.
The missed approach points pre-programmed into the flight management computer of Qantas 737s were incorrect for 8 different approaches to Sydney runway 34R. The missed approach points were located over the runway threshold, which was not consistent with the locations of the missed approach points as determined by the relevant instrument approach charts.
Airservices Australia did not have procedural controls to separate aircraft concurrently carrying out the MARUB SIX standard instrument departure and a missed approach from runway 34R at Sydney Airport while below the minimum vector altitude at night. (Safety issue)
Airservices Australia’s compromised separation recovery training for Sydney tower controllers did not include scenarios involving aircraft below the minimum vector altitude at night. (Safety issue)
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The Airservices Australia MARUB SIX standard instrument departure and the missed approach procedure for runway 34R directed aircraft onto outbound tracks that did not sufficiently assure separation between aircraft following the procedures concurrently.
Safety issue description: Although Airservices Australia applied operational risk assessments to high-level threats, it did not formally assess and manage the risk of specific threat scenarios. As a likely result, Airservices did not formally identify and risk manage the threat of separate aircraft concurrently carrying out the MARUB SIX standard instrument departure and a missed approach from runway 34R at Sydney Airport, even though it had been a known issue among controllers generally.
Safety issue description: Airservices Australia did not have procedural controls to separate aircraft concurrently carrying out the MARUB SIX standard instrument departure and a missed approach from runway 34R at Sydney Airport while below the minimum vector altitude at night.
Safety issue description: Airservices Australia’s compromised separation recovery training for Sydney tower controllers did not include scenarios involving aircraft below the minimum vector altitude at night.
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Airservices advised that it had or would conduct the following safety actions in response to this occurrence:
Standardisation Directive (DIR_19_0039) issued to ensure controllers adhere to the agreed spacing for arriving aircraft as detailed in the Sydney Operational Procedure (LoA_3183) and the requirement to coordinate any reduction to these distances.
Establish an operations manager-led focus group to facilitate joint discussion between the Sydney Tower and Terminal check and standardisation supervisors to foster an increased understanding of shared risk factors.
Group circular reinforcing the arrival and departure spacing requirements, expectations and procedure design objectives.
Issue a safety alert to airlines on the importance of adherence to published missed approaches to increase the understanding of shared risk factors.
Temporary Local Instruction (TLI_19_0340) issued to advise TSMs [tower shift managers] to operate as a stand-alone role and only combine with other roles following a risk assessment.
Redesign the Sydney TSM roster to allocate stand-alone TSM during core hours.
Dehais, F, Behrend, J, Peysakhovich, V, Causse, M and Wickens, CD (2017) Pilot flying and pilot monitoring’s aircraft state awareness during go-around execution in aviation: A behavioral and eye tracking study, The International Journal of Aerospace Psychology, 27(1-2): 15-28.
Fowlkes, J, Dwyer, DJ, Oser, RL and Salas, E (1998) Event-based approach to training (EBAT), The International Journal of Aviation Psychology, 8(3): pp. 209-221.
Gibb, R, Gray, R and Scharff, L (2010) Aviation visual perception, Routledge, London.
Isaac AR and Ruitenberg B (1999) Air traffic control: human performance factors, Routledge, London.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
captain and first officer of the 737
captain and first officer of the A330
trainee aerodrome controller
on-the-job training instructor
director controller
tower shift manager
Qantas Airways
Civil Aviation Safety Authority
Airservices Australia.
Submissions were received from:
the captain of the A330
Qantas Airways
Civil Aviation Safety Authority
Airservices Australia.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Technically, this was before the end of nautical twilight. At this time in the absence of moonlight, artificial lighting or adverse atmospheric conditions, it is dark for normal practical purposes. There was a quarter moon to the north-west.
[2] The approach controller was part of the terminal control unit (TCU) that managed the terminal control area.
[3] Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[4] In this report, bearings are magnetic. At Sydney in 2019, true bearings are about 13° higher than magnetic bearings; for example, 335° magnetic is 348° true.
[6] Ground Based Augmentation System (GBAS), is a satellite-based precision landing system and is recognised by ICAO as a potential future replacement for current instrument landing systems (ILS). The system uses GPS signals to provide aircraft with precise positioning guidance during the final stages of an approach, both horizontal and vertical, which is especially critical during the landing phase of flight.
[7] Decision altitude (DA): a specified altitude in an instrument approach operation at which a missed approach must be initiated if the required visual reference to continue the approach has not been established. The point at which this occurs is known as the missed approach point. The GLS runway 34R approach chart specified 2 DAs according to aircraft performance. For this operation, the applicable DA was 220 ft.
[9] The flight director generates pitch and roll indications and commands to maintain the desired flight path, either through visually guiding the flight crew’s manual control inputs or commanding manoeuvres through the autopilot.
[10] This radial passes about 0.7 NM past the northern threshold of runway 34R and almost crosses the intersection of runway 16R/34L and runway 07/25.
[11] Image sourced from Airservices PC Replay reproduction tool and modified for display purposes. It does not necessarily reflect the screen viewed by the controllers during the occurrence. The separation measurement can be applied at any time by a controller and was added to the replay as an example. There are also symbols on the display background that provide distance references on approach.
[12] The approach reference speed (Vref) was 144 kt; the flight crew selected 149 kt as the approach speed (Vapp).
[17] Controllers were not permitted to issue a ‘track extended centreline’ instruction to aircraft departing runway 34R.
[18] Traffic advisory aural annunciations are inhibited when the aircraft is less than 500 ft (+/- 100 ft) above ground level. The inhibit status was recorded, and the annunciation occurred about 6 seconds after the inhibit ceased to apply.
[19] The ATSB calculated that had the 737 made the same turn but commencing at the missed approach point, and with both flight paths otherwise identical, the minimum separation would have been about 1.4 NM (2.6 km).
[20] The applicable standard was either 3 NM (5.6 km) horizontal separation or 1,000 ft vertical separation.
[21] MATS is a joint document of Defence and Airservices and is based on the rules published in Civil Aviation Safety Regulations Part 172 – Manual of Standards and International Civil Aviation Organization standards and recommended practices, combined with rules specified by Airservices and Defence.
[23] Sydney Operational Procedures Letter of Agreement (LoA_3183), version 32, effective 8 August 2019.
[24] The terminal control unit provides air traffic services within the terminal control area.
[25] Wake turbulence: turbulence from wing tip vortices that result from the creation of lift. Those from large, heavy aircraft are very powerful and persistent, and are capable of causing control difficulties for smaller aircraft either following or below.
[27] Airservices Australia. The Long Term Operating Plan for Sydney (Kingsford Smith) Airport and Associated Airspace, 1996. Available at https://sacf.infrastructure.gov.au/ltop.
[29] Corporate integrated reporting and risk information system. The system Airservices uses to capture safety, environment and risk management information, including occurrences.
[30] Loss of separation and radar vectors below minimum vectoring altitude involving Saab 340B, VH‑OLL, Boeing 737, VH‑YVC, and Airbus A320, VH-VNH near Adelaide, South Australia on 18 May 2015 (AO-2015-054).
[31] Unsafe proximity and radar vector below minimum vector altitude involving a Boeing 777-31HER, A6-EBU, and two 737-838s, VH-VXS and VH-VYE, Melbourne Airport, Victoria, on 5 July 2015 (AO-2015-084).
[32] Federal Aviation Administration (2011). Introduction to TCAS II, version 7.1.
On 11 October 2018 a Qantas Airways Boeing 737-800, registered VH-VZD (VZD) was inbound to Brisbane, Queensland from Melbourne, Victoria on a scheduled passenger flight. Another Boeing 737-800 also on a scheduled passenger flight, operated by Virgin Australia Airlines and registered VH-YFW (YFW), departed Brisbane, Queensland for Proserpine, Queensland. The two aircraft were on reciprocal tracks in the Amberley Queensland airspace when a loss of separation occurred. The aircraft inbound to Brisbane, VZD, was being controlled on the Royal Australian Air Force (RAAF) Amberley (military) air traffic control (ATC) frequency and the aircraft outbound from Brisbane, YFW, was being controlled on a Brisbane (civil) ATC frequency.
What the ATSB found
RAAF Amberley and Brisbane ATC operated non-linked air traffic management systems, which did not share a common display. Between ATC jurisdictions without linked systems information was shared using manual coordination between ATC elements.
The departing aircraft from Brisbane (YFW) entered Amberley airspace without a hand‑off from Brisbane ATC and without instructions to the crew to change to the Amberley frequency. This resulted in YFW monitoring an incorrect frequency on entry to Amberley airspace and Amberley ATC initially unable to communicate with the flight crew.
The Brisbane departures air traffic controller did not hand‑off the departing aircraft YFW until after it had entered Amberley airspace. In addition, just prior to this incident, Brisbane terminal control unit did not advise Amberley ATC of a change in configuration to the terminal control unit consoles. This led to Amberley ATC contacting the incorrect console position at Brisbane ATC once the departing aircraft had entered Amberley airspace, and delayed the opportunity for Amberley ATC to resolve the impending conflict.
Once appropriate communication with Amberley and Brisbane ATC was established, the outbound aircraft was transferred to the Amberley frequency, and the aircraft were initially diverted away from each other, before being re-established on their respective tracks.
What’s been done as a result
Following the occurrence both RAAF Amberley and Brisbane ATC have taken corrective actions to improve communication and coordination between the two units. This has included deploying a dedicated communications pathway between Amberley approach and the Brisbane Departures South air traffic control positions, and implementing an airspace release that controls the risk that short notice deviations present across the non-linked systems.
Safety message
This incident highlights the importance of clear communication and coordination between air traffic controllers operating in different, yet immediately adjacent airspace. Air traffic controllers need to maintain a clear understanding of responsibility for separation assurance, especially when operating without a shared traffic picture. This incident also illustrates the effectiveness of the conflict resolution training received by air traffic controllers in loss of separation events.
The occurrence
What happened
On 11 October 2018 at about 1413 Eastern Standard Time (EST),[1] there was a loss of vertical and lateral separation standards in military airspace near the Royal Australian Air Force (RAAF) Amberley aerodrome, Queensland, involving two Boeing 737-800 aircraft. Prior to the loss of separation the two aircraft were operating in the same airspace but on different frequencies, with one aircraft controlled by RAAF Amberley (military) air traffic control (ATC) and the other by Brisbane (civil) ATC.
Sequence leading to the incident
At 1406 a Qantas Boeing 737-800, registered VH-VZD (VZD), operating as QF618 on a scheduled passenger flight from Melbourne, Victoria to Brisbane, Queensland, was on descent to Brisbane Airport and passing through RAAF Amberley airspace, which was controlled by military ATC. Weather warnings were in place for Brisbane and Amberley airports as a frontal weather system, including thunderstorms, was approaching from the west and moving east. About that time, a Virgin Australia Airlines Boeing 737-800 aircraft, registered VH-YFW (YFW) operating as VA1117 on a scheduled passenger flight, departed Brisbane Airport from runway 19 on an initial heading of 195, and turned right onto a heading of 230 and was on climb to flight level (FL)[2] 180. Due to the convective weather in the area, YFW was unable to use a procedural standard instrument departure, and was flying assigned radar headings provided by ATC. The flight crew advised the Brisbane departures controller that they were unable to make any further turns to the right at that time due to the convective weather.
At 1410, as YFW was approaching Amberley airspace, the Brisbane departures controller provided the RAAF Amberley approach controller with an identification on the aircraft, as required by the procedures in the Manual of Air Traffic Services (MATS): Supplementary South East Queensland.[3] At this time, the Amberley approach controller advised the Brisbane departures controller of the inbound aircraft on air route Y195 (Figure 1). The Brisbane departures controller replied that YFW would be turning right soon. The Brisbane departures controller then asked the flight crew of YFW to advise when they could turn right (north). The flight crew advised they would like to stay on heading 230 for an additional 70 to 80 NM due to the weather. It was around this time that YFW entered Amberley airspace (Figure 1), while still communicating with the Brisbane departures controller.
At this time, RAAF Amberley approach was being controlled by a trainee approach controller under supervision of a training supervisor.
At 1411:56, the Amberley approach controller attempted to contact the Brisbane departures south controller regarding the inbound aircraft VZD but was advised that they were speaking to the incorrect controller due to an earlier Brisbane terminal airspace configuration change (see Brisbane airspace configuration). The Amberley training officer took over from the trainee controller in the Amberley approach position, and about 17 seconds later established contact with the Brisbane departures controller, advising them of the inbound aircraft (VZD). The Brisbane departures controller questioned the assigned altitude of VZD raising concern over the potential conflict with YFW, which was now within Amberley airspace. At this point, the two aircraft were still on different radio frequencies, with VZD on the Amberley approach frequency, and YFW on the Brisbane departures frequency.
Figure 1: Position and direction of the two aircraft when VH-YFW entered Amberley airspace at 1411:44. The red line indicates the boundary between Brisbane airspace (right) and Amberley (left) airspace. Air route Y195 was assigned to VH-VZD.
Source: Airservices Australia – modified by the ATSB
At 1412:20, the Brisbane departures controller advised the Amberley approach controller that YFW would contact them for separation, and at 1412:29 instructed the flight crew of YFW to contact Amberley approach. Around this time, the Brisbane ATC display presented a short term conflict alert (STCA) to the Brisbane departures controller. At about the same time the Amberley approach controller issued a safety alert[4] to VZD and instructed the crew to turn left (north). Upon contact with YFW at 1413:10, the Amberley approach controller issued a safety alert and instructed them to turn to left (south). After both aircraft had turned and separation recovery actions were complete, VZD resumed its descent into Brisbane and YFW continued its flight to Proserpine.
Both aircraft were fitted with a traffic collision avoidance system[5] (TCAS) which would have assisted in providing separation instructions to the flight crew in the event ATC were unable to resolve the situation.
Airspace information
The red line in Figure 1 shows the delineation between Brisbane and Amberley airspace. The local coordination procedures between Brisbane and Amberley ATC are described in the MATS: Supplementary South East Queensland. This document included the following:
the hand-off of (aircraft) must be initiated prior to 5 NM (9.26 km) of the boundary
when runway 19 is in use, the standard assignable level is FL 130 for aircraft on approach to Brisbane on the air route Y195, through Amberley airspace
Brisbane Terminal Control Unit (TCU) are to advise Amberley of any changes to the position of Brisbane departures south. This includes if it is merged with Brisbane approach south or Brisbane departures north.
Brisbane and Amberley ATC used different air traffic management systems to control their airspace. These systems were not linked and did not display the same information, so the Amberley controllers did not get details of aircraft which were not entering their airspace as the details were not entered by their planning function. The Brisbane controllers were required to contact the Amberley controllers to provide them an aircraft’s identification and basic details if the aircraft was approaching the boundary between Brisbane and Amberley airspace.
Aircraft hand-off
ATC recordings and interviews identified that the Brisbane departures controller originally intended to turn the departing aircraft, YFW, to the north avoiding Amberley airspace. Amberley controllers stated that YFW came further into their airspace than they were expecting, as they were expecting it to turn north based on communications with the Brisbane departures controller. The Brisbane departures controller reported that several previous aircraft had ‘accepted’ turns to the north-northwest.
The Amberley approach controller had not received a hand‑off of YFW when it entered Amberley airspace. The hand-off of YFW occurred after the impending conflict with the inbound aircraft (VZD) was identified by the Brisbane departures controller. The Brisbane departures controller reported that they had expected Amberley to assure separation between the aircraft by assigning VZD to maintain FL 190, however 5 minutes before YFW entered Amberley airspace VZD had been instructed by the Amberley approach controller to descend to FL 130.
Brisbane airspace configuration
Prior to the occurrence, and due to the World Parachuting Championships at Runaway Bay (about 65 km south-south-east of Brisbane Airport), the airspace sectors for the Brisbane TCU were not in the usual configuration. Due to the proximity of the inbound and outbound tracks of aircraft around the parachute operations, one controller was controlling all departures and approaches in the southern area. Due to the weather front approaching, the parachuting championships were put on hold prior to the incident.
About 5 minutes prior to the incident, at about 1407, the Brisbane airspace was returned to a more standard configuration, being that the departures controller controlled all departures to the south and north. The Brisbane approach south controller was controlling all aircraft approaching from the south. It was reported that this change, back to the more standard configuration was not communicated to Amberley ATC.
Amberley to Brisbane communication
Amberley approach and Brisbane TCU controllers used three tele-communication lines. These included direct lines to the following sectors: Brisbane approach north, Brisbane approach south and Brisbane departures north. There was no direct line to Brisbane departures south. Brisbane TCU used combinations of sectors whereby the sector of Brisbane departures south was always combined with one of the other sectors. In accordance with agreed procedures, Brisbane TCU was required to notify Amberley when the position of Brisbane departures south changed.
The Amberley controllers stated that they were not aware that Brisbane departures positions had been combined until they contacted the incorrect controller. The Airservices internal investigation stated that the Brisbane TCU did not advise Amberley of the change of configuration. There was approximately 4 minutes and 30 seconds from the time Brisbane departures was combined and the Amberley approach controller contacting the incorrect Brisbane controller.
Workload
The presence of the rapidly moving weather front, including thunderstorms, around Brisbane meant that many aircraft were unable to operate on standard instrument departures. This resulted in an increase in coordination requirements for the air traffic controllers. The Brisbane departures controller had continuous communications with multiple aircraft for approximately 6 minutes prior to the loss of separation.
Separation
Once the two aircraft were operating on the same frequency, they were instructed to deviate from their flight path away from each other by the Amberley approach controller. The two aircraft passed each other and had a loss of separation,[6] where the required separation was 3 NM horizontally or 1,000 ft vertically, and the minimum recorded distances were 2.1 NM and 650 ft.
Safety analysis
The Brisbane departures controller intended to turn the departing aircraft YFW to the north, avoiding Amberley airspace. When YFW did not accept turns to the north, it was unlikely the situation was effectively reassessed by the Brisbane departures controller resulting in YFW entering Amberley airspace without a hand-off. The presence of the rapidly moving weather front likely increased the workload for the Brisbane departures controller due to the increase in aircraft coordination requirements, and this may have influenced the delay in the hand-off of YFW to the Amberley approach controller.
When YFW entered Amberley airspace without a hand-off from the Brisbane departures controller it was operating on a different frequency to Amberley approach and other aircraft in Amberley airspace. This resulted in the Amberley approach controller being unable to effectively manage the multiple aircraft, specifically YFW, in their airspace and therefore reduced their ability to maintain separation standards.
Amberley ATC were not expecting YFW to enter their airspace due to the Brisbane departures controller stating the aircraft would be turning north soon, which was consistent with their actions for several previous departing aircraft. This, combined with the aircraft operating on a different frequency to Amberley approach, resulted in a delay in the Amberley approach controller being able to resolve the impending conflict. The Brisbane departures controller was expecting the Amberley approach controller to assure separation between the two aircraft, but was unaware that VZD was already on descent and therefore in conflict with YFW.
Due to the World Parachuting Championships, the Brisbane Terminal Control Unit (TCU) were not operating in a standard configuration on the day of the occurrence. When the TCU reverted back to a more standard configuration this was not communicated to Amberley ATC as per the agreed procedure. Consequently, this led to a delay in the Amberley approach controller being able to contact the Brisbane departures south controller due to the incorrect position being contacted. Further, this resulted in a delay in the aircraft being transferred to the Amberley approach controller to effect recovery of the compromised separation scenario. The time from configuration change to the Amberley approach controller contacting the incorrect Brisbane position (4 minutes and 30 seconds) suggests that there was an opportunity for Brisbane TCU to advise Amberley ATC of the new configuration prior to the Amberley approach controller requiring contact with the Brisbane departures south controller.
The Amberley approach controller contacting the incorrect controller resulted in a reduction of potential recovery time of 17 seconds before the correct Brisbane controller was reached. Calculations based on the estimated ground speed of both aircraft obtained from Airservices indicate that this 17-second delay led to a reduction in the lateral separation of the two aircraft by approximately 6 km (3.24 NM). This delay in communication between Amberley and Brisbane ATC reduced the amount of time available to recover the impending loss of separation while the aircraft were closing on reciprocal tracks in opposite directions. If this configuration change was immediately relayed to Amberley ATC, it would have allowed the Amberley approach controller more time to resolve the impending conflict between the two aircraft, and separation requirements may have been maintained.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The departing aircraft was not expected to enter Amberley airspace but did so without hand‑off of control from the Brisbane departures controller, resulting in the aircraft operating on a different frequency to the Amberley approach controller and the other aircraft operating in Amberley airspace.
The Brisbane departures controller did not hand‑off the departing aircraft until after it had entered Amberley airspace due to the original intention to turn the aircraft north prior to the airspace boundary.
The Brisbane Terminal Control Unit did not advise Amberley of the changed terminal control unit configuration. This led to Amberley approach contacting the incorrect Brisbane controller once the departing aircraft had entered Amberley airspace, and delayed the opportunity for Amberley approach to resolve the impending conflict.
Safety action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Airservices Australia
As a result of this occurrence, Airservices Australia (civil air traffic control) advised the ATSB that they are taking the following safety actions:
Implementing airspace releases that control the risk that short notice deviations present across the non-linked systems.
Deployed dedicated communication lines between Amberley ATC and Brisbane departures south.
Royal Australian Air Force (RAAF)
As a result of this occurrence, RAAF (military) air traffic control has advised the ATSB that they have taken the following safety actions:
A communications line to Brisbane departures south has been established and commenced operational use.
The relevant parties are working together to implement a solution to ensure separation assurance between Brisbane departing aircraft and Amberley traffic during weather diversions.
Amberley have submitted a documentation change to Airservices Australia to extend the weather colour coding to include the Brisbane TCU/Amberley approach interface.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 15 December 2016, an Airbus A330-202 aircraft, registered VH-EBA and operating Qantas Flight (QF) 652, was on descent to Brisbane Airport, Queensland, arriving from the south-west from Perth, Western Australia. QF652 was sequenced to follow another Qantas Airbus A330-303 aircraft, registered VH-QPG and operating QF62, which was also on descent to Brisbane Airport, but arriving from the north-west from Narita, Japan.
For noise abatement, reciprocal runway operations were in progress at Brisbane, with arriving aircraft landing on runway 19, and departing aircraft taking off from runway 01.
At 0516:25 Eastern Standard Time (EST), the approach controller cleared QF62 to descend to 5,000 ft.
At 0517:55, a Qantas Boeing 737-838 aircraft, registered VH-VXF and operating QF601, (departing Brisbane for Melbourne, Victoria) took off from runway 01 and was tracking to the south-west. At 0519:15, the approach controller cleared QF601 to climb to 8,000 ft.
Five seconds later, the approach controller cleared QF652 to descend to 9,000 ft for separation with QF601 travelling in the opposite direction. The controller advised the crew of QF652 that they would be cleared for further descent once they had passed opposite direction traffic. The controller then also advised the flight crew of QF601 that there would be a short delay at 8,000 ft due to opposite direction traffic above.
At 0520:20, the controller inadvertently cleared QF652 (instead of QF62) to descend to 2,500 ft and conduct an ILS approach to runway 19. The crew of QF652, still on descent to 9,000 ft, read back the clearance and set their assigned altitude to 2,500 ft (which was normal procedure having been cleared for the descent). The crew sighted the opposite direction aircraft out to their right and continued their descent.
About 30 seconds later, the air traffic system identified a discrepancy between the controller-cleared flight level of 9,000 ft and the flight crew-entered altitude of 2,500 ft. The controller received a predicted level mismatch (PLM) alert, which displays as ‘cleared flight level (CFL?)’.[1] The controller asked the crew of QF652 to confirm they were maintaining 9,000 ft, and the crew responded that they were on descent to 2,500 ft as cleared. The aircraft was passing 9,200 ft at this stage. The controller immediately responded ‘no, that was for Qantas 62, Qantas 652 maintain 9,000’. By that time, radar data indicated that QF62 was at 4,900 ft. No read back was heard from the crew of QF62 to the clearance inadvertently issued to QF652.
The flight crew of QF652 reported that they were passing about 8,600 ft, when the controller instructed them to maintain 9,000. The crew stopped the descent and climbed the aircraft back up to 9,000 ft. The crew received a traffic alert[2] for about 5 seconds on the reciprocal aircraft. At 0521:19, the controller cleared the flight crew of QF652 to descend to 8,000 ft and the aircraft subsequently conducted a normal approach to Brisbane.
Figure 1: Traffic disposition and PLM alert
Source: Airservices Australia – annotated by ATSB
Safety analysis
Separation
As the two aircraft passed each other, radar data showed QF652 at an altitude of 9,000 ft and QF601 at 8,000 ft, with 2.3 NM lateral separation (Figure 1). Figure 2 shows QF652 at 8,700 ft and lateral separation with QF601 of 2.6 NM (Figure 2). The incorrect descent clearance resulted in a loss of separation with QF601, where the separation required was 3 NM or 1,000 ft and the minimum separation recorded was 2.5 NM and 700 ft.
Figure 2: Loss of separation
Source: Airservices Australia – annotated by ATSB
Controller comments
The approach controller had been in the position since 0200 and reported feeling alert, well rested and that things were going very well in the minutes prior to the incident in adhering to noise abatement requirements and keeping the traffic moving. The controller commented that between 0500 and 0600 they get busy; departures tend to conflict with arrivals and traffic can be quite complex at times. The controller assessed that their workload at the time was moderate.
The controller commented that when they identify similar call signs, there are techniques they employ such as appending ‘heavy’, or the aircraft’s position in the sequence, to the call sign, but did not do that in this instance. Both inbound aircraft were ‘heavy’ so it would not have helped to resolve the possible confusion.
After giving the clearance (inadvertently) to QF652 that was meant for QF62, both aircraft appeared to descend.[3] When the flight crew read back ‘Qantas six fifty two’, the controller did not identify the mismatch of the data in the aircraft label with the response, possibly because it was the expected response to the clearance instruction.
Flight number call signs
According to the Australian Aeronautical Information Publication (AIP) General 3.4 paragraph 4.17, rules for aircraft call signs include that flight numbers should ‘take into account flight numbers already in use by the operator and other agencies in the intended control environment, operational area or nearby’.
Call sign confusion
The Manual of Air Traffic Services (MATS) 6.2.1.1 Callsign confusion stated:
When similar callsigns may cause confusion you may take action to minimise errors including:
a) emphasising certain numbers/letters;
b) repeating the entire callsign e.g. QANTAS451 QANTAS451;
c) repeating the prefix e.g. QANTAS451 QANTAS;
d) advising pilots that there are aircraft with similar callsigns on frequency; or
e) instructing pilots to use a different callsign either temporarily or for the duration of the flight.
Airservices Australia initiative
After a number of REPCON (confidential reports) related to flight number call sign confusion in the Brisbane area, Airservices Australia (Airservices) established a process to monitor and increase awareness of reported call sign confusion issues. The process involves reviewing the call sign confusion occurrences reported through their internal reporting system and notifying relevant airlines of the reported occurrence. In addition, Airservices provides a ‘call-sign conflict report’ to domestic aircraft operators each month.
Airservices advised that the distribution of the monthly call sign confusion reports to domestic operators was paused in 2016. This was to allow for an upgrade to an improved information system as the basis of the report. However, given a new system has yet to be commissioned Airservices has reinstated use of the previous system, and will continue to distribute monthly call sign confusion reports while working on improvements to the advice provided to industry.
Airservices also commented that a number of current mitigation measures currently exist for pilots and controllers to respond to call sign confusion, including documented AIP and MATS procedures to minimise the likelihood of call sign confusion. Additionally, Australia utilises 'group format' as the preferred means of transmitting call sign/flight number within Australian airspace in an effort to reduce the possible confusion with assigned flight levels or headings.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The controller inadvertently assigned descent to QF652 instead of QF62 due to call sign confusion, resulting in a loss of separation with QF601.
The two inbound aircraft were operating on the same frequency with similar call signs and call sign confusion mitigation strategies were not used by air traffic control.
ATSB comment
According to the article Callsign Confusion, the US Aviation Safety Reporting System (ASRS) receives a large number of reports of call sign confusion, some of which result in losses of separation. The article states that communications technique is pilots’ and air traffic controllers’ primary defence against confusion and that they need to continue to bring call sign problems to the attention of management.
The Skybrary article Call-sign confusion lists contributory factors including:
failure of operator to give sufficient consideration in allocation of call signs
pilot and controller workload
interruption or distraction
airspace and procedure design
traffic density.
Safety message
Air traffic control and flight crew need to be vigilant when they identify the potential for call sign confusion.
Flight numbers are assigned by airlines, some of which operate call sign de-confliction programmes. The ATSB encourages aircraft operators to use these strategies to help prevent similar incidents occurring. Air traffic control is encouraged to consider liaising with airlines to enhance call sign de-confliction programmes.
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
On 9 December 2016, a QantasLink Bombardier DHC-8-402, registered VH-LQG (LQG), departed runway 16 left at Sydney Airport. The aircraft was operating a scheduled passenger flight from Sydney to Tamworth, New South Wales. The captain was the pilot monitoring (PM) and the first officer the pilot flying (PF).[1] At the time of departure, windshear conditions existed in the vicinity of Sydney Airport and because of this, the flight crew used normal take-off power.[2]
When LQG departed, an Air New Zealand Boeing 777-219ER, registered ZK-OKF (OKF), operating a scheduled passenger flight from Auckland, New Zealand, was on descent to Sydney from the east, assigned 6,000 ft by the Sydney Approach controller. The projected routes of the aircraft crossed approximately 11 km east of Sydney (Figure 1) and the Approach controller had assigned OKF an altitude of 6,000 ft to provide separation with LQG, who would be assigned 5,000 ft.
At 1407 Eastern Daylight-saving Time (EDT), LQG became airborne and after passing 500 ft, the PF turned the aircraft to an assigned heading of 090. When this turn was made, the flight crew had the go-around (GA) vertical mode selected on the aircraft flight guidance control panel with the altitude select (ALT SEL)[3] mode. After passing the acceleration altitude[4] of 1,100 ft, the PF requested the PM to select the indicated airspeed mode and a speed of 185 kts. The PM did this and then, at 1407:45, they contacted Sydney Departures while the PF engaged the autopilot.
When the PM contacted Sydney Departures, they reported passing 1,900 ft, heading 090 and climbing to an assigned altitude of 3,000 ft. Sydney Departures identified LQG on radar and instructed them to climb to an altitude of 5,000 ft. The PM read back this instruction and the flight crew correctly updated the autopilot with the new altitude and engaged the ALT SEL mode.
At 1408:12, as the aircraft climbed through 2,600 ft, Sydney Departures instructed LQG to track direct to waypoint KAMBA.[5] The position was entered into the flight management system and the autopilot was set to the lateral navigation mode. The aircraft then commenced turning left towards KAMBA.
At 1408:38, as the aircraft climbed through 3,800 ft (Figure 1), Sydney Departures advised LQG there would be a short delay at 5,000 ft due to traffic above them. This was acknowledged by the PM.
Figure 1: Disposition of aircraft when LQG was passing 3,800 ft direct KAMBA and showing the projected point of crossing.
Source: Airservices Australia, modified by the ATSB
Also, around this time, with the aircraft now tracking to KAMBA, the PF increased the airspeed setting from 185 knots to 210 knots. Almost simultaneously, the autopilot altitude mode changed to capture the assigned altitude.
The adjustment of the airspeed setting, while the autopilot was in altitude capture mode, resulted in the autopilot reverting from altitude capture mode to pitch mode, which meant the autopilot would now not stop the aircraft climb at 5,000ft.
Consequently, the PF decided to disconnect the autopilot and commenced hand flying the aircraft. They pitched[6] the aircraft nose down, to reduce the rate of climb, and simultaneously the PM selected the autopilot indicated airspeed and ALT SEL modes. Once these modes were selected, the PF attempted to reconnect the autopilot so the aircraft would maintain 5,000 ft. Before ensuring the autopilot had reconnected, they became aware of the conflicting traffic (OKF) and obtained its position by referencing the traffic alert and collision avoidance system (TCAS)[7] display. During this time, as the autopilot had not been correctly reconnected, the aircraft continued to climb.
After sighting OKF, the PF looked back at the aircraft instrumentation and observed the aircraft had climbed through 5,000 ft. This coincided with an altitude alert from the autopilot, which indicated that the selected altitude was exceeded. The PF responded by again pitching the aircraft nose down to stop the climb and return the aircraft to 5,000 ft. The maximum altitude LQG reached was 5,600 ft[8] before the aircraft began to descend.
Prior to the altitude excursion, the air traffic control system presented a short-term conflict alert (STCA), to both the Sydney Approach and Departures controllers. In response to the STCA, both controllers monitored the altitude of LQG to ensure the aircraft would maintain 5,000 ft. When the Sydney Departures controller observed LQG continue to climb, they issued the flight crew a safety alert,[9] requested confirmation that the aircraft was maintaining their assigned altitude and issued them a heading instruction to turn away from OKF. The Sydney Approach controller issued the flight crew of OKF a safety alert and instructed them to stop their rate of descent. In response, the flight crew of OKF advised they would level out and reported they were over the top of LQG and would be able to sight them again shortly. During the conflict, the lowest altitude OKF reached was 6,800 ft.
Separation Standards
The Sydney Approach and Departures controllers had anticipated that LQG and OKF would pass with less than the required 3 NM (5.6 km) surveillance separation between the aircraft. LQG subsequently passed approximately 0.5 NM (1 km) behind OKF. As surveillance separation did not exist, 1,000 ft vertical separation was required. In applying vertical separation, using pressure derived altitude information, tolerances need to be applied. When these tolerances are considered, the 1,200 ft displacement between the aircraft was not adequate to apply vertical separation. Consequently, the level excursion by LQG resulted in a loss of prescribed separation.
Operation of Autopilot
In multi-crew operations, standard operating procedures are established to support the principles of crew resource management (CRM). This includes defining the roles of the PF and PM in relation to autopilot selections. The captain of LQG reported that if the autopilot is engaged, the PF will make the autopilot selections. If the PF is hand flying the aircraft, the PM will make the selections, under the direction of the PF. In both sets of circumstances, visual and verbal cross-checks are made to help identify any potential errors.
Pilot monitoring comments:
After they had selected the correct modes, they believed the PF had reconnected the autopilot. At this time, their attention was divided between managing other radio transmissions and monitoring the PF’s actions.
The requirement to maintain 5,000 ft on departure was received regularly and something they monitored closely. In normal circumstances, the autopilot would remain engaged.
The PM advised that they should have been monitoring the PF’s actions more closely.
Pilot flying comments:
They were aware that when the autopilot mode changed to altitude capture, as they used the speed control, the autopilot mode could change to pitch. So, when this occurred, they disconnected the autopilot rather than concentrating on changing the modes with a high rate of climb close to the required altitude.
They thought they had reconnected the autopilot after the PM had reset the modes, but were distracted by looking outside the aircraft for the conflicting traffic and did not confirm the autopilot had reconnected.
Safety analysis
When the PF initiated the speed increase to 210 knots, the autopilot had not commenced capturing the assigned altitude. The speed increase at this stage of flight was reported as consistent with company practice of increasing speed when tracking towards the intended destination.
As the PF increased speed, the autopilot started to capture the assigned altitude. These near simultaneous events resulted in the autopilot reverting to pitch mode. The potential for the autopilot to behave in this manner was known to the flight crew. It is probable that the altitude capture occurred earlier than expected, due to the aircraft’s rate of climb being unusually high. The selection of normal take-off power on departure contributed to this high rate of climb.
The PF became concerned that the autopilot was not correctly configured to maintain the assigned altitude and disconnected the autopilot to hand fly the aircraft. After the PM had selected the correct autopilot modes, the PF, believing the autopilot would successfully maintain the aircraft at 5,000 ft, decided to reconnect the autopilot. They attempted to do this but the action was not successful. The PF did not realise this and the PM did not correctly confirm the status of the autopilot.
It was probable that the PF was distracted with looking for the conflicting traffic, rather than ensuring they had successfully reconnected the autopilot.
The loss of separation subsequently occurred after LQG did not maintain 5,000ft on a track that conflicted with OKF.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The PF increased the aircraft speed at approximately the same time as the autopilot commenced capturing the selected altitude. This resulted in the autopilot mode changing and influenced the PF’s decision to disconnect the autopilot.
The PF did not engage the autopilot correctly and became distracted before ensuring it was connected, resulting in the aircraft climbing through the assigned level. The PM was also not aware that the autopilot had not been correctly reconnected.
Safety Action
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Operator
As a result of this occurrence, the aircraft operator has advised the ATSB that they have taken the following safety action:
Further training was provided to both the PM and PF in the areas of situational awareness, human factors and operational decision-making during high workload scenarios, including a review of aircraft automation technology and procedures. The crew members were also required to demonstrate competency prior to return to flying duties.
Safety message
Maintaining separation in high traffic terminal areas, such as Sydney, requires that flight crews strictly adhere to air traffic control instructions. As highlighted in this occurrence, any deviation has the potential to reduce safety margins.
During this occurrence, the interactions between the crewmembers were not effective in responding and managing the encountered threats and highlights the importance of effective CRM.
CRM is described as the practical application of all aspects of human factors including situational awareness, decision-making, threat and error management, team cooperation and communication.
One important aspect of effective CRM, is related to successful monitoring of aircraft systems and ensuring crewmembers actively cross check each other’s actions. These skills can be improved through standard operating procedures and increased emphasis and practice.
Key flight crew monitoring principles include:
be technically proficient
keep all team members informed
ensure the task is understood, supervised and accomplished
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the Australian Transport Safety Bureau (ATSB) to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation.
On 26 July 2016, the ATSB commenced an investigation into a loss of separation between a Jetstar Airbus A320 registered VH-VFO and an Air Asia X Airbus A330 registered 9M-XXC, near Gold Coast Airport, Queensland.
The Airbus A330 was departing Gold Coast Airport for Auckland, New Zealand while the A320 was arriving from Avalon, Victoria. Both aircraft were in visual meteorological conditions and the flight crews of both aircraft had the other aircraft in sight.
At the request of air traffic control, the flight crew of the A330 reported the A320 in sight and was instructed to pass behind that aircraft and climb. As the A330 climbed, both flight crew received a Traffic alert and collision avoidance system (TCAS)[1] Resolution advisory (RA).[2]Separation reduced to about 600 ft vertically and 0.35 NM (650 m) laterally. The required separation standard was 1,000 ft and 3 NM (5.6 km).
An Airservices Australia (Airservices) internal investigation into the occurrence identified the following safety issue:
Visual-pilot separation is not applied internationally in Classes A, B and C airspace. This may result in pilots of foreign registered aircraft not being familiar with their requirements and obligations when subject to this form of separation.
In response to the identified issue, safety action was undertaken to:
Review the risks of the application of visual pilot separation as applied to foreign registered aircraft. In determining its ongoing feasibility, with these operators, ensure any identified risks are appropriately managed
That review was conducted and resulted in a recommendation to:
Remove PASS BEHIND as a stand-alone phraseology for assigning pilot visual separation. (Note: could still be used in conjunction with other phraseology e.g. MAINTAIN SEPARATION WITH (AND PASS BEHIND).
The review also recommended that the following rule changes be considered in regard to assigning visual separation:
• Changing phraseology from MAINTAIN SEPARATION WITH to MAINTAIN OWN SEPARATION WITH. (alignment with ICAO phraseology)
• Restricting the use of pilot visual separation for jet traffic to sight and follow scenarios. That is, no ‘pass behind’ for jets.
• Limiting the application of pilot visual separation for foreign registered aircraft to sight and follow situations.
Airservices subsequently advised that it intends to implement the review recommendation and also the phraseology rule change described in the first dot point of the review considerations.
The ATSB reviewed the Airservices reports, safety issues and safety actions. Based on this review, the ATSB considered it was unlikely that further investigation would identify any systemic safety issues. Consequently, the ATSB has discontinued this investigation.
On 19 September 2013, the pilot of a Beechcraft B300, registered VH-FIZ, was conducting calibration activities of ground-based navigation aids at Williamtown (Newcastle Airport), New South Wales.
During the calibration activities, the aircraft conducted a 7 NM (13.0 km) orbit around Williamtown. However, the Tower air traffic controller had intended the aircraft to hold south of Williamtown over land. At the same time, other aircraft were approaching Williamtown to land.
VH-FIZ tracked on the 7 NM arc towards, and then across the coast, on a converging path with a formation of four Boeing F/A18 aircraft that were on a visual approach to Williamtown. The formation flew directly below VH-FIZ with less than the required 1,000 ft separation.
What the ATSB found
The ATSB found that the applicability of a general requirement to conduct aviation risk assessments at Department of Defence aerodromes for complex, new, unusual or irregular activities was open to interpretation. This led to an absence of prior planning for the calibration activities, resulting in an air traffic control work-around on the day of the activities that did not address all related safety aspects. One work-around was that airspace over land usually controlled by Approach was transferred to the Tower. The resultant airspace controlled by the Tower was considerably larger than normal, resulting in the Tower controllers having difficulties visually monitoring the airspace and needing to rely on the surveillance display for situation awareness.
An instruction given to VH-FIZ to ‘orbit’ was insufficiently clear, resulting in the pilot misinterpreting it as permission to conduct a pre-planned 7 NM (13.0 km) orbit around Williamtown. As a result of the Tower controller’s assumption that VH-FIZ would remain in the area they intended, the aircraft was not adequately visually monitored by the controllers in the Tower, or monitored on radar by the Approach controller. This removed any chance of early detection of the impending aircraft conflict. When the Tower controller did detect the conflict, clear control instructions were not immediately given to either VH-FIZ or the F/A18s, leading to a loss of separation.
What's been done as a result
The Department of Defence took proactive action to improve the implementation of aviation risk management (AVRM) to ensure that AVRM plans developed for unusual or irregular operations, such as calibration operations, addressed staffing and traffic levels, coordination and workload.
Safety message
Although not guaranteeing the absence of aircraft separation incidents, prior planning for unusual or irregular operations can permit the development of robust air traffic control defences that address the specific hazards of that operation. Aircraft separation safety also relies on controllers issuing specific control instructions to all pilots, along with the provision of timely and relevant traffic information to pilots of aircraft identified to be in conflict.
Williamtown Visual Terminal Chart
Source: Airservices Australia
Context
Background
As a Department of Defence (Defence) airfield, air traffic services at Williamtown, also known as Newcastle Airport, were provided by Defence personnel. Approval had been granted for the operation of a number of civil aircraft, including regular public transport flights. In 2013, there were 16,764 domestic/regional airline movements[15] into and out of Williamtown.[16] In addition to airlines and military aircraft, civilian general aviation aircraft also regularly used the airfield.
Airspace
Williamtown Tower controllers are normally responsible for the Aerodrome Traffic Zone (ATZ) (shown as the dark green area in Figure 1) that includes the circuit area; 5 NM (9.3 km) radius of Williamtown, over land only, from the surface to 1,500 ft above mean sea level (AMSL).
On the morning of the occurrence, the Tower and Approach supervisors learnt that calibration check activities for the instrument landing system (ILS) and the tactical air navigation system (TACAN) would commence at 1100. There were no procedures in place relating to the control and sequencing of the calibration flight. To expedite the calibration activity and reduce the workload of both the pilot and controllers, the Tower and Approach supervisors agreed that VH-FIZ (FIZ) would remain on the Tower controller’s frequency and operate in airspace normally under the jurisdiction of the Approach controller. To achieve this, airspace usually under the control of Approach was released to the Tower. The released airspace, over land within a 12 NM (22.2 km) radius of Williamtown, from the surface to 3,500 ft (light green area of Figure 1), would contain all of the planned calibration runs apart from the two 7 NM (13.0 km) orbits of Williamtown. The latter required FIZ to track over water in airspace controlled by Approach.
The airspace was released to the Tower controller 2 minutes before FIZ became airborne. The pilot of FIZ had been cleared to operate within 15 NM (27.8 km) of Williamtown not above 3,300 ft. However, as the clearance did not specify ‘over land’, the clearance contained the airspace required to complete all calibration runs.
Personnel information
On weekdays, three controllers normally worked in Williamtown Tower – a Tower supervisor, a Tower controller and a Surface Movement controller. On the morning of the occurrence, two additional controllers were present – a training officer and a checking controller. The afternoon shift comprised three controllers – the Tower supervisor, the Tower controller and a newly endorsed Surface Movement controller. All controllers held the appropriate endorsements to provide a Tower control service for aircraft operating within the Williamtown airspace.
A review by the Australian Transport Safety Bureau (ATSB) indicated that the roster for the controllers was unlikely to have resulted in work-induced fatigue.
The primary duty of the Tower controller was to visually separate aircraft. The surveillance display could be used as a separation and situation awareness aid, as long as that utilisation did not detract from the primary duty of applying visual separation. The intent of allowing Tower controllers to use the display to establish or monitor separation was to enable the controller to convert a radar separation standard established by the Approach controller into a Tower visual separation standard for arriving aircraft and vice versa for departing aircraft. The display was not designed to enable Tower controllers to use radar as the primary method of separation between aircraft operating within the ATZ.
The larger than usual volume of airspace released to the Tower controller required the controller to, on occasion, use the display to monitor and separate aircraft, even though they were not trained to use radar separation. Neither the afternoon Tower supervisor nor the Tower controller had ever operated with such a large volume of airspace. They both reported that it had been difficult to see the calibration aircraft and that often binoculars were needed to see FIZ.
Aircraft information
The operator of FIZ provided calibration services to both of Australia’s air navigation service providers – Airservices Australia and Defence. The flight crew included a number of technicians to undertake the actual calibration tasks while the pilot maintained a pre-determined and specific flight path and level.
The four Boeing F/A18 aircraft (F18s) were operated by Defence personnel based at Williamtown. The F18 flight crew operated in accordance with procedures designed to provide separation assurance and contained within the Williamtown Base Standing Instructions (Base SIs), available to both the Defence aircrew and air traffic control (ATC) personnel.
Calibration activities
Both the ILS and the TACAN were designed for use by aircraft in instrument meteorological conditions (IMC)[17] and both provided guidance to aircraft during the final stages of an approach to land. Routine monitoring, ground testing and maintenance ensured that the systems performed within the specified tolerances and that the operational integrity and serviceability of the systems were maintained. Australia-wide, periodic flight testing (calibration) was required to ensure that ground-based aeronautical navigational equipment remained within the tolerances required for the safe operation of aircraft.
The Flight Commander[18] at Williamtown was given 24 working days’ notice that a calibration aircraft would be operating there for a 2-day period. The run sheet for the instrument landing system (ILS) calibration was emailed to Williamtown 2 days prior to the occurrence, but those for the tactical air navigation system (TACAN) were only emailed on the morning of 19 September 2013 (the day of the occurrence). Additionally, the TACAN run sheet was only provided in ‘draft’ to the operational personnel, not to the Flight Commander.
The run sheet for the ILS listed 23 runs and included a copy of the Williamtown visual terminal chart (VTC) with relevant information added. The ILS run sheet indicated that some runs could be deleted, and that runs would not necessarily be consecutive. The run sheet for the TACAN calibration was emailed to Williamtown in draft format, with a note ‘The run numbers are to assist with Pilot/ATC communications, not to indicate the order in which the runs will be completed.’ Although the approaches and manoeuvres were listed as runs, the layout was significantly different to that used on the ILS run sheet. The TACAN runs included two 7 NM (13.0 km) orbits around Williamtown (runs 1A and 1B, the blue broken line in Figure 1) and two approaches to each runway (runs 2A and 2B to runway 30, runs 3A and 3B to runway 12).
At about 1500, when the afternoon Tower shift commenced work, FIZ had completed almost all of the ILS runs, but had yet to commence the TACAN runs.
When run 3B was cancelled and the pilot of the calibration aircraft asked ‘… can we climb up and do the orbit then?’ the Tower controller reported that they expected FIZ would complete a holding orbit. That is, that the pilot would conduct a continuous steady rate turn to remain to the south of the airfield. However, the tracking of FIZ demonstrated that, on receiving the response ‘…affirm climb not above 3,100’, the pilot understood the controller had cleared the calibration aircraft for the 7 NM (13.0 km) orbit around the Williamtown TACAN.
Military operations
Military fast jets and some training aircraft operate predominately in formation where the pilots of two or more aircraft fly in close proximity to each other and operate as a single aircraft with regard to navigation, position reporting and control.[19]
Military aircraft ‘initial and pitch’ circuit procedures were as follows:
For military fast jet and training aircraft, the preferred method of joining the circuit is via a procedure known as Initial and Pitch. The aircraft (or formation) will track to the Initial Point, a point at 5 NM downwind of the runway in use displaced to the dead side, and track inbound at high speeds. At any stage once abeam the threshold of the runway in use, and safe to do so, the aircraft turns (“Pitches”) to join downwind and configures for landing.[20]
The initial point for runway 30 was a position at the intersection of a line aligned slightly north of the runway and the coast to the east of Williamtown (pink cross on both Figure 1 and 2). Base SIs required military pilots to report their position to the Tower controller 30 seconds prior to the initial point as left, right or straight initial – the direction denoting the turn required from their arrival path to align with the landing direction. Traffic information[21] was provided to these aircraft following that report.
Organisational and management information
Coordination
The 453 Squadron Williamtown Flight Standing Instructions (ATC SIs) stipulated that the Approach controller did not need to seek a clearance from the Tower controller for visual approaches to the duty runway for locally-based Hawk and F18 aircraft. They also stipulated that those aircraft on a visual approach would be transferred to the Tower frequency at 10 NM (18.5 km). However, the Approach controller was required to coordinate all traffic that would infringe the ATZ.
To reduce workload when the ATZ was controlled by the Tower controller, voice coordination from Approach to Tower controllers for arriving locally-based Hawk and F18 aircraft was replaced by silent coordination. Silent coordination was conducted by placing the intentions for the aircraft in the data label for the aircraft or formation on the surveillance display, utilising abbreviations listed in the ATC SIs.
Strategic separation assurance
The Manual of Air Traffic Services (MATS)[22] stipulated that separation assurance must be applied. It defined strategic separation assurance as:
Strategic separation assurance is the designing of airspace, air routes, air traffic management plans and air traffic control practices, to reduce the likelihood that aircraft will come into conflict, particularly where traffic frequency congestion or system performance, amongst other considerations, may impair control actions.
Strategic separation assurance was provided at Williamtown and published in the Base and ATC SIs. When issued a visual approach, pilots of locally-based military aircraft were required to remain outside the Tower’s airspace until provided with traffic information on aircraft within that airspace. The normal vertical limit of the Tower’s airspace was 1,500 ft with a requirement that local military aircraft were required to overfly not below 2,500 ft. On the day of the occurrence the Tower’s airspace was increased to 3,500 ft. However, as the operators of the local military aircraft were not advised, the minimum overfly altitude remained unchanged at 2,500 ft. Changing the airspace on the day of the occurrence without changing these requirements, or amending the silent coordination arrangements, negated the documented strategic separation measures applicable to locally-based military aircraft.
Separation
Separation is the concept of ensuring an aircraft maintains a prescribed minimum distance from another aircraft or object. Within controlled airspace, ATC provided separation using standards specified in the Manual of Standards Part 172[23] (MOS 172) and listed in MATS. Although different standards could be used between military aircraft, Williamtown ATC used the MOS 172 standards when controlling civil, or a combination of civil and military, aircraft. Only one separation standard was required to be in place between aircraft at any one time, but another standard had to be established by a controller prior to the current separation minimum being infringed. Controllers normally base the method of separation on operational advantage but the type of separation standard used depends on a number of factors.
The ATC SIs required the Tower controller to separate and sequence circuit aircraft with all arrivals, departures and transits of the ATZ. As well as all aircraft conducting operations in the ATZ, aircraft arriving via the initial point were considered to be circuit aircraft at the initial point.
The methods of separation used by Williamtown Tower controllers were predominately vertical and visual. Although the Tower controller had access to a surveillance display, they were not trained or endorsed to use that equipment for radar separation, and as such, the surveillance standard of 3 NM (5.6 km) did not apply. However, the Tower controller could use the surveillance display to assist with situation awareness and for silent coordination (see the section on Coordination).
The use of one of the two vertical separation standards available to the Tower controller, 500 ft or 1,000 ft, was dependent on the maximum take-off weight (MTOW) of the aircraft being separated. If both aircraft were 7,000 kg MTOW or less, 500 ft could be used. Although the MTOW of the calibration aircraft was below 7,000 kg, the weight of the F18s was considerably higher so the appropriate minimum vertical separation standard between FIZ and the F18s was 1,000 ft.
To determine the altitude of the F18s for separation purposes, the Tower controller could request the pilot of the lead F18 to report when the formation had descended through 2,100 ft (1,000 ft below FIZ).
Two visual separation standards were available to the Tower controller. The use of the visual (pilot) separation standard transferred separation responsibility from ATC to the pilot of an aircraft and required that pilot to ensure that their aircraft remained clear of other aircraft. A number of requirements existed for the use of the visual (pilot) standard, the most relevant to this occurrence were that the pilot of one aircraft had to have reported the other aircraft in sight and the pilot of the other aircraft, if IFR, had to have been provided with traffic information and advised that the responsibility for separation had been transferred.
The visual (ATC) separation standard could be used between aircraft that had been positively identified by the Tower controller visually identifying the aircraft type. Prescribed separation minima could be reduced in the vicinity of airfields when adequate separation could be provided using visual observation and each aircraft was continuously visible by the Tower controller. However, visual (ATC) separation could only be applied when the projected flight paths of the aircraft did not conflict. As long as the calibration aircraft remained over land to the south of Williamtown, the visual (ATC) separation standard existed.
The lateral separation standard of 1 NM (1.9 km) could have been applied to the aircraft if their positions were determined relative to a prominent topographical feature. If the Tower controller has issued positive holding instructions to the pilot of FIZ to hold over land to the south of the airfield, and the controller had established that the aircraft was holding in that position either by sighting the aircraft or by pilot report, the lateral standard would have existed.
Of the separation standards available to the Tower controller, the only applicable standards on the day were 1,000 ft vertical, visual (pilot) or lateral. As the requirements for the visual (pilot) standard and the lateral standard were not in place, 1,000 ft was required between FIZ and the F18s. When the Tower controller identified that FIZ was over water to the south-east of the airfield, they asked the pilot for confirmation that the aircraft was holding to the south. However, if the Tower controller had at that time issued turn instructions to the pilot to re-establish FIZ over land and clear of the projected flight path of the F18s, the visual (ATC) separation standard would have been re-established between the calibration aircraft and the F18s.
Monitoring aircraft
To ensure that separation was maintained, Tower controllers were required to monitor the traffic situation. However, the Tower controller did not monitor the location of FIZ holding to the south and was therefore unaware that the aircraft had crossed the coast and left the airspace under their jurisdiction. Although the Tower controller had requested that the Surface Movement controller monitor FIZ, monitoring an aircraft of that size at that distance was difficult. Additionally, the Approach controller did not monitor the airspace under their jurisdiction sufficiently to observe FIZ crossing the coast.
Compromised separation recovery
If a controller determined that aircraft were, or would be, in unsafe proximity, the controller was required to issue a safety alert, using the following prescribed phraseology:
SAFETY ALERT TRAFFIC (number) MILES OPPOSITE DIRECTION / CROSSING LEFT TO RIGHT / RIGHT TO LEFT (level information).[24]
Although the Tower controller did issue a safety alert to the pilot of VH-FIZ, the correct phraseology was not used, and no safety alert was provided to the F18 pilots.
Supervision
The Tower supervisor was responsible for, among other activities, supervising and coordinating the work of the Tower and Surface Movement controllers, and for maintaining a close working liaison with the Approach supervisor.
The Tower supervisor reported that the calibration aircraft was difficult to see when it tracked to hold south of the airfield and that they had told the Tower controller a number of times to provide clearer holding instructions to the pilot of FIZ as the aircraft did not look like it was holding as expected.
Close liaison was a regular activity for the supervisors to optimise traffic management as the majority of Williamtown Tower traffic was high speed military aircraft, sometimes requiring last-minute sequence changes for operational reasons.
Priorities
The Australian Aeronautical Information Publication (AIP) stated that an aircraft first able to use the airspace in the normal course of its operations would be given priority. However, as the AIP allowed for aircraft engaged in navigation aid checks to be given priority, controllers prioritised FIZ’s operations as much as possible. The prioritisation was achieved by holding departures on the ground and holding arrivals outside the calibration aircraft’s area of operations for short periods of time, then holding FIZ to facilitate departures and arrivals.
Risk management
Defence required the use of aviation risk management strategies across all aviation activities. In line with this, the agency responsible for Defence air traffic services stipulated that any complex, new, unusual or irregular activity required a risk assessment and that treatments be developed for any risks assessed as medium or higher.
Williamtown ATC had in place a number of generic risk assessments and treatments for occasions when less than the required number of endorsed personnel were available to assist decision making while balancing controller workload and safety. Issues requiring consideration included anticipated traffic complexity or unusual activity, complexity of airspace, and experience levels. The documentation provided direction on the number of personnel required and methods for reducing the number or complexity of traffic. Within each assessment, the level of risk had been assessed in line with specific conditions and/or treatments – including staffing and traffic levels, weather, equipment serviceability and airspace configuration. However, there were no risk assessment for increased traffic complexity (such as a calibration aircraft operating to the non-duty runway) or for additional airspace being released to the Tower controller.
Although executive personnel within the Williamtown ATC unit were notified of the calibration flight inspection 5 weeks prior to the event on 15 August 2013, and further details of the proposed inspection were available from an internal Defence website, the Williamtown Flight Commander reported that, as calibration flights occurred a number of times each year at Williamtown, they were not considered irregular activities and therefore did not require the development of a risk assessment or treatment. The Flight Commander noted that initial notification of calibration flights had provided no details.
Previous occurrences
A review of the ATSB database identified three notifications involving a calibration aircraft at Australian airfields in the 7 years prior to, and one shortly after, the Williamtown occurrence. None of these notifications were investigated by the ATSB.
The ATSB research report AR-2012-034 Loss of separation between aircraft in Australian airspace – January 2008 to June 2012, noted that ‘assessing and planning’ or ‘monitoring and checking’ errors were involved with most individual controller actions that contributed to loss of separation (LOS) occurrences. Ineffective management of compromised separation before it became a LOS was categorised as an assessing and planning error. Monitoring and checking errors included controller actions associated with maintaining awareness of traffic disposition and not detecting that the pilot of an aircraft was not complying with an instruction when there was opportunity to detect this.
Additionally, the ATSB report found that about a quarter of LOS occurrences contributed to by ATC actions involved communication errors. These included not passing traffic information to pilots once separation was compromised and not providing clear, timely or urgent instructions to pilots when separation had been lost to ensure that immediate action was taken to avoid other aircraft or re-establish separation.
The research report found that task demands were the most common type of local condition identified in LOS occurrences where controllers were involved – in particular, high workload and distractions. Common in all ATC environments, these local conditions were more common in the Tower environment. Controller knowledge, skills and experience factors were also identified as local conditions in LOS occurrences.
From the evidence available, the following findings are made with respect to the loss of separation between a Beechcraft B300, registered VHFIZ, and a formation of four Boeing F/A18 aircraft that occurred near Williamtown (Newcastle Airport), New South Wales on 19 September 2013. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
The applicability of a general requirement to conduct aviation risk assessments for complex, new, unusual or irregular activities was open to interpretation. [Safety issue]
The absence of prior planning relating to the operation of the calibration aircraft resulted in a work-around that did not address all related safety aspects and negated the existing strategic separation assurance.
The Williamtown Approach controller released airspace to the Tower controller that was considerably larger than that normally controlled by the Tower, resulting in both the Tower supervisor and the Tower controller having difficultly monitoring the airspace visually, and the need for the Tower controller, though not trained in the use of surveillance control, to rely on the surveillance display for separation.
The absence of specific control instructions by the Tower controller to the pilot of VH-FIZ created an opportunity for the pilot to misunderstand the Tower controller's intent in relation to the pilot’s requested ‘orbit’.
The Tower controller did not monitor the flight path of VH-FIZ due to an assumption the aircraft would remain in the area the controller had intended the aircraft to remain, leading to a loss of separation assurance.
The Approach controller did not monitor their airspace sufficiently well to observe VH-FIZ crossing the coast into airspace under their jurisdiction, removing the chance for earlier detection of the loss of separation assurance.
The Tower controller did not provide immediate and clear control instructions to either VH-FIZ or the formation of F18s once the conflict was detected, resulting in a loss of separation with the formation of Boeing F/A18 aircraft flying directly below VH-FIZ with less than 1,000 ft separation.
Safety issues and actions
The safety issue identified during this investigation is listed in the Findings and Safety issues and actions sections of this report. The Australian Transport Safety Bureau (ATSB) expects that all safety issues identified by the investigation should be addressed by the relevant organisation(s). In addressing those issues, the ATSB prefers to encourage relevant organisation(s) to proactively initiate safety action, rather than to issue formal safety recommendations or safety advisory notices.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are repeated separately on the ATSB website to facilitate monitoring by interested parties. Where relevant the safety issues and actions will be updated on the ATSB website as information comes to hand.
Absence of prior planning
The applicability of a general requirement to conduct aviation risk assessments for complex, new, unusual or irregular activities was open to interpretation.
Although the opportunity for Williamtown air traffic control (ATC) to undertake prior planning for the calibration operations had existed in the 24 working days between the initial notice and the activity, no such planning took place. Defence air traffic services stipulated that any complex, new, unusual or irregular activity required a risk assessment. However, as calibration flights occurred a number of times each year, the Williamtown ATC Flight Commander did not believe that such activity required the conduct of a risk assessment. In addition, although Williamtown ATC had in place a number of generic risk assessments and treatments for unusual situations, there were no risk assessment for increased traffic complexity such as that created by the calibration activities.
Prior planning and a risk assessment had the potential to identify the need to increase staffing in both the Tower and Approach areas, provide briefings for ATC personnel and the pilots of locally-based aircraft, and ensure controllers had a thorough understanding of the calibration run sheets prior to the activity commencing. Such prior planning would have incorporated strategic separation assurance considerations.
The Williamtown Approach controller released airspace to the Tower controller that was considerably larger than that normally controlled by the Tower. That resulted in both the Tower supervisor and the Tower controller having difficultly monitoring the airspace visually, and the need for the Tower controller, though not trained in the use of radar separation, to rely on the surveillance display for situation awareness as well as separation. In situations where the location of an aircraft is known (from a position report or from observing a surveillance display), a controller could quickly use the binoculars to locate an aircraft. However, to locate an aircraft at an unknown position, the controller would need to scan the sky, possibly with the assistance of binoculars. Although binoculars were available to the controllers, binoculars could potentially limit the controller’s view. Using binoculars would also have been time-consuming.
During the morning, there had been two additional controllers in the Tower cabin than normal. They were able to assist with monitoring VH-FIZ (FIZ), and a number of the controllers present had experience with the use of surveillance data for monitoring aircraft and providing separation instructions. At the time of the occurrence, only three controllers were in the Tower cabin. One was newly endorsed in Surface Movement control, without having undertaken training in the control of airborne aircraft. The other two controllers present were not trained in separating aircraft with surveillance data.
Williamtown Base Standing Instructions (Base SIs) and 453 Squadron Williamtown Flight Standing Instructions (ATC SIs) contained restrictions and requirements, for both controllers and locally-based military aircrew, to provide strategic separation assurance between arriving locally-based military aircraft and those within the airspace normally controlled by the Tower controller. These specifically required the local aircraft to remain clear of airspace under the Tower controller’s jurisdiction until issued with traffic information. The last minute planning conducted on the morning of the occurrence by two ATC supervisors, though well intentioned, resulted in less than optimal conditions. These included procedures that negated the established strategic separation assurance documented in both Base and ATC SIs, increased traffic complexity, and the need for the Tower controller to rely on the surveillance display when the controller was not trained to use radar separation.
The run sheet provided to ATC for the calibration of the tactical air navigation system (TACAN) numbered each required run and included a note ‘The run numbers are to assist with Pilot/ATC communications, not to indicate the order in which the runs will be completed.’ Had the pilot of VHFIZ (FIZ) used the run number (Run 1A) in the request to conduct the 7 NM (13.0 km) orbit around Williamtown, the Tower controller may not have misinterpreted the pilot’s request with a request to hold south of Williamtown in an orbit – a standard holding manoeuvre that would essentially keep the aircraft in the same area. However, as the only calibration runs requiring 3,100 ft were the 7 NM (13.0 km) orbits of the Williamtown TACAN, the Tower controller’s reported belief that the pilot of FIZ had asked for that altitude to prepare for the next run to runway 30, for which the run sheet indicated a commencement altitude of 1,500 ft, demonstrated that the controller was either not referring to the run sheet or did not understand the run sheet.
If the Tower controller had used run numbers on the data labels for silent coordination, the Approach controller would have had the opportunity to maintain situation awareness of calibration activities. Further, the use of run numbers would have provided cues to the Tower controller. In turn, the Tower controller may then have been more likely to use the numbers in communication with the pilot of FIZ, removing the opportunity for the pilot to misunderstand the controller’s approval to conduct an orbit.
Although prompted a number of times by the Tower supervisor, the Tower controller did not issue specific holding instructions to the pilot of FIZ. Specific holding instructions could have included ‘hold over land to the south of the field’ or to hold over a specific location. Such an instruction would have resulted in the pilot of FIZ questioning their understanding of the approval to conduct an orbit.
Once the pilot of FIZ commenced the 7 NM (13.0 km) orbit around Williamtown, in line with the pilot’s interpretation of the Tower controller’s response to the request, a loss of separation assurance (LOSA) existed between the calibration aircraft and the formation of four Boeing F/A18 aircraft (F18s) tracking for runway 30. Believing that FIZ was holding to the south in an orbit, the Tower controller did not visually monitor FIZ’s position. Instead, the Tower controller relied on the Surface Movement controller to do so while the Tower controller attended to other aircraft.
An opportunity to identify the loss of separation assurance at an earlier point was lost when the Approach controller did not identify that FIZ had crossed the coast, leaving the airspace released to the Tower controller. The Tower controller had not coordinated FIZ’s entry into airspace under the jurisdiction of the Approach controller. However, the Approach controller should have observed the calibrator entering and remaining in airspace under their jurisdiction. FIZ crossed the coast into the Approach controller’s airspace prior to the F18s passing overhead Williamtown and before they were issued with a visual approach. If FIZ had been identified in the Approach controller’s airspace at this stage, the F18s could have been held away to allow FIZ to complete the 7 NM (13.0 km) orbit of Williamtown, or the Tower controller could have been instructed to turn FIZ to re-establish the calibration aircraft over land. When the Approach controller did observe FIZ and realise the potential conflict with the F18s, they immediately contacted the Tower controller and asked that a safety alert be issued.
Once the Tower controller became aware of FIZ’s position to the south-east over water, clear and urgent information was not immediately provided to the pilot to ensure separation and avoidance with the F18s. As the closure speed between the calibration aircraft and the F18s was very high, the opportunity to provide timely control instructions and traffic information was lost when the controller asked the pilot of FIZ to confirm that the aircraft was holding to the south even though the controller had observed the aircraft tracking in a northerly direction south-east of Williamtown. The absence of clear control instructions to either the calibration aircraft or the formation of F18s resulted in a loss of separation (LOS) between aircraft that had not been provided traffic information in relation to the impending conflict. The absence of traffic information in sufficient time and in sufficient detail increased the risk posed by the LOS.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the Department of Defence (Defence)
Airservices Australia
the operator and pilot of VHFIZ.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to Defence, the pilot and operator of VHFIZ and the air traffic controllers directly involved.
Submissions were received from Defence. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
The occurrence
At 1549 Eastern Standard Time[1] on 19 September 2013, a Hawker Beechcraft Corporation B300, registered VH-FIZ (FIZ), was conducting calibration operations at Williamtown (Newcastle Airport)[2] in NSW (Figure 1). While conducting a 7 NM (13.0 km) orbit around Williamtown at 3,100 ft (the broken blue line in Figure 1), a loss of separation (LOS) occurred between FIZ and a formation[3] of four Boeing F/A18 aircraft (F18s). The formation of F18s flew directly below the B300 with less than the required 1,000 ft separation.
The calibration activity involved checking the equipment associated with the instrument landing system (ILS),[4] which was aligned to runway 12,[5] and the tactical air navigation system (TACAN).[6] To complete the calibration, numerous approaches and manoeuvres were required to test the accuracy of the navigational equipment, each referred to as a run. The various planned runs each had a number on a run sheet held by both the pilot of FIZ and air traffic control (ATC).
The Williamtown ATC Tower controller normally had jurisdiction over the airspace within 5 NM (9.3 km) of Williamtown over land (dark green area in Figure 1), from the surface to 1,500 ft above mean sea level (AMSL),[7] referred to as the aerodrome traffic zone (ATZ). Earlier in the day, additional airspace had been released by the Williamtown Approach controller to the Tower controller – over land within a 12 NM (22.2 km) radius of Williamtown, from the surface to 3,500 ft AMSL (light green area in Figure 1).
On the day of the occurrence, the wind at Williamtown favoured the use of runway 30 (marked in orange in Figure 1), so the majority of FIZ’s approaches were to the opposite direction non-duty runway. To reduce traffic complexity, FIZ was permitted to conduct calibration runs while ATC held other aircraft on the ground or outside the airspace released to the Tower controller, while FIZ was held clear of traffic when a mix of military and civil aircraft were required to depart or arrive. The majority of military aircraft arrived via the initial point, marked by a pink cross in Figure 1 (see the section titled Military operations).
Figure 1: Williamtown Tower airspace: Dark green shading shows the usual airspace, light green shows additional airspace on 19 September 2013. An orange arrow indicates the duty runway location and direction. A blue dashed line indicates the intended flight path of VH-FIZ during the aerodrome orbit run. A pink cross indicates the initial point used by military aircraft.
To reduce the need for extensive voice-coordination between the Tower and Approach controllers, Williamtown ATC added information to an aircraft’s data label[8] on the surveillance data display. The information added to a data label, referred to as silent coordination, was visible to both Approach and Tower controllers. For an arriving aircraft, the Approach controller would add arrival type (e.g. ‘T’ for a TACAN) or that an aircraft had reported visual (‘V’). Both the Tower controllers that day (morning and afternoon shifts) had been using the data label for FIZ to indicate the current run number, and, when known, the next run number. However, at 1530 the Tower controller did not include a run number in the data label of FIZ, rather the label indicated that the calibration aircraft was completing a TACAN approach to runway 12 (which was run 3A) and that the next approach would be a 7 NM (13.0 km) orbit of Williamtown (run 1A). Shortly after, the data label was amended to show that the next run would be the second TACAN approach to runway 12 (run 3B).
At 1537, the Tower controller advised the pilot of the calibrator aircraft that, after the next run (that is, run 3B), FIZ would be required to hold to facilitate a number of arriving aircraft. In response, the pilot of FIZ asked ‘on completion of this run would it be possible to join the 7 TAC[9] counter-clockwise orbit 3,100 and would that keep us clear of traffic?’ This referred to run 1A on the TACAN run sheet, although the pilot did not include ‘run 1A’ in the request. The Tower controller responded with ‘standby’.
To enable the calibration of all of the TACAN equipment, the second of each run number (runs 1B, 2B and 3B) required ground-based technicians to switch to the redundant TACAN system. However, there was a delay in the requested switch for run 3B which was increasingly causing a delay to arriving aircraft, so the Tower supervisor told the Tower controller to cancel run 3B and hold FIZ to facilitate the arrivals.
At 1541, on being advised to hold south of the airfield not above 1,500 ft, the pilot of FIZ asked ‘… can we climb up and do the orbit then?’ The Tower controller responded with ‘… affirm climb not above 3,100 (ft).’ Anticipating that they may become busy with other tasks, the Tower controller reported requesting the Surface Movement controller to monitor FIZ.
At 1543, the pilot of the first of the arriving aircraft, a passenger Airbus A320, contacted the Tower controller and was cleared to track from the north of Williamtown to the right base leg of the circuit for runway 30. At the same time, surveillance data showed that FIZ commenced flying in a counter-clockwise direction (run 1A) around Williamtown from a position 7 NM (13.0 km) to the west of the airfield (position 1 on Figure 2).
Figure 2: Williamtown airspace showing the location and track of VH-FIZ and a formation of four Boeing F/A18 aircraft (numbers represent relative locations at the same time – see Table 1)
At 1546, the pilot of the lead aircraft in a formation of three BAE Systems Hawk aircraft (Hawks) contacted the Tower controller east of Williamtown for a visual approach stream landing[10] via ‘straight initial’ (see the section titled Military operations) to runway 30. The Hawks were descending to 2,500 ft, 1,000 ft above the level of the A320, and advised the Tower controller that the aircraft would be deploying brake-chutes[11] on landing.
At the same time, the pilot of the lead aircraft of a formation of four F18s contacted the Approach controller tracking from the west directly to Williamtown on descent to 8,000 ft. At the time, the transponder for the lead F18[12] indicated that the aircraft was descending through flight level[13] (FL) 137. The Approach controller entered silent coordination in the data label for the F18s which indicated that the aircraft would track to overhead the airfield and then to the northeast on a heading. No information on how or if the aircraft would return for landing was included.
At 1545, the Tower controller cleared the A320 to land and at 1546 cleared the Hawks for a visual approach. At the same time, the Tower controller was involved in coordinating personnel to enter the runway after the Hawks landed to retrieve the brake-chutes. The surveillance data showed that, nine seconds later, FIZ crossed the coast tracking in a north-easterly direction, leaving the airspace released to the Tower controller and entering airspace under the jurisdiction of the Approach controller (position 3 , Figure 2).
Shortly before the formation of F18s passed overhead Williamtown at 1547, the Approach controller cleared the F18s to descend to 5,000 ft and track for an arrival via ‘right initial’ to runway 30 involving a right descending turn towards the ‘initial point’ seen in Figure 2 (see the section titled Military operations). The Approach controller then removed the heading from the F18s data label. After the pilot of the lead F18 reported the Hawks in sight, the Approach controller cleared the F18s for a visual approach.
Ten seconds after clearing the F18s for a visual approach, the Approach controller updated the silent coordination on the data label to show that the F18s were making a visual approach via right initial (the F18s were then at position 6 in Figure 2). Nine seconds later, at 1548, the pilot of the lead F18 contacted the Tower controller while descending through 6,300 ft and on a converging track with the track of FIZ.
Twenty four seconds later, as FIZ was maintaining 3,100 ft at 7 NM (13.0 km) to the southeast of Williamtown and about 8 NM (14.8 km) from and 1,100 ft below the F18s, the Tower controller asked the pilot of FIZ to confirm that the aircraft was holding south of the airfield. The pilot responded in the negative and that FIZ was conducting a counterclockwise orbit of Williamtown.
Fourteen seconds later, when the aircraft were about 6 NM (11.1 km) apart, the Approach controller alerted the Tower controller to the need for a safety alert[14] between the aircraft. The Tower controller responded that he had ‘got it’ and 4 seconds later issued a safety alert to the pilot of FIZ: ‘safety alert Toxin Tripod four F18s your 2 o’clock passing through 3,000’. At this time, the lead F18 was descending through 3,400 ft, 5 NM (9.3 km) directly in front of and converging with FIZ. At that time, FIZ was travelling at 230 knots (kt) towards the F18s travelling at 460 kt.
At 1549, as the pilot of FIZ reported the F18s in sight, separation between the formation of F18s and FIZ reduced below 3 NM (5.6 km) with the lead F18 descending through 2,700 ft. Nineteen seconds later, the F18s flew directly below FIZ with less than the required 1,000 ft separation and they advised the Tower controller that they were ‘visual with the traffic that just passed overhead’
Shortly afterwards, the Approach controller resumed the airspace outside 5 NM (9.3 km) Williamtown and above 1,500 ft, and FIZ was transferred to the Approach controller’s frequency for the remainder of the calibration flight. The F18s landed shortly afterwards.
Table 1: Location of VH-FIZ and the F18s at specified times as shown in Figure 2
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
VH-TJM departed Ayers Rock for Alice Springs and VH-LTC departed Alice Springs for Ayers Rock. To ensure separation the Alice Springs air traffic controller assigned a cruising altitude of 5000 feet to VH-LTC and cleared VH-TJM to descend to 7000 ft. He estimated that the aircraft would pass about 40km from Alice Springs and VH-LTC was instructed to report sighting and passing VH-TJM.
Subsequently, at 48km from Alice Springs, VH-TJM was cleared for a visual descent. The air traffic control workload was heavy at the time, but shortly afterwards the controller realised he had not applied a separation standard before allowing VH-TJM to commence the visual descent. He contacted both aircraft for position reports which revealed that they had passed safely and were about 20km apart. Fortuitously there was no confliction.


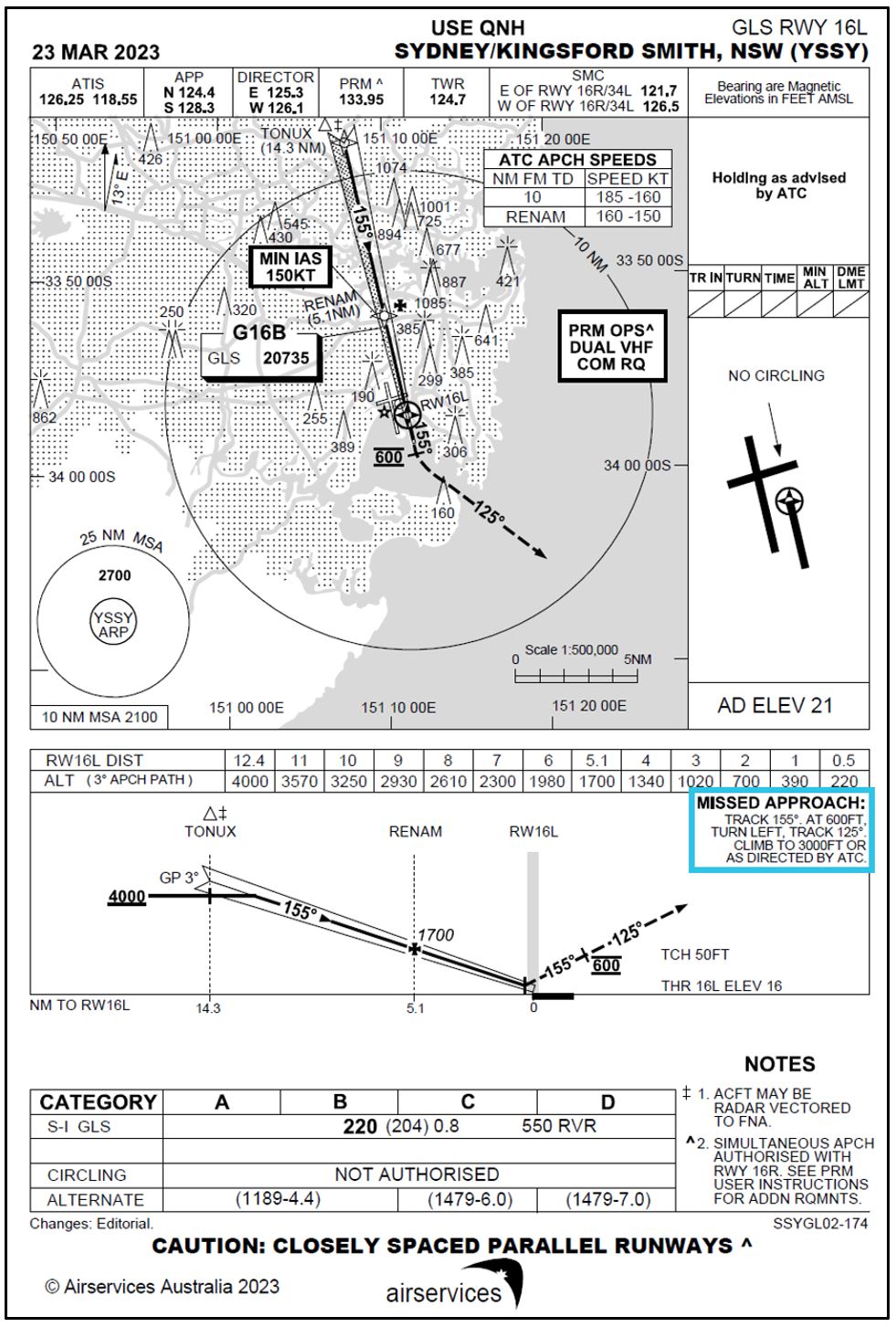

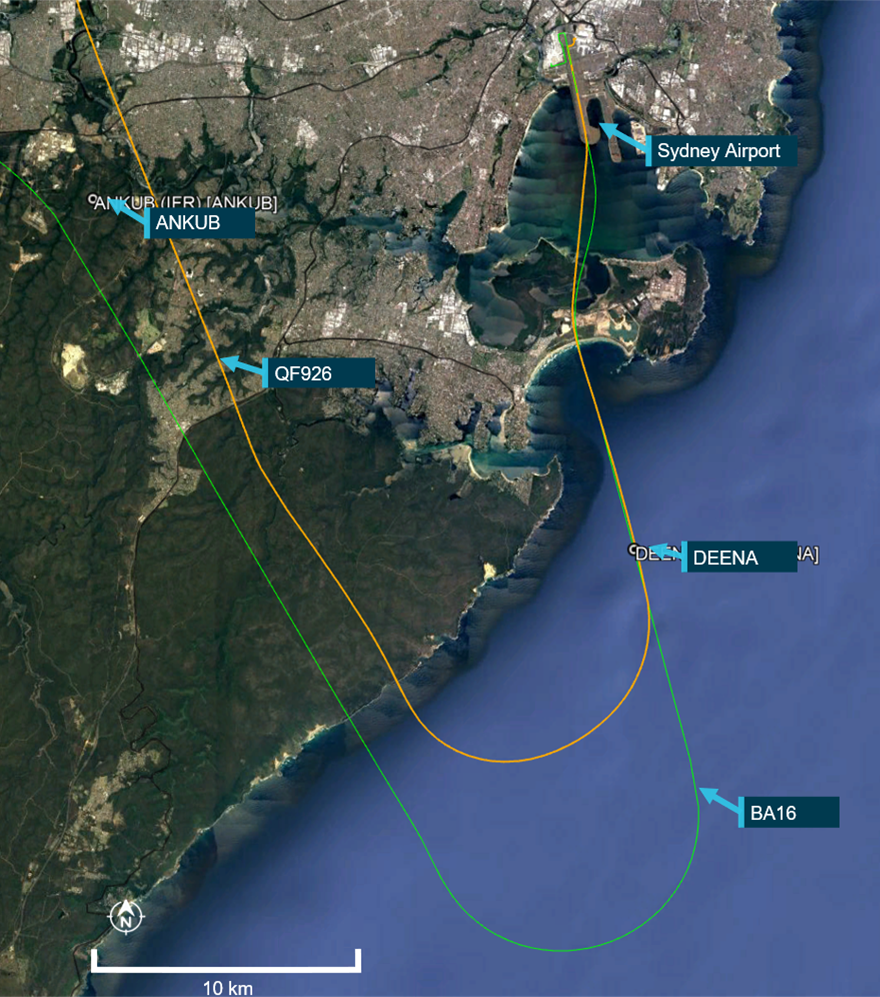
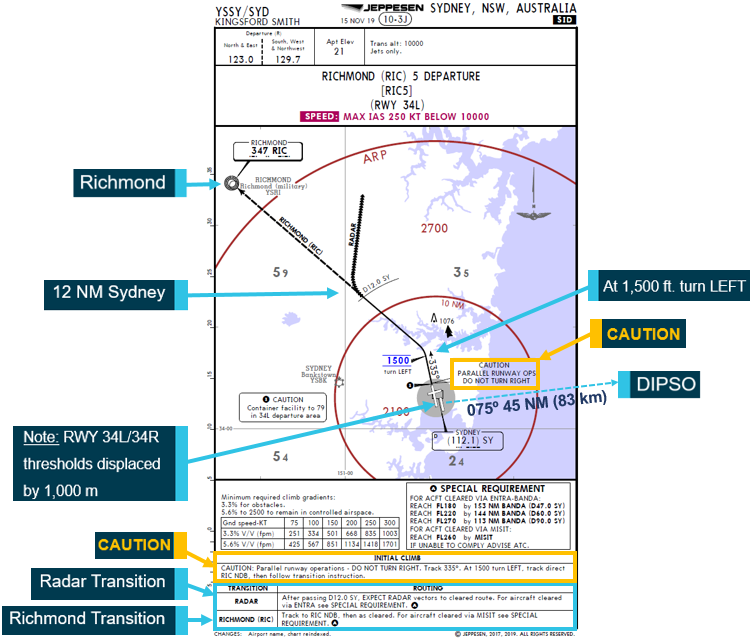
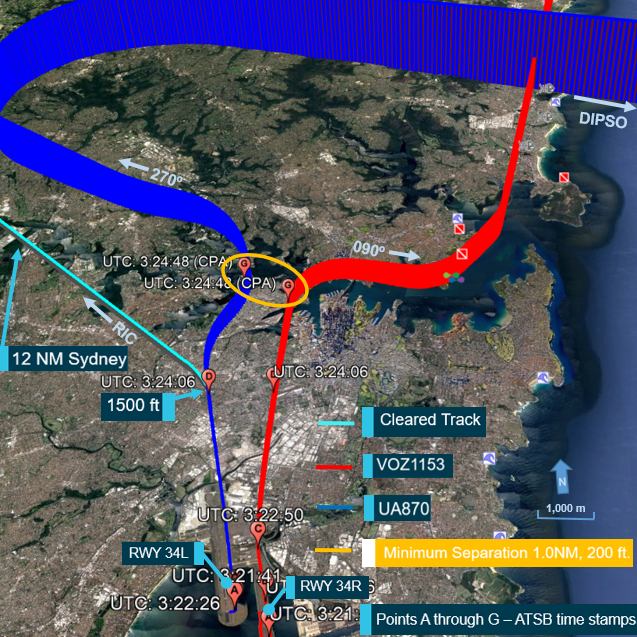
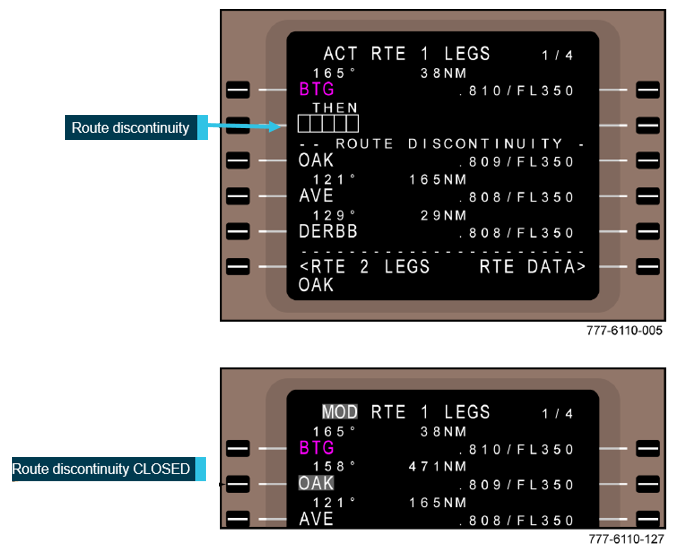

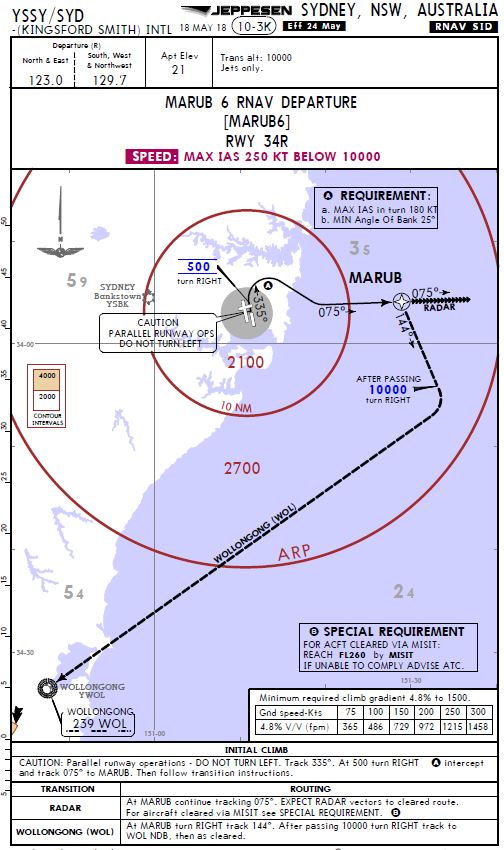
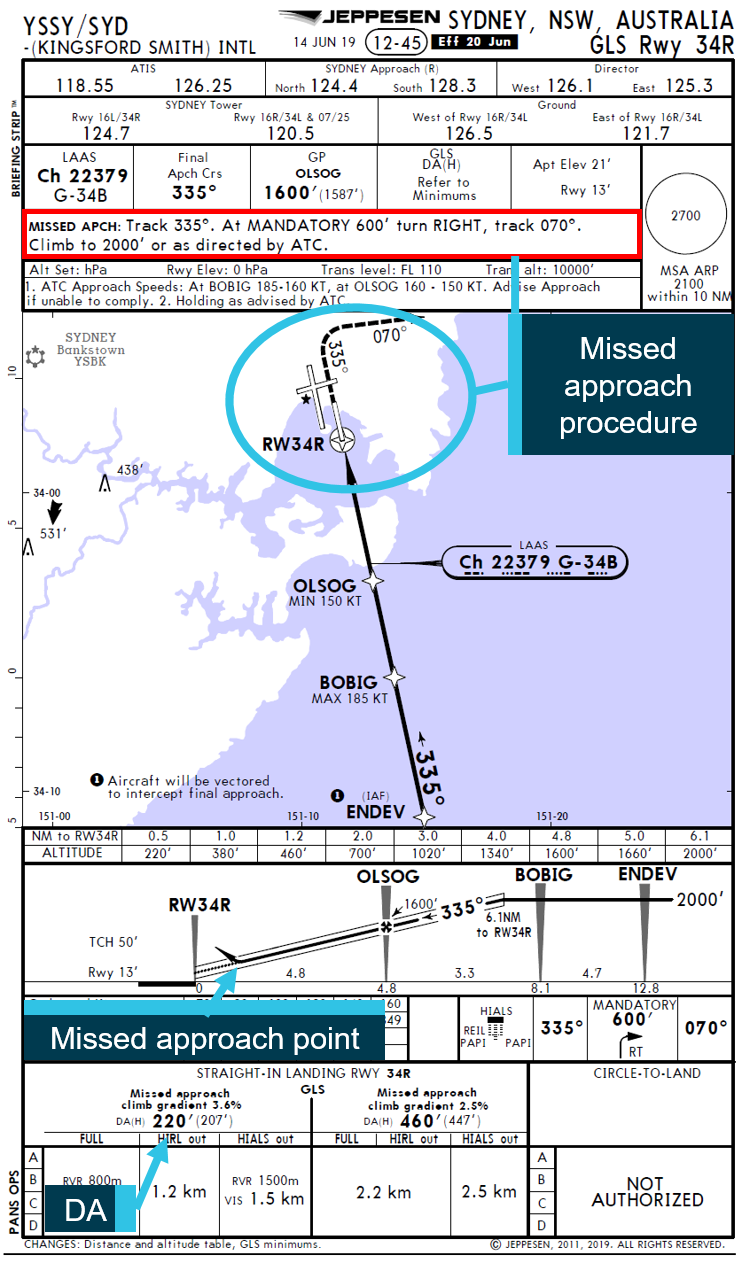

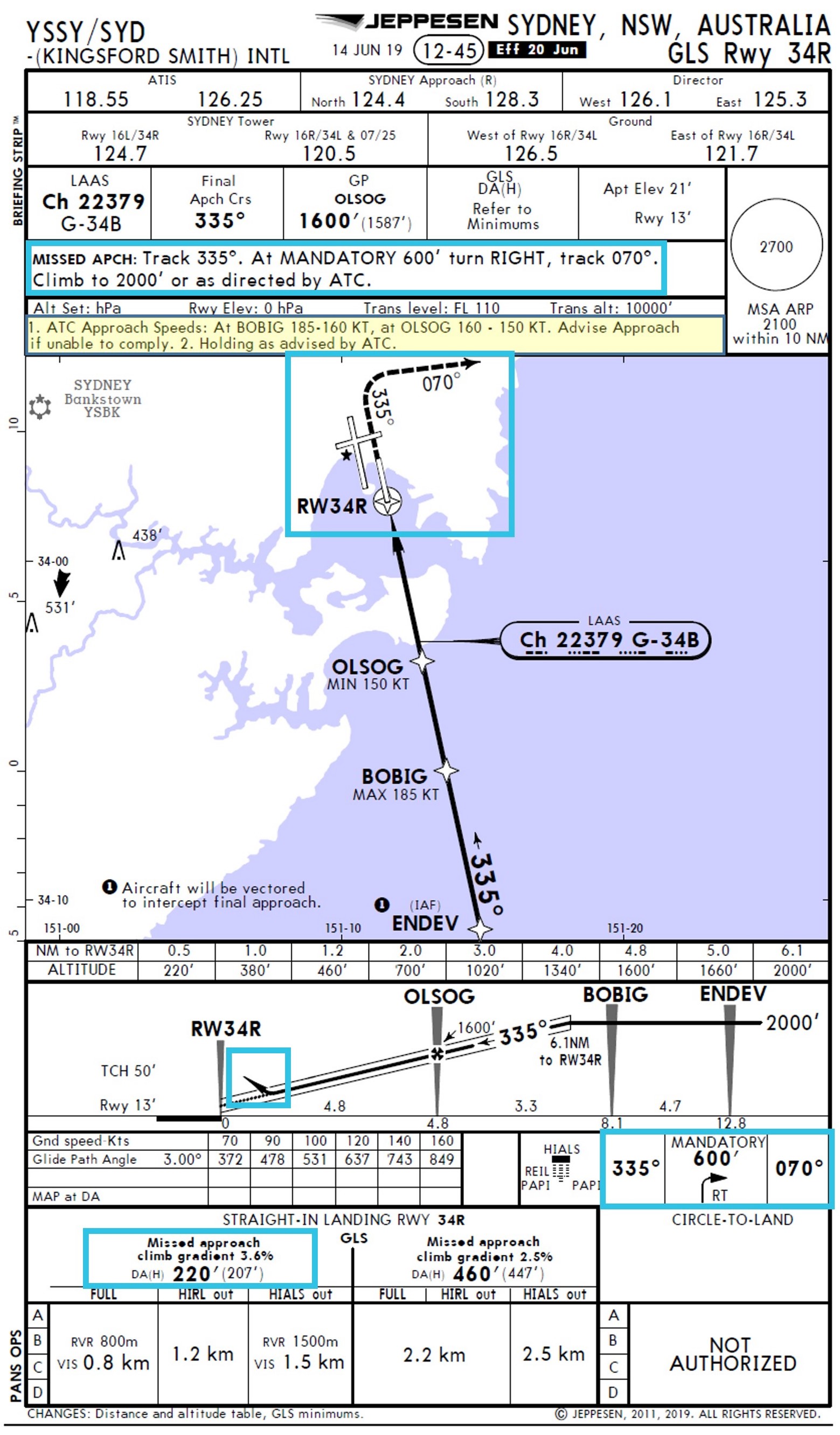
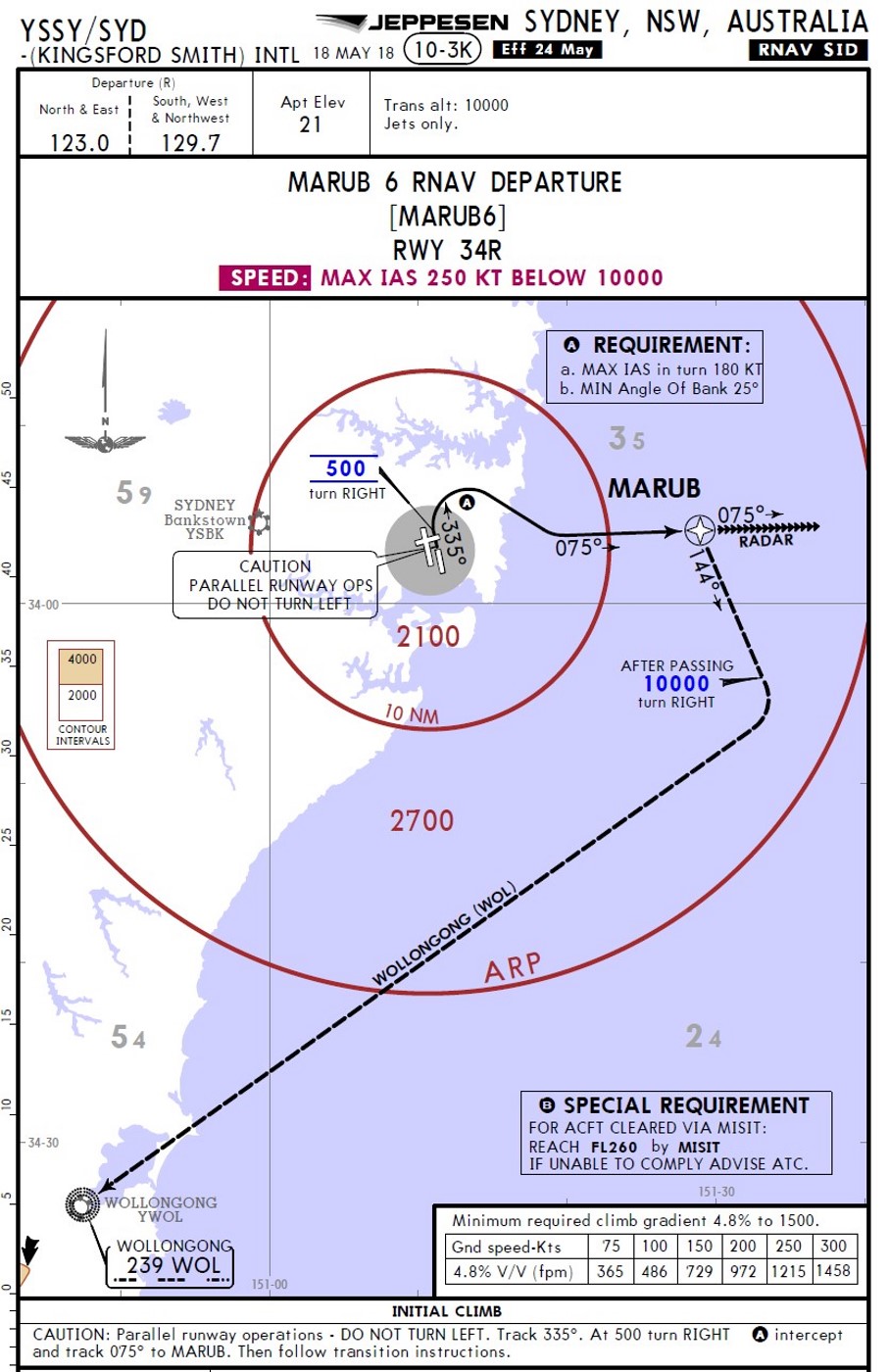

![Figure 5: Representation of an ATC display when the A330 crew was instructed to line up showing location of the A330, Dash 8 and 737 aircraft and an exemplar separation measurement (light yellow).[11]](/sites/default/files/inline-images/AO-2019-041%20Figure%205.jpg)