At 0728 Eastern Standard Time on 31 March 2006, an amateur-built Lancair 320 aircraft, registered VH-BST, departed Townsville, Qld, on a private flight to Archerfield Aerodrome, Qld. The pilot, who owned the aircraft and was the sole occupant, had earlier submitted a visual flight rules (VFR) flight plan for the flight.
At 1048.30, the pilot contacted the Archerfield Aerodrome Controller and reported that he was 19 miles (35 km) from the aerodrome and inbound. He said that he was new to the area and would appreciate any help. The controller advised the pilot to report at the TV towers, a VFR reporting point 13 km north-west of Archerfield. The aircraft was maintaining about 3,700 ft AMSL (above mean sea level).
The pilot reported at the TV towers but had difficulties finding the aerodrome. Radar data showed that the aircraft was 2 km north of the aerodrome at 1,700 ft AMSL, and tracking south-south-east. At 1058.11, the controller asked the pilot if he had the aerodrome in sight. The pilot said that he did not, and said 'I feel I've overflown it'. The controller advised that radar information indicated that the aircraft was north of the aerodrome, and he suggested that the pilot continue to turn left. The pilot then acknowledged that transmission. No further radio transmissions were received from the pilot.
Witnesses reported seeing the aircraft's left wing drop and the aircraft appeared to enter a spin before descending straight down, colliding with a tree and then a creek running parallel to Kessels Road, Coopers Plains. The aircraft was destroyed and the impact was not survivable.
Summary
At 0728 Eastern Standard Time on 31 March 2006, an amateur-built Lancair 320 aircraft, registered VH-BST, departed Townsville, Qld, on a private flight to Archerfield, Qld. At 1058, shortly after flying past the destination airport, the aircraft departed controlled flight and impacted the ground. The aircraft was destroyed and the pilot sustained fatal injuries.
The loss of control was consistent with an accelerated aerodynamic stall, at a height from which it was not possible to recover, followed by the aircraft entering a spin to the left prior to impact. The loss of control occurred when the pilot was operating in adverse weather conditions of low cloud, was tracking towards an area of reduced visibility in rain and towards terrain that was higher than the aircraft.
The pilot's decision to continue the flight into instrument meteorological conditions, even though neither he nor the aircraft were certified to operate is those conditions, increased safety risk. The pilot's ability to fly the aircraft and manage the flight was limited by his relative lack of experience on high performance aircraft, and deficiencies in the training that he had received on the Lancair.
Some aerodynamic and flight control characteristics of the Lancair 320 aircraft increased the risk of an accident. However, those characteristics were largely a consequence of the role for which the aircraft had been designed. In order to operate Lancairs and other high-performance amateur-built experimental aircraft safely, pilots need to be aware of, and maintain the aircraft within, the safe operational envelope.
In response to this and other accidents involving amateur-built experimental aircraft, the ATSB is conducting further research on safety aspects of these types of aircraft.
A turbine-engined PZL-Warszawa-Okecie M-18A Dromader aircraft, registered VH-FVF (callsign Bomber 223), was conducting fire suppression operations on a bushfire in the vicinity of Mount Ulandra, near Bethungra, NSW. At 1921 Eastern Daylight- saving Time, the aircraft was seen by fire fighters to make a low pass over the fire ground area and commence a left turn. Another fireman reported seeing the aircraft in an almost vertical left bank before losing sight of it. None of the other firemen continued to watch the aircraft but, moments later, they reported that they heard a loud noise. When they looked again, the aircraft had hit the ground. The pilot was fatally injured, and the aircraft was destroyed by impact forces. There was no fire.
The crew of a helicopter engaged in fire bucket operations on the same fire ground reported hearing the Dromader pilot broadcast that he was 'lining up for a drop'. A short time later, the helicopter crew reported that they heard the pilot transmit three short expletives. After unsuccessfully attempting to contact the pilot, they commenced searching and located the wreckage of the aircraft a few minutes later, where fire fighters were already in attendance.
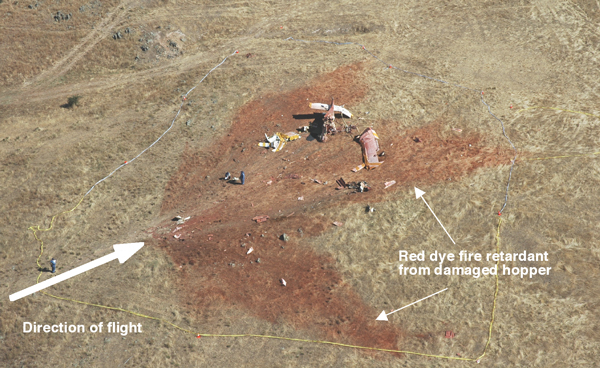
The aircraft had impacted open, rising terrain in a nose-down, slightly right wing-low attitude. Examination of the impact marks and the wreckage indicated that the aircraft had been travelling at low forward speed and with a high rate of descent. The ground around the wreckage was covered with a considerable amount of chemical retardant from the ruptured hopper (Figure 1).
Figure 1: Aerial view of wreckage
The aircraft was manufactured in Poland in 1988 and placed on the Australian register in March 1999. In November 2003, the aircraft was modified from the original design in accordance with an approved Supplemental Type Certificate (STC), number SA09039SC, which permitted the replacement of the original reciprocating (radial) engine and the 4-blade propeller with a Garrett TPE 331-12U gas turbine engine and a Hartzell 5-blade constant speed propeller. The modification also incorporated other changes that included the replacement of the hopper with a larger, 800 US gallon (3,030 L) hopper. Additionally, servo tabs were added to the primary flight control surfaces, flap travel was increased and vortex generators were installed on the wings and tailplane.
The aircraft was operated in the restricted category 1 that permitted flight at weights up to 5,300 kg during agricultural operations, which was 1,100 kg in excess of the certified maximum aircraft weight. Flights at those weights restricted the aircraft's maximum speed and, during fire suppression operations, manoeuvring was limited to a maximum angle of bank of 30 degrees.
The pilot held a commercial pilot licence, endorsed for the aircraft type, and a valid Class 1 medical certificate. The pilot also held a Grade 1 Agricultural Rating and had been issued a Night Visual Flight Rules Agricultural Rating on 19 December 2004. The test for that rating met the requirements of the Aeroplane Flight Review, the biennial proficiency check required of pilots. The pilot had in excess of 4,000 hours in agricultural flying operations, of which 127 hours were flown in fire suppression operations over a period of six seasons. Although the pilot had only 4.7 hours on the aircraft type, he had flown over 400 hours on the unmodified radial-engine Dromader aircraft type, and had over 600 hours on other turbine-powered aircraft. The pilot had commenced fire bombing operations two days before and was reported to have been well rested and in good health.
The investigation is continuing and will include the following aspects:
analysis of data downloaded from the aircraft's Global Positioning System navigation receiver to determine the actual flight path
testing of the switches controlling the hopper gate
examination of other aircraft components
a review of maintenance documentation and records of modification made to the aircraft
an appraisal of flight characteristics of the modified aircraft during operations at higher gross weights.
Restricted category aircraft are certified by the Civil Aviation Safety Authority to conduct certain special purpose operations.
Summary
At about 1922 Eastern Daylight-Saving Time on 16 February 2006, the pilot of a turbine PZL-Warszawa-Ockie M-18A, Dromader, registered VH-FVF, was fatally injured when the aircraft impacted terrain during fire-bombing operations approximately 20 km south-south-west of Cootamundra, NSW.
The pilot was an experienced agricultural pilot with previous fire-bombing experience. Although he had considerable flying experience on radial-engine Dromader aircraft, and in other turbine agricultural aircraft, his total flying experience in the modified turbine Dromader was 4.7 hours. Prior to commencing fire-bombing duties two days before the accident, the pilot had not recorded any fire-bombing flights in the previous 3 years.
The pilot's limited familiarity with the handling characteristics of the modified and heavily loaded aircraft might not have allowed him adequate recognition of an impending stall. The pilot had not jettisoned the load of retardant when the aircraft stalled. The ensuing loss of control occurred at a height that did not permit recovery before the aircraft collided with the ground. The possibility that the pilot was distracted by a problem with the operation of the fire doors, or some other activity could not be determined.
Subsequently, the state fire authority reviewed its minimum pilot experience levels for aerial fire suppression. The minimum aircraft type experience for fire-bombing pilots was made more specific to the type of aircraft. It also introduced a recency requirement for fire-bombing operations.
During a charter flight from Broome, WA to Cone Bay, WA, the pilot of an amphibious (float and landing gear equipped) Viking Air Ltd DHC-3-T 'Turbo-Otter' aircraft (VH-OTV) reported an unusual movement within the control system, followed by a sudden downward pitching motion, leading to a rapid and uncontrolled descent. With the assistance of the front seat passenger, the pilot was able to arrest the descent and regain control of the aircraft, before making a precautionary landing at Lombadina Station, WA.
An engineering assessment of the aircraft found that the right elevator servo tab had broken away from the control rod and horn at the outboard end. Damage to the elevator trailing edge and tearing of the tab through the mid-span was consistent with gross oscillatory movement (flutter) of the tab after it had become disconnected from the rod and horn.
Aerodynamic flutter within the elevator trim and servo tabs of the DHC-3 aircraft type had been known since the 1960s, however the development of turboprop engine conversions for the aircraft had resulted in an increased potential for tab failure as a result of the increased airspeeds and control surface loads associated with the re-engined aircraft. A series of engineering solutions to the flutter problem had been subsequently developed, and in April 2004, a US Federal Aviation Administration airworthiness directive (AD) mandated the modification of the DHC-3 elevator tab assembly for US registered aircraft.
At the time of the occurrence, VH-OTV had not undergone the elevator tab modifications. The maintenance organisation stated that it was unaware of the FAA actions and had not received any information as to the availability of flutter prevention modifications from the aircraft type certificate holder or the certificate of registration holder.
Safety action taken by the maintenance provider after the occurrence included the implementation of systems to more adequately alert the organisation to the existence of important safety bulletins and airworthiness directives affecting the aircraft. An airworthiness directive for the elevator tab modifications issued by Transport Canada the month before the occurrence, became effective on 31 March 2006 and, on 1 March 2006, the Civil Aviation Safety Authority (CASA) introduced an AD to mandate the prospective Transport Canada requirements from 31 May 2006.
Occurrence summary
Investigation number
200600837
Occurrence date
15/02/2006
Location
Lombadina, (ALA)
State
Western Australia
Report release date
25/01/2008
Report status
Final
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Loss of control
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
De Havilland Canada/De Havilland Aircraft of Canada
On 12 February 2006, the pilot of a Robinson Helicopter Company R44 Raven II Newscopter, registered VH-WYS, was conducting aerial filming of a banner towing helicopter in the vicinity of Williamstown, Vic. On board with the pilot were a photographer in the front left seat and a gyro-stabilised camera operator in the rear left seat.
While in a turn at low airspeed, and with a quartering tailwind, the helicopter began an uncommanded yaw to the right. The pilot attempted to regain control, but the helicopter continued to rotate to the right and descended approximately 1,800 ft before control was regained. The helicopter was flown to a nearby beach and landed.
The reported ambient conditions and nature of the loss of control were consistent with the pilot report that the helicopter had suffered a loss of tail rotor effectiveness (LTE). It was possible that the onset of vortex ring state had contributed to the high rate of descent during the pilot's recovery from the LTE.
On 19 December 2005, the helicopter manufacturer advised the Australian Transport Safety Bureau (ATSB) that the procedure for setting the autorotation rotor RPM contained in the Kawasaki Heavy Industries BK 117 B-2 (BK 117 B-2) maintenance manual did not cover operation of the helicopter at high gross weight. In order to correct that procedure, the manufacturer advised the operator to re-set the helicopter's collective pitch setting in accordance with the relevant procedure in the BK 117 C-18 model helicopter's maintenance manual, which can be used to set the helicopter's autorotation rotor RPM at high gross weight.
On 20 December 2005, the helicopter manufacturer advised the ATSB that it intended amending the BK 117 B-2 maintenance manual to reflect the procedures detailed in the BK 117 C-1 manual, and that it would advise all customers who operated the BK 117 B-2 helicopter of the change to the maintenance manual. A temporary revision to the manual was subsequently issued by the manufacturer. On 20 January 2006, the maintenance manual was amended to include the procedure for setting autorotation rotor RPM in the BK 117 B-2 at high gross weight.
Australian Transport Safety Bureau
The ATSB provided an initial alert to the Civil Aviation Safety Authority (CASA) of this safety deficiency on 15 December 2005. Further information on the progress of the ATSB investigation was provided to CASA technical staff on 19 December, with notice of the likelihood of the ATSB issuing a safety recommendation provided later that day. On 21 December 2005, CASA technical staff met with ATSB investigators and, following a briefing, advised the ATSB that CASA would alert operators about this safety deficiency.
On 22 December 2005, the ATSB issued the following safety recommendation R20050014 to CASA. That recommendation stated:
The Australian Transport Safety Bureau recommends that the Civil Aviation Safety Authority alert Australian operators of the Kawasaki BK 117 B-2 helicopter to the discrepancy with respect to the procedure for adjusting the collective pitch settings in the maintenance manual.
On 22 December 2005, CASA wrote to all Australian owners and operators of the BK 117 B-2 helicopter and recommended that, pending advice from the helicopter manufacturer, operators of the BK 117 B-2 should:
reduce exposure to conditions of high-density altitude and atmospheric turbulence, especially if the aircraft is at high gross weight
if such conditions were encountered, reduce airspeed and torque settings while hand flying the aircraft with SAS [Stability Augmentation System] mode engaged.
On 7 February 2006, CASA advised the ATSB that the helicopter manufacturer had provided all Australian operators of the BK 117 B-2 helicopter with the amended procedure for setting the collective pitch setting. In response to the safety action undertaken by CASA and the helicopter manufacturer, the ATSB has classified safety recommendation R20050014 as 'Closed-accepted'.
8. The BK117 B-2 helicopter type certificate also included the BK 117 C-1 model helicopter.
Analysis
The abnormally high collective pitch setting meant that the majority of the helicopter's forward cyclic control authority was required by the pilot to maintain level flight. The result was that, in response to the nose-up pitch, there was insufficient remaining forward cyclic control available for the pilot to recover the helicopter without also lowering the collective control. It appeared likely that the reported severe turbulence contributed to the helicopter's initial nose-up pitch.
Factual Information
At about 1315 hours Eastern Daylight-saving Time on 7 December 2005, a Kawasaki Heavy Industries BK 117 B-2 (BK 117 B-2) helicopter, registered VH-IME, was being operated on a medical flight at 7,000 ft above mean sea level, in moderate to severe turbulence and in visual meteorological conditions (VMC), when the helicopter sustained an uncommanded nose-up pitch of 40° to 45°. The pilot attempted to counter the nose-up pitch by applying full forward cyclic control, but without effect. The pilot then lowered the collective control, producing a nose-down pitching moment, before recovery to normal level flight could be achieved. The Mast Moment advisory light illuminate 1 and the pilot continued the flight to the destination at reduced airspeed.
The pilot reported that, immediately prior to the nose-up pitch, the helicopter's indicated airspeed was about 120 kts, and the outside air temperature was 20° C. He indicated that the torque 2 setting was about 68 % and within the helicopter's published limits at that time, and that he felt the position of the cyclic control may have been further forward than normal.
The helicopter's estimated all up weight (AUW) was 3,200 kg and its Velocity Never Exceed 3 was estimated to be 125.5 kts. The Eurocopter Deutschland GmbH 4 (ECD) Flight Safety Department advised that that speed should have only been possible in the BK 117 B-2 helicopter when in a descent.
The pilot reported that he flew through severe turbulence just prior to the incident, but that he felt no abnormal vibrations prior to the nose-up pitch. He also stated that, during an after-flight crew de-brief, one crew member reported that the helicopter rolled right after the nose-up pitch. The pilot could not recall that roll.
The incident was subsequently investigated by an ECD test pilot and engineer, in consultation with representatives of the helicopter's Japanese manufacturer. That investigation revealed that the published procedure for setting autorotation rotor RPM in the BK 117 B-2 maintenance manual did not include for aircraft operations at high gross weight, and that the application of that procedure in the incident helicopter had resulted in an inappropriately high collective pitch setting.
The effect of the helicopter's collective pitch stop is to limit the collective travel and, in turn, establish a maximum horizontal speed (VH 5) for the ambient conditions and AUW of the helicopter. The ECD Flight Safety Department advised that the helicopter's abnormally high collective pitch setting meant that the pilot would require increased forward displacement of the cyclic control in order to maintain level flight. That would result in a reduction in the longitudinal cyclic control authority 6 that was available to the pilot.
The ECD Flight Safety Department indicated that the severe turbulence reported by the pilot could have precipitated the helicopter's nose-up pitch in this incident, and that the reduced longitudinal cyclic control authority would have restricted the pilot's ability to recover the changing pitch. Retreating blade stall 7 was considered by the ECD Flight Safety Department as an unlikely contributory factor in this instance, as it was only considered possible when the helicopter was in a descent profile.
The illumination of the Mast Moment advisory light indicated that the rotor mast had exceeded its normal limits.
A measure of the power provided by the helicopter's engines to overcome the resistance of the rotor blades to rotation, and maintain constant main rotor RPM.
Never-exceed speed that was specified by the helicopter's manufacturer.
Co-designed with Kawasaki Heavy Industries. The incident helicopter was manufactured by Kawasaki Heavy Industries.
The maximum possible sustained airspeed in level flight at the helicopter's continuous engine power rating.
The forward and aft limits of travel of the cyclic control.
Stall of the retreating blades at high helicopter forward speeds. Occurs when the angle of the attack of the retreating blades becomes excessive, especially towards the tip of the retreating blades.
Summary
At about 1315 hours Eastern Daylight-saving Time on 7 December 2005, a Kawasaki Heavy Industries BK 117 B-2 (BK 117 B-2) helicopter, registered VH-IME, was being operated on a medical flight at 7,000 ft above mean sea level, in moderate to severe turbulence and in visual meteorological conditions (VMC), when the helicopter sustained an uncommanded nose-up pitch of 40° to 45°. The pilot attempted to counter the nose-up pitch by applying full forward cyclic control, but without effect. The pilot then lowered the collective control, producing a nose-down pitching moment, before recovery to normal level flight could be achieved. The Mast Moment advisory light illuminated, and the pilot continued the flight to the destination at reduced airspeed.
An investigation by the co-designers and manufacturer of the helicopter identified an incorrect collective pitch setting that reduced the longitudinal cyclic control authority available to the pilot. That reduced authority restricted the pilot's ability to recover the nose-up pitch.
A number of safety actions resulted from this investigation, including:
advice to the operator from the helicopter's manufacturer to re-set the helicopter's collective pitch setting in accordance with the BK 117 C-1 model helicopter maintenance manual
amendment of the BK 117 B-2 maintenance manual to include the relevant collective pitch setting procedure from the BK 117 C-1 manual
the issue of Safety Recommendation R20050014, which recommended that the Civil Aviation Safety Authority (CASA) should alert Australian operators of the collective pitch setting discrepancy in BK 117 B-2 helicopters
an interim alert was provided to Australian operators of the BK 117 B-2 helicopter by CASA to amend their operation of the BK 117 B-2 pending advice from the helicopter's manufacturer
On 27 October 2005, a McDonnell Douglas Hughes 369E 1 helicopter, registered VH-SUV, sustained a loss of tail rotor control and started spinning, while being operated on a power line inspection near Warwick, Qld. The pilot attempted to control the spin, but the helicopter was reported to have made approximately 12 to 15 full rotations before landing in a paddock. The pilot and two observers on board received minor injuries. The helicopter sustained minor damage.
Helicopter
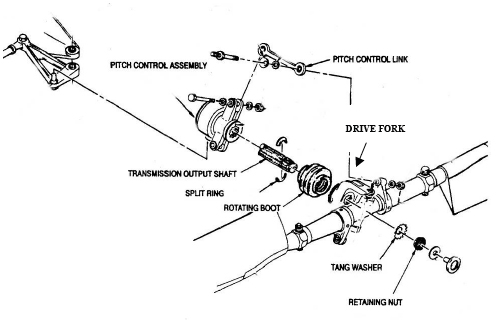
The helicopter was manufactured in 1990 and at the time of the occurrence had accumulated 3,543.8 hours total time in service (TTIS) and 4,348 landings since new. The helicopter was purchased overseas in a damaged condition after accumulating 3,118.35 hours TTIS since new. It was purchased and rebuilt by the operator and in February 2005 received a Civil Aviation Safety Authority (CASA) Certificate of Airworthiness. Maintenance records indicated that the helicopter had been fitted with a serviceable pitch control assembly during the rebuild (Figure 1).
Figure 1: Tail rotor pitch control assembly
Since the rebuild and its return to service, the helicopter had been maintained in accordance with the maintenance requirements applicable at that time and had a valid Maintenance Release. It had flown approximately 82.2 hours since the last periodic inspection in September 2005.
Tail rotor examination
The operator examined the tail rotor. That examination found that the loss of tail rotor control was due to the failure of the inner tab of the tang washer (Figure 2). The washer locked the retaining nut holding the drive fork and the tail rotor assemblies onto the transmission output shaft. The failure of the inner tab resulted in looseness of the retaining nut that allowed the split ring to be dislodged. Consequently, the drive fork and the tail rotor assemblies were able to move freely along the transmission output shaft. That resulted in the loss of tail rotor control and the blades adopting a neutral pitch.
Figure 2: New tang washer with an undamaged locking tab and the subject tang washer with broken locking tab
Tang washer
The operator reported that a new tang washer was fitted at the time of the helicopter rebuild and that a torque strip was applied across the retaining nut, tang washer and drive fork as required by the helicopter maintenance manual. The maintenance manual requires the torque strip to be applied in a location where it could be checked visually.
The operator sent the failed tang washer to the helicopter manufacture to determine the nature of the locking tab failure. At the time of issue of this report the operator had not received a response from the helicopter manufacturer.
Previous tail rotor control problems
A search of the ATSB database, for the 1995 to 2005 period, revealed no records of similar tail rotor control problems. The CASA Service Difficulty Report database, for the same period, contained only the record of the tail rotor control problem from this occurrence.
The manufacturer advised that they have received two worldwide reports of a broken locking tab since 1988.
The helicopter was fitted with the two bladed tail rotor assembly.
Summary
The helicopter sustained a loss of tail rotor control while carrying out a power line inspection. It made approximately 12 to 15 full rotations before landing in a paddock. The pilot and two observers on board received minor injuries. The helicopter sustained minor damage.
Examination of the tail rotor revealed that the loss of control was due to failure of the inner tab of a tang washer. The washer locked the retaining nut holding the drive fork and the tail rotor assemblies onto the transmission output shaft. The failure of the inner tab resulted in looseness of the retaining nut and the split ring becoming dislodged. Consequently, the drive fork and the tail rotor assemblies were allowed to move freely along the transmission output shaft.
The ATSB was advised that at the helicopter rebuild a new tang washer was fitted. To inspect the washer, the retaining nut would have to be removed.
The operator sent the failed tang washer to the helicopter manufacturer to determine nature of the locking tab failure. The report had not been received at the time of writing this report.
A search of the ATSB database, for the 1995 to 2005 period, revealed no records of similar tail rotor control problems. The Civil Aviation Safety Authority Service Difficulty Report database, for the same period, contained only the record of the tail rotor control problem from this occurrence.
The manufacturer advised that they have received two worldwide reports of a broken locking tab since 1988.
The investigation identified that the following factors contributed to the accident:
The aircraft descended below the minimum altitude for a practice forced landing (500 ft above ground level).
The pilot allowed the aircraft's speed to decrease below the aircraft's stalling speed.
The aircraft stalled at a height above the ground that was not adequate to permit recovery.
It is possible that carburettor ice was present during the latter stages of the flight, reducing the available engine power.
Analysis
ANALYSIS
The final minutes of the recorded Air Traffic Services radar data indicated that the pilot performed a series of turns in a constant descent that was consistent with a forced landing. Given the pilot's history of performing many practice forced landings, it is likely that immediately prior to the accident, the pilot was conducting a practice forced landing.
When radar contact was lost, the aircraft was already below the minimum altitude for a practiced forced landing and there was no indication that the pilot had decreased the rate of descent. That was confirmed by witnesses that indicated that the aircraft was well below 500 ft above ground level.
Based on the pilot's training records and interviews with flight instructors, it is probable that the pilot was fixated on the chosen landing area and descended below the minimum height for a go-around. During the latter stages of the approach recorded by the radar, the pilot performed a tight 360º turn. That may have been intentional to allow the aircraft to lose height and still be positioned for the selected landing area. During the turn, the aircraft lost approximately 25 kts, which reduced the margin above the aircraft's stall speed.
A person near the accident site reported seeing the aircraft at a very low altitude and flying quietly before hearing power applied. However, the atmospheric conditions around the time of the accident were conducive to the formation of serious carburettor ice at descent power and the engine may not have been capable of producing full power when it was applied. Because the person's attention returned to their duties, it was not known if the application of power that they reported was sustained for any length of time. The evidence in the wreckage indicated that there was little or no power applied at impact. The pilot may have removed power as part of the stall recovery procedure. The use of carburettor heat could not be determined and the formation of carburettor ice was a possibility.
The attitude at which the aircraft impacted the ground and the damage to the tail section indicated that the aircraft had stalled before it impacted the ground. The combination of the loss of airspeed during the turn and the pilot's documented difficulty with stall recognition and response, may have led to an inadvertent stall, either during the go-around or in the subsequent climb out. The height at which the aircraft stalled was not sufficient to permit a recovery. It was not possible to determine if carburettor icing had reduced the power available for the go-around and aggravated the situation.
Fatigue
Based on the pilot's activities and sleep patterns prior to the occurrence, it was apparent that the pilot probably obtained only 5 to 6 hours of interrupted sleep on the night before the accident. Even though this was consistent with his normal sleeping patterns, in all likelihood, the pilot may have started the day with a degree of fatigue as a result of insufficient quantity and quality of sleep the previous night. The pilot may have also been experiencing the effects of chronic fatigue given his recurring pattern of interrupted and relatively low quantity of sleep. Consequently, fatigue may have reduced the pilot's ability to fly the aircraft accurately and to develop and maintain awareness of, and make timely decisions in response to, a degraded aircraft state, such as a stall.
Pilot's training history
The pilot had required a significant amount of flying training to meet the General Flying Progress Test standard. The pilot's training was regular, but spread over a considerable period of time. The training records indicated that the pilot had difficulty in acquiring, maintaining and consolidating the skills required to safely operate a light aircraft. Many lessons were repeated to bring the pilot up to the required competency standard. Of particular note is that the pilot consistently demonstrated poor airspeed control during practice forced landings, indecision, a poor awareness of an impending stall, a lack of response to the stall warning horn, and incorrect stall recovery technique. These factors are consistent with the circumstances surrounding the accident.
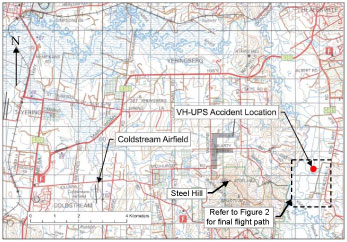
At about 0945 Eastern Standard Time2 on Saturday 23 April 2005, a Cessna Aircraft Company A150L Aerobat aircraft, registered VH-UPS, departed Coldstream Airfield, Vic. for a private flight in the Coldstream General Flying Training Area, with the pilot as the only occupant (Figure 1).
The aircraft was first tracked by the Air Traffic Services (ATS) radar at 0949 heading in a northerly direction consistent with a departure from Coldstream runway 35. Over the next 6 to 7 minutes, the aircraft made a series of right turns that brought the aircraft into an area to the southeast of Steel Hill. The radar track shows the aircraft performing some aerial manoeuvres in this area before heading north-northeast towards Healesville for several minutes, then turning left for another series of aerial manoeuvres.
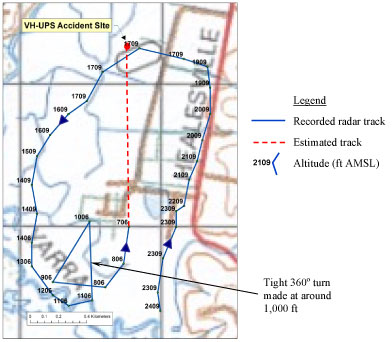
The final minutes of recorded radar data (Figure 2) show that the aircraft performed a descending orbit into the Yarra Valley before losing radar contact. The aircraft did not reappear on radar. At about that time, a passenger in a vehicle travelling along the Healesville - Koo Wee Rup Road observed the aircraft flying at low level. Shortly after, the aircraft was seen in a steep dive before it disappeared behind an embankment. The occupants of the vehicle located the wreckage of the aircraft in an open field about 1 km west of the Healesville - Koo Wee Rup Road. The aircraft was destroyed by impact forces and the pilot was fatally injured. There was no fire.
Figure1 : Accident location
Figure 2 : Recorded radar track
Recorded radar data showed that the aircraft maintained a fairly constant rate of descent of about 660 ft/min from an altitude of about 2,400 ft Above Mean Sea Level (AMSL), down to about 700 ft AMSL. That placed the aircraft at about 430 ft above ground level (AGL) when radar contact was lost. There was no indication in the radar data that the aircraft had ceased its descent when contact was lost. The accident site was located about 0.7 NM to the north of the last radar return.
At about 1,000 feet AMSL and heading in a north-easterly direction, the aircraft performed a tight 360º turn3 whilst maintaining the descent. During this turn, the radar recorded a decrease in speed of about 25 kts.
An employee working on the property where the accident occurred observed the aircraft pass at a very low level (estimated between 100 and 200 ft AGL) and flying quietly. The aircraft passed within several hundred metres of the employee and was headed in a northerly direction. The employee reported hearing the engine sound increase before returning their attention to their duties. Having worked on the property for some years, and observed many aircraft training in the area, the employee did not notice anything unusual about the aircraft, other than it being very low. Although located only 900 m from the accident site, the employee did not observe the final moments of the flight or the collision with the ground.
Wreckage information
Ground marks and crushing of the left-wing tip indicated that the aircraft had impacted the ground in a left wing-low and approximately 30º nose-down attitude. The direction of flight was approximately 320º (magnetic). The wing flaps were found in the fully retracted position.
The aircraft came to rest about 10 m from the impact point (Figure 3). The fuselage lay on its roof with the left wing wrapped over the cabin and the right wing in a near vertical position. The rear fuselage was bent downward and to the left. The tailplane had separated from the fuselage and the fin, which was lying on the right tailplane, had broken away from its mounting brackets. There were no indications of any pre-existing defects in the aircraft structure.
Figure 3 : Aircraft wreckage
Examination of the propeller, throttle lever position and engine instruments indicated that the engine was operating at low RPM and developing little or no significant engine power at impact. Examination of the engine found no evidence of a mechanical or system failure that would have prevented the production of power prior to impact. Due to the impact damage, the status of the carburettor heat control at impact could not be reliably determined.
Examination of the stall warning system, airspeed indicator and altimeter indicated that they were capable of normal operation during the flight prior to impact.
Personnel information
The pilot's flying experience was estimated as:
Experience Type
Flying time (hours)
Total time
180.9
Dual time
132.7
Command time
48.2
On type (Cessna 150)
152.9
Hours flown in the last 24 hours
0.7
Hours flown in the last 7 days
1.3
Hours flown in the last 90 days
12.8
The pilot commenced part-time flying training on 23 May 2003 and was issued a Student Pilot Licence on 15 November 2003. The pilot's first solo flight on 23 November 2003 was made after receiving 43.7 hours of dual training. A pre-licence check flight was conducted by a senior instructor on 6 January 2004 when the pilot had 77.3 hours of experience. However, it was not until 24 July 2004 that the pilot achieved the General Flying Progress Test (GFPT) after a further 51 hours of flying training. At that time, the pilot had accumulated a total flying time of 128.4 hours, of which 104.9 hours were dual instruction. All of the pilot's flying training was undertaken at the same organisation.
The flying training organisation's pre-GFPT syllabus indicated that the minimum flying training required to the end of the GFPT phase was 23 hours dual and 6 hours solo, a total of 29 hours. The regulatory minimum total flight time required before attempting the GFPT was 20 hours of flight time.
After completing the GFPT, the pilot commenced cross-country navigation training as part of the Private Pilot (Aeroplane) Licence training syllabus. He had also completed 9.7 hours of aerobatic flight training but had not received an aerobatics endorsement. Entries in the pilot's logbook suggested that the pilot had previously engaged in solo aerobatics with a passenger on board the aircraft.
The pilot held a current Class 2 medical certificate that was endorsed with the restriction 'Renew by CASA only'. The results of the post-mortem examination and toxicology screening found no evidence of any physiological factor that may have impaired the pilot's performance during the accident flight.
In the days leading up to the accident flight, the pilot averaged 5 to 6 hours of sleep per night. These sleep periods were interrupted by waking periods late at night and was reported as the pilot's typical sleep pattern.
A review of the pilot's training records indicated that many lessons were repeated before the minimum competency standards were met. The pilot had recurring difficulties in airspeed management, steep and tight turns, identification of impending stall, response to the stall warning horn, recovery from the stall and go-around decision and technique. The pilot's instructors noted that constant reminders to monitor airspeed and altitude and to perform the appropriate recovery technique were required. The training records included several entries relating to inattention, tunnel vision and trouble attending to all parameters. Annotations of these difficulties were associated with many aspects of the pilot's training, but were particularly apparent for practiced forced landings.
The pilot had recorded a large number of practice forced landings during training, the majority of which were with an instructor.
Practice forced landing
The practice forced landing manoeuvre, as used in the flying training organisation's syllabus, typically involved simulating an engine failure by closing the throttle and gliding the aircraft toward a selected landing area.
The main objective of the manoeuvre was to develop judgement and skill in positioning the aircraft for a gliding approach to the selected field. When the manoeuvre is practiced on to an airfield, a landing is made off the approach. However, when the manoeuvre is practiced in the training area, the student is required to demonstrate a go-around from a safe height, usually not below 500 ft AGL. The go-around manoeuvre requires the pilot to apply full power and select the carburettor heat off, raise the flaps (if used) and establish the normal climb. If, for any reason, engine power is not available, the aircraft is ideally positioned for an emergency landing into the selected field.
To prevent the formation of carburettor ice during the practice forced landing, full carburettor heat is applied. A short application of engine power is normally made every 1,000 ft of descent to maintain engine temperatures. If carburettor heat is not selected off during the go-around, full power will not be available. When the normal climb attitude is maintained with less than full power, the aircraft will climb at a slower airspeed and rate of climb.
The Cessna A150L aircraft was a two-place, high-wing, light aircraft designed for general flying training, but was also capable of aerobatic flight. The aircraft was powered by a Teledyne-Continental Motors O-200-A normally-aspirated piston engine through a fixed-pitch two-bladed propeller.
VH-UPS was imported into Australia in 1990 and had been operated and maintained by the same flying club since that time. It was utilised for both initial flying training and aerobatic training.
The flying club maintained the aircraft in accordance with a CASA approved maintenance system. The last periodic maintenance inspection was carried out on 23 March 2005. The aircraft's maintenance release, recovered from the wreckage, did not list any defects, and the documentation indicated that all required maintenance was completed. The maintenance release was endorsed by a licensed pilot certifying that the daily inspection had been satisfactorily completed on the morning of the accident. The accident flight was the first flight of the day for the aircraft.
Prior to importation into Australia, the aircraft had been fitted with a carburettor ice detection system in accordance with a United States Federal Aviation Administration approved kit. The system consisted of an optical sensor in the carburettor, a control box and a warning light mounted on the instrument panel. The operating instructions indicated that the pilot was required to adjust the sensitivity of the system to suit the local conditions prior to operation. The operational status of the system at the time of the accident could not be determined.
The aircraft had sufficient fuel and was within the weight and centre of gravity limitations for the duration of the flight.
Meteorological information
The Bureau of Meteorology automatic weather station for Coldstream recorded the environmental conditions for Saturday 23 April 2005 as:
At 0900
At 1500
Temperature
11.3 ºC
26.4 ºC
Relative Humidity
98%
38%
Wind Speed and Direction
Calm
9 km/h from NNE
Mean Sea Level Pressure
1028.7 hPa
1024.5 hPa
The skies were overcast with high level cloud, there was a degree of haze; however, the horizon in the valley was clearly distinguishable. People in the area reported that winds were very light.
Carburettor icing
On the day of the accident, the atmospheric conditions were conducive to the formation of serious carburettor icing at descent power. Refer to Appendix A for a Flight Safety Australia magazine 5 article on carburettor icing.
Only those investigation areas identified by the headings and subheadings were considered to be relevant to the circumstances of the occurrence.
Eastern Standard Time was Coordinated Universal Time (UTC) + 10 hours.
The large changes in the aircraft position in this region are likely due to limitations in the radar system at low altitude, however the general pattern of a tight turn is indicated by the data points at 1106, 1006, 906 and 806 ft.
Total time in service.
Flight Safety Australia magazine is a publication of the Australian Civil Aviation Safety Authority.
Summary
At about 0945 Eastern Standard Time on Saturday 23 April 2005, a Cessna Aircraft Company A150L Aerobat aircraft, registered VH-UPS, departed Coldstream Airfield, Vic, for a private flight in the Coldstream General Flying Training Area, with the pilot as the only occupant.
The aircraft was tracked by the Air Traffic Services radar after its departure from Coldstream Airfield. The radar track showed that the aircraft performed some aerial manoeuvres to the east of the airfield before a descending orbit into the Yarra Valley when radar contact was lost. At about that time a passenger in a vehicle travelling along the Healesville - Koo Wee Rup Road observed the aircraft flying at low level. Shortly after, the aircraft was seen in a steep dive before they lost sight of it. The occupants of the vehicle located the wreckage of the aircraft in an open field about 1 km west of the Healesville - Koo Wee Rup Road. The aircraft was destroyed by impact forces and the pilot was fatally injured.
The aircraft had impacted the ground in a left wing-low and nose-down attitude. The fuselage lay on its roof with the left wing wrapped over the cabin and the right wing in a near vertical position. The rear fuselage was bent downward and to the left. The tailplane had separated from the fuselage and the fin had broken away from its mounting brackets. There were no indications of a pre-existing defect in the structure.
The investigation found that it was likely that the pilot was performing a practice forced landing and had descended below the safe altitude when the accident occurred. The airspeed was reduced to a point that the aircraft stalled and the altitude was not sufficient to affect a recovery before impact with the ground. It is possible that carburettor ice was present during the descent.
On 26 May 2005, the Civil Aviation Safety Authority advised the Australian Transport Safety Bureau (ATSB) that it had previously reviewed the issue of life jackets for water operations and that the requirement to wear life jackets by the occupants of an aeroplane, seaplane or an amphibian that is taking off or landing on water is contained in draft Civil Aviation Safety Regulation (CASR) Part 135. Specifically, the draft of CASR Part 135.825 (6), states that each occupant of a seaplane or amphibian that is taking off from or landing on water must wear a life jacket equipped with a whistle and a survivor locator light.
Operator
The operator has advised the ATSB that since the accident, the pilot had undertaken human factors training with the Civil Aviation Safety Authority, and that it will be implementing a range of safety actions including:
introduction of a wind limitation of 30 kts for commercial operations in the company aircraft landing area (ALA) register
monitoring of the Bureau of Meteorology's radar website by ground staff on days of frontal activity and anticipated windshear conditions
carriage of a portable wind speed meter for actual wind readings to be kept in the aircraft and used where doubt exists as to the wind strength
consideration will be given to lateral effects of loading passengers when conducting weight and balance calculations
requiring all passengers to wear an approved life jacket while on company aircraft
requiring all company pilots to complete Underwater Escape Training.
Significant Factors
Meteorological conditions were conducive to wind shear, mechanical turbulence or a combination thereof.
The pilot took off in a crosswind that exceeded the limitations specified in the Pilots Operating Handbook.
Analysis
The environmental conditions at the time of the accident required the pilot to take particular account of the prevailing sea conditions and the wind direction and speed, when selecting the area for, and direction of, the take-off. This led to the pilot making a compromise that placed emphasis on an area with a more favourable sea state rather than directly into the prevailing wind.
The local effects of the terrain gave the impression to the pilot that the wind at surface level in the area selected for the take-off was from the north-north-east. Therefore, he assessed that that wind direction was suitable for the take-off. However, it is likely that the aircraft encountered a crosswind during the take-off that exceeded the limitations in the Pilots Operating Handbook (POH). It was also likely that wind shear or mechanical turbulence, or a combination of both these effects, was encountered by the pilot shortly after take-off. At the point where the angle of bank of the aircraft exceeded 45 degrees, it is likely that the aircraft stalled causing it to strike the water.
The pilot reported that he was able to exit the aircraft quickly because of his previous underwater escape training. The Australian Transport Safety Bureau encourages all operators in this environment to ensure that their flight crews have completed similar training. The actions of the rear seat passenger were significant in enabling the remaining occupants to exit the aircraft.
The pilot and passengers did not have the time to retrieve their life jackets from under their seats before exiting the aircraft. This was also the case in the floatplane accident in Tasmania in 2001 (BO/200105932). Although the carriage of life jackets and the stowage of them below each of the seats was in accordance with Civil Aviation Order (CAO) 20.11 parts 5.1.4 and 5.1.5, the wearing of life jackets was not required by CAO 20.11 part 5.1.8, and as a consequence, their availability was not assured after the occupants of the floatplane had exited the aircraft into the water.
The lack of time available to retrieve and don life jackets in the event of an accident when operating close to, or on the water, has the potential to adversely affect the survivability of aircraft occupants after they have exited an aircraft. As highlighted in Federal Aviation Administration Advisory Circular (AC) 91-69A, it is extremely difficult for a person to don a life jacket when they are already in the water, and practically impossible to do so if the person is injured.
Summary
At 1735 eastern summer time on 20 January 2005, a Cessna Aircraft Company A185F floatplane, registered VH-SBH, with one pilot and three passengers on board was taking off on a water departure for a charter flight from Rose Bay aircraft landing area (ALA) to Palm Beach, NSW. Shortly after becoming airborne, the aircraft rolled 45 degrees to the left causing the left wing to strike the water. The aircraft became inverted and was substantially damaged. The four occupants escaped with minor injuries.
The pilot had positioned the floatplane to the eastern side of the ALA, approximately 200 m from the shoreline and to the west of a headland, to achieve more favourable sea conditions for a take-off to the north-north-west. The pilot reported that the wind direction was 010 degrees M at a speed of 20 kts. The intended take-off path ran approximately parallel to the headland in a direction of 350 degrees M.
The pilot reported selecting 20 degrees of flap for the take-off. As the aircraft was about to leave the surface, he selected 30 degrees of flap. This technique was used to help get the aircraft off the surface of the water quickly in difficult sea and/or weather conditions. He also reported that the aircraft took longer than he expected to reach take-off speed. The aircraft became airborne at 45 to 50 kts and he then selected 20 degrees of flap. At approximately 30 ft above the water, the aircraft commenced an uncommanded left roll that he was able to correct with full right aileron input. The aircraft then commenced a second uncommanded left roll that he was unable to correct with control inputs. The pilot, passengers and witnesses, all reported that the aircraft rolled more than 45 degrees to the left before the left wing struck the water.
The floatplane came to rest inverted and shortly after the cabin became submerged. The pilot reported that he had completed Helicopter Underwater Escape Training (HUET) previously, and that he thought that assisted him to exit the cabin quickly through the pilot's door, located on the left of the cabin. The passenger in the copilot's seat, located on the right of the cabin, was momentarily disorientated, but managed to undo his seat belt while the passenger in the middle row was attempting to locate and undo his seatbelt. The rear seat passenger was able to swim towards the front passenger and reported kicking open a door with her foot before pushing the front passenger out of the aircraft. She then returned to the middle row passenger and unfastened his seat belt buckle before pushing him out of the aircraft and then exiting the submerged cabin herself. One passenger reported that he was initially disoriented after the aircraft entered the water. In addition, given the rapid nature of the event and the need to exit the inverted cabin quickly, the passengers did not retrieve the life jackets which were stowed underneath their seats. It was likely that all passengers exited the floatplane via the pilot's door, because the co-pilot's door was still locked closed when the aircraft was recovered.
The floatplane stayed inverted with its floats remaining buoyant. After exiting the aircraft, the passengers were picked up by a passing boat. The pilot remained with the aircraft and secured it to a boat.
The load chart for the flight showed that the aircraft was within weight and balance limitations. The pilot was appropriately licensed and endorsed for the operation and was experienced in floatplane operations in Sydney Harbour. The aircraft was capable of normal operations before flight and there were no known maintenance issues.
A Bureau of Meteorology (BoM) report of the weather in Sydney Harbour at the time of the accident, showed that the prevailing wind around the time of the accident was from the north-east, averaging 26 to 29 kts, with gusts reaching 37 kts. The report also suggested that:
…in considering the wind shear that would have been experienced by a plane taking off from Rose Bay, the sheltering effect of the surrounding topography, especially the shielding of Rose Bay from north easterlies by the southern headland of Sydney Harbour, needs to be taken into account. It is conceivable that in passing from the relatively sheltered inshore waters of Rose Bay to a more exposed location, either through ascent or forward motion or both, that significant wind shear may have been experienced.
The pilot advised that he used a number of cues to determine the wind velocity, particularly the orientation of moored boats and flags, the BoM forecast and the water conditions.
Mountain waves and their turbulence can occur downwind of any obstacle, including an isolated hill a few hundred feet high. If the wind at the altitude of the top of the obstacle is 20 kts or more, there will be noticeable wave turbulence and significant downdrafts. This turbulence will be greatest in the rotor zone in the lee of the obstacle and will be at a maximum at about the same altitude as the top of the obstacle.1
The company ALA register notation for Rose Bay warned that 'Dumping will be encountered in winds over 20 kts from the North-East, South and West'. The significant downdrafts described in the previous paragraph are what the operator's ALA register referred to as 'dumping'.
A fact sheet on mountain wave turbulence that accompanied Australian Transport Safety Bureau (ATSB) report BO/200104092 into an accident involving mechanical turbulence stated in part that:
In addition to generating turbulence that has demonstrated sufficient ferocity to significantly damage aircraft or lead to loss of control, the more prevailing danger to aircraft in the lower levels in Australia seems to be the effect on an aircraft's climb rate. General Aviation aircraft rarely have the performance capability sufficient to enable the pilot to overcome the effects of a severe downdraft generated by a mountain wave, or the turbulence or the windshear2 generated by the rotor.
The Pilots Operating Handbook (POH) for the Cessna 185 indicated that the stalling speed in a 20 degree flap configuration, at a mid-range centre of gravity, was 55 kts. The POH also indicated a maximum demonstrated crosswind velocity for take-off and landing of 13 kts. The investigation determined that the crosswind for the accident flight would have been between 19 and 24 kts.
In December 2001, the ATSB investigated an accident involving a floatplane in Tasmania where the occupants had insufficient time to don life jackets before exiting the aircraft (see ATSB report BO/200105932). That accident investigation highlighted that regulations governing the use of life jackets, do not reflect the operational realities of exiting from an inverted submerged cabin.
Civil Aviation Order (CAO) 20.11 part 5.1.4 stated that:
Amphibious aircraft when operating on water, helicopters equipped with fixed flotation equipment when operating on water, and all seaplanes and flying boats on all flights shall be equipped with: (a) 1 life jacket for each occupant; and (b) an additional number of life jackets (equal to at least one-fifth of the total number of occupants) in a readily accessible position near the exits.
CAO 20.11part 5.1.4 stated that:
Life jackets shall be so stowed in the aircraft that 1 life jacket is readily accessible to each occupant and, in the case of passengers, within easy reach of their seats.
CAO 20.11 part 5.1.8 stated that:
Where life jackets are required to be carried in accordance with paragraph 5.1.4 each occupant of a single engine aircraft shall wear a life jacket during flight over water when the aircraft is operated beyond gliding distance from land or water, as appropriate, suitable for an emergency landing. However, occupants need not wear life jackets when the aircraft is taking off or landing at an aerodrome in accordance with a normal navigational procedure for departing from or arriving at that aerodrome, and occupants of aeroplanes need not wear life jackets during flight above 2 000 feet above the water.
Federal Aviation Administration Advisory Circular (AC) 91-69A contained recommendations and revised information for the safe operation of seaplanes. The AC stated that:
Life jackets in sealed pouches can be awkward to remove and don in a flooded aircraft. When a survivor attempts to put on a jacket in the water, it may be difficult to find and fasten its straps and hooks. It would take considerable effort to accomplish the combined maneuver [sic] of pulling a lifejacket over one's head while in the water trying to stay afloat. If a life preserver is not worn before flight, it is practically impossible for a survivor with an injured arm, for example, to don the life preserver in time for it to be effective for survival. Wearing an uninflated TSO C13f life preserver at all times in the seaplane and inflating it only after exiting the seaplane would seem to be the best protection.
Furthermore, the AC stated that after a seaplane accident:
and especially while submerged inverted in water, the passengers are likely to become disoriented and panic.
It also stated that:
Maneuvring [sic] while holding flotation devices can also be disorienting because it occupies the hands, making swimming or treading water difficult.
Additionally the AC stated in Section 1.b. (1)
For-hire operators must use FAA-approved PFD's. A PFD should be worn by each occupant while on the seaplane.
1. Modern Airmanship, Eighth Edition, Van Nostrand Reinhold Company, New York, 1999.
2. A change of wind velocity with distance along an axis at right angles to wind direction, specified vertically or horizontally. Recognised as an extremely dangerous phenomenon because encountered chiefly at low altitude (in squall or local frontal systems) in approach configuration at speed where it makes sudden and potentially disastrous difference to airspeed and thus lift.
On 21 November 2004, the crew of a Fairchild Industries SA227-AC Metro III aircraft, registered VH-TAG, was conducting an endorsement training flight near Lake George, 33 km north-east of Canberra Airport. The flight included a planned in-flight engine shutdown and restart, conducted at an altitude below 4,500 ft (about 2,200 ft above ground level (AGL)). During the engine restart preparation, the instructor departed from the published procedure by moving the power lever for the left engine into the beta range and directing the pilot to select the unfeather test switch. These actions were appropriate to prepare an engine for start on the ground with a feathered propeller, but not during an air start.
As a result, the propeller on the left engine became fixed in the start-locks position. The crew lost control of the aircraft, and it descended 1,000 ft, to about 450 ft AGL, before they regained control. The crew could not diagnose the source of the loss of control and proceeded to start the left engine while the propeller was fixed on the start-locks. As a result, the crew lost control of the aircraft for a second time and it descended 1,300 ft, to about 300 ft AGL, before they regained control.
The SA226 / SA227 aircraft contain no lockout system to prevent pilots from intentionally moving the power lever into the beta range during flight. It was the first time the instructor had given a Metro endorsement, and he was subject to time pressure to complete the endorsement. His ongoing difficulties in adapting to his employment tasks were not successfully dealt with by the operator. He had a limited understanding of the aircraft's engine and propeller systems, and had not practiced an air start for 8 years as the CASA check and training approval did not include an assessment of all flight critical exercises.
Appendix A: Radar data relating to Mooney M20K VH-DXZ
Time (EST)
Altitude (ft AMSL)
Groundspeed (kts)
Explanatory notes
2014:01
1440
189
2014:04
1440
189
2014:08
1340
183
2014:12
1340
183
2014:15
1240
183
2014:19
1240
183
2014:23
1140
183
Overhead Caloundra
2014:26
1240
183
2014:30
1240
183
2014:34
1342
183
2014:38
1342
179
2014:41
1342
177
2014:45
1342
185
2014:49
1242
179
2014:52
1242
165
2014:56
1242
176
2014:59
1142
172
2015:03
1142
172
2015:07
1042
182
2015:11
1042
182
2015:14
1042
182
2015:18
1042
182
2015:22
942
182
2015:25
942
182
2015:29
842
182
2015:33
842
182
2015:37
742
182
2015:40
742
183
2015:44
642
183
2015:48
642
183
2015:51
542
185
2015:55
542
179
2015:59
442
189
Minimum recorded altitude
2016:02
542
185
2016:06
642
186
2016:10
742
183
2016:13
642
173
Last valid radar return
Safety Action
Previous recommendation
On 23 October 2002 the ATSB issued the following recommendation as a result of a fatal accident at night near Newman, WA, (ATSB Investigation BO/200100348):
Recommendation R20020193 The Australian Transport Safety Bureau recommends that the Civil Aviation Safety Authority (CASA) review the general operational requirements, training requirements, flight planning requirements and guidance material provided to pilots conducting VFR operations in dark night conditions.
On 13 December 2002, CASA responded to the recommendation as follows:
CASA acknowledges the intent of this Recommendation. As part of the proposed CASR [Civil Aviation Safety Regulations] Part 61, CASA is developing the requirements for night VFR ratings which will be based on the existing Civil Aviation Order CAO 40.2.2. In addition, a draft competency standard for night visual flight operations has been developed for inclusion in the proposed CASR Part 61 Manual of Standards. CASA plans to publish a Notice of Proposed Rule Making [NPRM] in relation to this matter in March 2003.
During July 2003, CASA published NPRM 0309FS Flight Crew Licensing and Draft Part 61 Manual of Standards [MOS]. The draft MOS included a requirement for a periodic flight review of night flying competencies. On 24 November 2004, the Chief Executive Officer of CASA issued two directives related to the regulatory reform process. As of March 2005, CASA was working on the processes necessary to apply the directives to the development of new CASR parts, including Part 61. In a letter to the ATSB dated 6 January 2006, CASA advised that the proposed CASR Part 61 would require night VFR rating holders to undergo flight reviews covering night and instrument flying, in addition to structural changes to the night VFR rating. CASA advised that Part 61 could be completed in the second half of 2006.
During March 2005, the ATSB issued Aviation Safety Investigation report BO/200304282 on the fatal night accident involving a Bell 407 helicopter, registered VH-HTD, which occurred off Cape Hillsborough, Queensland, on 17 October 2003. The report stated that CASA had advised that they intended to issue a CAAP (Civil Aviation Advisory Publication) to clarify safety guidelines for night VFR operations. In a letter to the ATSB dated 6 January 2006, CASA advised that the Night VFR CAAP was in the final stages of preparation, and it was intended that it would be published in the first quarter of 2006. The CAAP would include competency standards for night and instrument flying.
CASA has also advised that copies of a night VFR-related 'Briefing in a Box' were distributed to flying schools in March 2006. The briefings included safety material on night flying and were intended to assist flying instructors and flying schools in providing appropriate training to night VFR pilots.
Analysis
The investigation was unable to establish why the pilot lost control of the aircraft during a climbing turn while apparently returning to land at Caloundra aerodrome.
However, the following issues are considered to have been significant to the circumstances of the accident.
Aircraft altitude
The altitude of the aircraft as it passed over Bokarina was well below the minimum permissible for a night visual flight rules (VFR) flight, and was also below the minimum for a flight over a populated area. The aircraft's maximum altitude of 742 ft after it crossed the coast provided little margin for inadvertent height loss during the subsequent turn, and was evidently insufficient to allow the pilot to regain control of the aircraft.
Aircraft systems
There was no indication from the recorded radar information that the performance of the aircraft was abnormal. No radio transmission was heard from the pilot to indicate any problem with the aircraft.
Although one witness at Bokarina described the engine noise as abnormal, three other witnesses described the sound as normal and there was clear physical evidence that the engine was operating at high power at impact. There was also evidence that electrical power was being delivered to the lights, and that pneumatic power was being delivered to the gyroscopic instruments.
There was no evidence of a defect that could have affected the controllability of the aircraft. However, impact damage and the unavailability of some parts of the aircraft prevented a comprehensive assessment of the pre-impact serviceability of the flight control system.
Physiological and cognitive factors
The aircraft's recorded cruise altitude of 11,300 ft was above the altitude at which the Civil Aviation Safety Authority (CASA) required supplemental oxygen to be used, but was below the altitude above which oxygen should be used according to the aircraft flight manual.
By flying at 11,300 ft without supplemental oxygen, the pilot increased his risk of developing hypoxia. However, any hypoxic effect on the pilot's performance could not be quantified. The aircraft's steady track and descent profile prior to passing overhead Caloundra suggest that the pilot, probably assisted by the autopilot, was effectively controlling the aircraft. Further, any adverse physiological effects of mild hypoxia would have reduced before the final stages of the flight. However, it is possible that the pilot's cognitive function during the latter part of the flight was affected by earlier exposure to hypoxic conditions.
The duration of the day's flying, together with an inadequate food intake, could have caused the pilot to become fatigued.
Fatigue and hypoxia have been demonstrated to adversely affect areas of cognitive function such as response time, decision-making and risk assessment. Any decrement in cognitive function could have reduced the pilot's ability to identify the reduced level of safety associated with conducting a low-level flight at night over a populated area, and transitioning from an area of extensive ground lighting to an area where surface features and the natural horizon were difficult to discern. However, there was no means of determining if the pilot's cognitive function had been adversely affected. Nor was it possible to determine that if affected, it had not recovered to its normal state once the pilot was no longer exposed to hypoxic conditions.
The pilot's reported difficulties with balance following the April 2002 stapedectomy and subsequent removal of the prosthesis were consistent with expected side-effects of the operations. While these difficulties persisted for some months after the operation, the available evidence indicated that the pilot was not affected by dizziness or balance problems in the months preceding the accident.
Spatial disorientation
The forecast weather conditions did not preclude night VFR flight, and witness reports indicated that there was no reduction in visibility due to smoke or cloud at the time of the accident. The pilot's attention was probably directed outside the cockpit as he positioned the aircraft to fly over his home. Extensive ground lighting associated with the populated Sunshine Coast area would have provided him with good surface and horizon reference during that period. However, after the aircraft turned east, it was heading towards an area of no surface lighting (other than that provided by one or two large ships), and minimal celestial illumination. Consequently, surface features and the natural horizon would have been difficult to discern. Those conditions required that the pilot transition to flight by reference to the aircraft instruments.
The pilot's recorded night flight time indicated that he satisfied the recency requirements for night VFR. Further, the pilot was flying a familiar aircraft, which was suitably equipped (including a standby pneumatic power source) and maintained for instrument flight. However, the pilot had not demonstrated competence in flight solely by reference to instruments since 1998. The Federal Aviation Administration Advisory Circular 60-4A indicated that even qualified instrument pilots can take up to 35 seconds to complete the transition from visual to instrument flight. If the pilot did not achieve a rapid and complete transition to instrument flight during the climbing turn, it is likely that he would have experienced the effects of spatial disorientation.
Because there was no regulatory requirement that the pilot's recurrent aeroplane flight reviews include night VFR or instrument flight, his level of recent competence could not be assessed. The pilot's ability to transition to flight solely by reference to instruments may have been adversely affected by various factors, including a lack of recent experience in instrument flight, possible residual effects of hypoxia, fatigue, and/or a distraction in the cockpit. If the pilot's attention was directed elsewhere, he may not have initially recognised that the aircraft was descending, or the degree to which it was turning after it crossed the coast.
The ability to maintain visual reference with surface features and the natural horizon at night is not assured, even in meteorological conditions that satisfy the night VFR requirements. Consequently, as the Flight Safety Australia (May-June 2005) article advised, it is imperative that night VFR pilots are competent and current in instrument flight. Completing an aeroplane flight review and satisfying the night VFR requirements may not sufficiently reduce the risk of spatial disorientation of a pilot during night VFR operations.
Conclusions
The circumstances of the accident are consistent with a loss of control due to the pilot becoming spatially disoriented after flying into an area of minimal surface and celestial illumination. Physiological and cognitive factors may have contributed to the development of the accident. However, the factors that contributed to the aircraft descending into the water could not be conclusively established.
This accident highlights the need for night VFR pilots to manage the risk of spatial disorientation in dark night conditions by maintaining proficiency in instrument flight.
Factual information
FACTUAL INFORMATION
History of the flight
At about 1730 Eastern Standard Time on 15 August 2004, the pilot of a Mooney Aircraft Corporation M20K aircraft, registered VH-DXZ, departed Cobar, NSW, on a private flight to Caloundra, Qld. The flight was conducted under the visual flight rules (VFR), with the latter part at night.
At about 2015, several people saw and heard the aircraft, with its wing tip strobe lights flashing, flying low in a northerly direction over Bokarina, 8 km north-north-east of Caloundra aerodrome. One witness said that the engine sounded as though it was 'struggling and cutting out'. Two other witnesses described the engine sound as a 'steady drone', while another said it sounded like it was 'turning at low [revolutions], as if it was powered down for a landing'.
The aircraft was then observed to turn east and cross the coast before descending steeply and impacting the water. The impact was accompanied by a bright flash. The aircraft wreckage was located 4 days later, approximately 1.5 km east of Bokarina beach, at a depth of about 16 m. The pilot, who owned the aircraft and was the sole occupant, did not survive the impact.
Earlier that afternoon, the pilot had flown from Caloundra to Cobar with one passenger. The passenger remained at Cobar and reported that the flight from Caloundra had been uneventful and that they arrived at Cobar at about 1700. The refueller advised that the pilot refuelled the aircraft with 156 L of avgas (apparently to full tanks) and checked the engine oil before departing on the return flight to Caloundra.
The pilot lived at Bokarina and family members reported that he did not normally fly over his home on returning from a flight. They indicated that the pilot's car was at the aerodrome, so he did not need to be met and driven home. They assumed that the purpose of flying over the house was to let them know that he would be home soon.
Recorded information
The pilot was not required to report to air traffic control during the flight and there was no record of him having done so. The Caloundra Common Traffic Advisory Frequency did not have a recording capability.
A pilot conducting a VFR flight was required to operate the aircraft's secondary surveillance radar (SSR) transponder on code 1200 in airspace not subject to air traffic control. The Mooney's SSR track for the flight was recorded by The
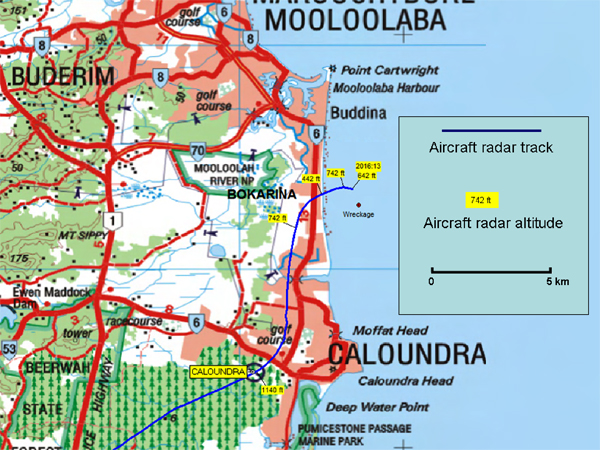
Australian Advanced Air Traffic System. That data showed that the aircraft first appeared on radar at 1903, north of Moree, NSW, on the direct track from Cobar to Caloundra at 11,300 ft. The aircraft maintained that altitude until 1937, when it commenced descent, passing through 10,000 ft at about 1940, and 5,000 ft at about 1958. It maintained a steady track and descent profile, and was overhead Caloundra at 2014, at 1,140 ft. The aircraft then maintained a relatively constant altitude and tracked north towards Bokarina (Figure 1).
At 2015, the aircraft commenced a further descent and when overhead Bokarina, turned right and headed east-north-east, towards the ocean. Radar data indicated that the aircraft descended to 442 ft about the time it flew over the beach. The aircraft's altitude then increased, reaching a maximum of 742 ft. The last valid radar information was recorded at 2016:13, and indicated that the aircraft had entered a descending right turn. The recorded radar data did not reveal any abrupt or abnormal changes in the aircraft's altitude, groundspeed, or track. The recorded speeds were consistent with normal cruise and descent speeds for the aircraft type (Appendix A).
Figure 1: The aircraft's radar-recorded track
Pilot information
The pilot purchased the aircraft in May 1994, and was issued with a private pilot (aeroplane) licence in July 1994. His logbook recorded his total flying experience at the time of the accident as about 1800 hours, 142 of which were at night. In April, May and June 2004, the pilot logged 5, 0.5 and 5.4 hours night flying respectively, all in DXZ. In those same months, he also logged 20.8, 12.3, and 25.4 hours day flying. The pilot last flew at night on 19 June 2004, and in actual or simulated instrument meteorological conditions, during 1998. His total instrument flight time was recorded as 32.4 hours.
The pilot was issued with a night VFR rating on 11 June 1998. There was no evidence that he had ever held an instrument rating. His three most recent flight reviews were completed on 29 March 2003, 18 November 2001, and 24 November 2000. They were logged as day flights, with no instrument or night flight recorded.
The pilot's family reported that he was well rested before the flight, was not affected by any illness and had never smoked cigarettes.
A person who spoke to the pilot while he was at Cobar reported that he said that it had been a busy day, and that he had not had any lunch, but was carrying some nuts and a drink on the aircraft.
Aircraft information
The aircraft was manufactured in the US in 1988 and was imported into Australia in the same year. At the time of the accident, it had accumulated about 2,868 flight hours. The aircraft was equipped and maintained in the instrument flight rules (IFR) category. It was fitted with a turbo-charged, piston engine which had accumulated about 180 hours since the last overhaul.
The aircraft cabin was not pressurised but was fitted with a supplemental oxygen system. The organisation that maintained the aircraft reported that the supplemental oxygen system tank was empty. There was no indication that the oxygen tank had been charged at Cobar.
A review of the aircraft's maintenance records revealed that the requirements of Airworthiness Directives (AD) RAD/43 and RAD/471 were due to be completed in July 2004 but had not been carried out. No other discrepancies were noted, and no defects had been recorded on the maintenance release.
The aircraft was fitted with an electrically driven standby vacuum system for providing pneumatic power to the gyroscopic instruments, and a Century 2000 autopilot system.
Meteorological information
Information provided by the Bureau of Meteorology indicated that the weather conditions in the Bokarina area at the time of the accident were benign. Smoke areas were forecast below 6,000 ft with visibility reducing to 4,000 m in smoke, and 1,000 m in thick smoke. The terminal area forecast for Maroochydore aerodrome (15 km north-north-west of Bokarina), issued at 1813, predicted visibility greater than 10 km and scattered cloud at 3,000 ft. None of the witnesses reported that smoke, cloud or haze affected their ability to see the aircraft.
The QNH2 recorded by the automatic weather station at Maroochydore at 2020 on the day of the accident was 1014 hPa.
On 15 August 2004 at the accident location, astronomical twilight occurred at 1846 and the moon set at 16373. Two cargo ships were located east of Maroochydore at the time of the occurrence, at least one of which was at anchor, and therefore displaying lights4. Several hours after the accident, witnesses observed two large ships moored east of Maroochydore which were displaying deck lights.
Wreckage and impact information
The wreckage was raised from the seabed on 28 August 2004 (Figure 2). Most of the aircraft was recovered, including the engine, fuselage, left wing, all three propeller blades and the propeller hub. The right horizontal stabiliser, right elevator, and parts of the right wing were not recovered.
An examination of the wreckage indicated that:
The aircraft was banked right, and in a nose-down attitude of approximately 45 degrees when it struck the water.
The nature of the damage to the engine crankshaft and the propeller blades was consistent with the engine delivering high power at impact.
The frangible plastic drive shaft of the engine driven vacuum pump had failed under a sideways load. The drive shaft of the electrically driven vacuum pump was intact.
Damage to the gyroscopes in the artificial horizon and directional indicator flight instruments was consistent with gyroscopic rotation at impact.
The light globes in the artificial horizon and the directional indicator flight instruments were receiving electrical power at impact.
The landing gear was retracted, and the wing flaps were extended about 10 degrees, at impact.
The altimeter subscale was set at 1015.
There was evidence of a short duration, post-impact fire.
Impact and saltwater corrosion damage precluded a determination of the serviceability of the automatic pilot system and its operational status during the final stages of the flight. None of the windscreen was recovered. There was no evidence in the recovered wreckage that the aircraft had struck a bird or a bat during flight.
The extent of airframe disruption and the missing parts of the right wing, horizontal stabiliser and right elevator prevented a comprehensive assessment of the functionality of the flight controls at impact.
Figure 2: Recovery of the main wreckage
Regulatory aspects
The pilot's night VFR rating authorised him to act as pilot in command of private or aerial work flights at night under the VFR. Civil Aviation Order (CAO) 40.2.2 detailed the flight tests and other requirements for the issue of a night VFR rating. The test requirements included recovery from unusual attitudes, basic turns, and straight and level flight, which were required to be conducted solely by reference to flight instruments. The CAO also required that training for the issue of a night VFR rating included at least one landing at an aerodrome 'that is not in an area that has sufficient ground lighting to create a discernible horizon'.
Once issued, a night VFR rating remained permanently valid. To exercise the privileges of the rating, a pilot needed to meet certain minimum recent experience requirements. There was no requirement for the holder of a night VFR rating to have any recent instrument flight time prior to conducting a flight at night 5.
Except during take-off, landing, or radar vectoring, the pilot of a night VFR flight was required to ensure than the aircraft remained at or above the calculated lowest safe altitude (LSALT) while further than 3 NM from the destination aerodrome. The minimum LSALT for the Bokarina area was 1,500 ft. Aircraft operating overpopulated areas were generally required to remain at or above 1,000 ft.
A pilot was required to satisfactorily complete an aeroplane flight review every 2 years. There were no published requirements or guidance material regarding theoretical knowledge or practical skills (such as flight conducted solely by reference to flight instruments) required to be demonstrated by pilots undergoing an aeroplane flight review.
Medical and pathological information
The pilot held a valid Class 2 Medical Certificate at the time of the occurrence. His medical records indicated that he had undergone a stapedectomy6 operation on his left ear about 22 years before the accident. He underwent a stapedectomy on his right ear on 11 April 2002 because of hearing loss. However, due to a post-operative decline in hearing and persistent balance problems, the prosthesis was removed on 24 April 2002. During two subsequent telephone conversations with the surgeon in June and July 2002, the pilot reported that he was still dizzy, couldn't look up and down quickly, and was still unsteady.
The pilot underwent a Class 2 aviation medical examination on 1 March 2004. The designated aviation medical examiner who performed that examination reported that the pilot had advised of no ongoing dizziness, disorientation, or other related problems.
A pathological examination did not identify any indication of a pre-existing medical condition that could have contributed to the development of the accident. It was not possible to establish when, or what, the pilot had last eaten.
Hypoxia
Hypoxia is a condition in which there is reduced oxygen supply to the body. Available oxygen decreases with increased altitude, such that at 12,000 ft, brain oxygen saturation is approximately 87%, compared with sea level saturation of 96%. The investigation calculated that if the entire cruise segment of the flight had been conducted at 11,300 ft, the aircraft would have been at that level for almost 2 hours.
The US Federal Aviation Administration7 (FAA) recommended that pilots use supplemental oxygen when flying above 10,000 ft during the day and above 5,000 ft at night when the eyes become more sensitive to oxygen deprivation.
The Mooney M20K Aircraft Flight Manual stated that 'supplemental oxygen should be used when cruising above 12,500 feet. It is often advisable to use oxygen at altitude lower than 12,500 feet under conditions of night flying, fatigue, …'. Civil Aviation Order (CAO) Part 20.4 paragraph 6.1 stated:
A flight crew member who is on flight deck duty in an unpressurised aircraft must be provided with, and continuously use, supplemental oxygen at all times during which the aircraft flies above 10,000 feet altitude.
An article8 in Flight Safety Australia magazine stated '[a]fter vision, the tissues most affected by hypoxia are those areas of the brain associated with judgement, self-criticism and the accurate performance of mental tasks'. An associated article9 in the same magazine indicated that the use of oxygen during night flight below 10,000 ft resulted in an increase in alertness and cognitive function, and a reduction in fatigue. Studies of the effects of exposure to altitudes between 10,000 ft and 15,000 ft have consistently shown small to moderate effects on human performance. Those effects included a reduction in night and peripheral vision, increased drowsiness, decreased response time, decreased short-term memory capacity, and poorer performance on complex and reasoning tasks.
The FAA Civil Aerospace Medical Institute Human Factors Research Laboratory in Oklahoma City, USA advised that restoration of a sea level atmosphere following exposure to hypoxic conditions caused rapid physiological recovery, but that cognitive recovery was slower.
Fatigue
Fatigue results from inadequate rest over a period of time, and leads to physical and mental impairment. The effects of fatigue include decreased short-term memory, slowed reaction time, decreased work efficiency, increased variability in work performance, a tendency to accept lower levels of performance and not correct errors. Not consuming food regularly is known to exacerbate the effects of fatigue. Based on previous flights recorded in the pilot's logbook, the total flight time for the trip from Caloundra to Cobar and return to Caloundra would probably have been between 6.4 and 6.9 hours.
Stapedectomy
Stapedectomy involved a small risk of ongoing episodes of dizziness and hearing loss10. However, according to an article published in 1998 in the journal Otolaryngology - Head and Neck Surgery11,
The FAA [Federal Aviation Administration] has always had the most experience with aircrew returning to flying duties after stapedectomy. The civilian track record is excellent with no reported cases of sudden incapacitating vertigo, sudden hearing loss, or other poststapedectomy related sequelae.
Spatial disorientation
Spatial disorientation describes an in-flight situation in which a pilot does not correctly sense the position, motion or attitude of the aircraft, and may be unable to tell which way is up. A pilot operating under the VFR determines the attitude of an aircraft by reference to the natural horizon or surface features. If these references are not visible, the pilot must use the flight instruments to determine the aircraft's attitude.
The risks of non-instrument rated pilots flying in conditions in which they are not able to orientate the aircraft by visual reference have been well known for over 50 years. During testing conducted on a group of non-instrument rated pilots, the average time before loss of control of the aircraft, after visual reference was lost, was 178 seconds12. An article titled 'Fatal Night Flight' in the Civil Aviation Safety Authority (CASA) magazine Flight Safety Australia (May-June 2005) stated that:
[v]isual disorientation is a distinct possibility on dark nights or away from areas of extensive ground lighting. Disorientation can be caused by sudden loss of visual reference such as when turning away from a well lighted area towards an area without ground lighting.
The article also stated that 'it is imperative that Night VFR pilots are competent and current in instrument flight'.
US FAA Advisory Circular 60-4A, Pilot's Spatial Disorientation, was published in 1983 and was intended to inform pilots of the hazards associated with disorientation caused by loss of visual reference with the surface. It included the following information:
Tests conducted with qualified instrument pilots indicate that it can take as much as 35 seconds to establish full control by instruments after the loss of visual reference with the surface.
Surface references and the natural horizon may at times become obscured, although visibility may be above visual flight rule minimums. The lack of natural horizon or surface reference is common on over water flights, at night, and especially at night in extremely sparsely populated areas, or in low visibility conditions.
Recent night VFR accident
On the evening of 17 October 2003, an air ambulance Bell 407 helicopter descended into the sea near Mackay, Qld. The ATSB investigation (200304282) was unable to determine, with certainty, what factors led to loss of control of the helicopter. The investigation considered that although the forecast weather conditions did not necessarily preclude flight under the night VFR rules, the lack of a visible horizon and surface lighting, and the pilot's limited instrument flying experience may have contributed to the accident. The investigation concluded that the circumstances of the accident were consistent with loss of control due to the pilot becoming spatially disoriented.
AD/RAD/43 required a biennial altimeter and encoder check and AD/RAD/47 required a biennial transponder check.
Vessels over 100 m long and at anchor are required to display white lights at either end of the vessel and available working lights or equivalent to illuminate the decks.
In contrast, the holder of an instrument rating was required to undergo an annual instrument flight test, and comply with flight and instrument approach recency requirements, in order to keep the instrument rating current.
Stapedectomy is an operation to remove the fixed stapes [the third middle ear bone] and to replace it with a prosthesis. That allows sound vibrations to be transmitted properly to the inner ear for improved hearing. http://www.bcm.edu/oto/clinic/educate/stapled.html
Federal Aviation Administration. 2003. Advisory Circular AC 61-107A Operations of Aircraft at Altitudes Above 25,000 feet MSL and/or Mach Numbers (MMO) Greater than .75.
Brock, J. & Bencke, R. 1998. Hypoxia. Flight Safety Australia. Volume 3 Number 1. Civil Aviation Safety Authority. Canberra.
Thom, A. 1998. Improved Performance. Flight Safety Australia. Volume 3 Number 1. Civil Aviation Safety Authority. Canberra.
Thiringer, J.K. & Arriaga, M.A. 1998. Stapedectomy in Military Aircrew. Otolaryngology - Head and Neck Surgery. Volume 118 Number 1. January 1998.
Bryan, L.A., Stonecipher, J.W. & Aron, K. 1954. 180-degree turn experiment. University of Illinois Bulletin. 54(11), 1-52.
Summary
At about 2017 Eastern Standard Time on 15 August 2004, a Mooney Aircraft Corporation M20K aircraft, registered VH-DXZ, descended into the ocean off Bokarina, Queensland. The pilot, who owned the aircraft and was the sole occupant, did not survive the impact.
The pilot held a private pilot (aeroplane) licence and a night visual flight rules (VFR) rating. His logbook recorded his total flying experience at the time of the accident as about 1800 hours, 142 of which were at night. The pilot last flew at night on 19 June 2004, and in actual or simulated instrument meteorological conditions, during 1998. His three most recent flight reviews were logged as day flights, with no instrument or night flight recorded.
The weather conditions in the area at the time of the occurrence were benign. Astronomical twilight occurred at 1846 and the moon set at 1637.
The wreckage was recovered 13 days after the accident. An examination revealed that at the time of impact; the engine was delivering high power, the instrument lights were receiving electrical power, and the gyroscopic instruments were receiving pneumatic power.
The circumstances of the accident are consistent with a loss of control due to the pilot becoming spatially disoriented after flying into an area of minimal surface and celestial illumination. Physiological and cognitive factors may have contributed to the development of the accident. However, the factors that contributed to the aircraft descending into the water could not be conclusively established.
This accident highlights the need for night VFR pilots to manage the risk of spatial disorientation in dark night conditions by maintaining proficiency in instrument flight.