Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On the afternoon of 12 November 2025, an instructor and student pilot departed Archerfield Airport, Queensland, for a navigational training flight in a Piper Aircraft Corporation PA-28R aircraft.
Following several hours of exercises, the flight was tracking east and transiting the Amberley Airport control zone at 1,500 ft when the entire upper engine cowling separated from its attachment points and flipped backward against the cockpit windshield, partially obstructing both pilots’ forward visibility.
Maintaining control of the aircraft and aware of their proximity to Amberley Airport, the crew immediately assessed the engine operation and aircraft handling – finding both unaffected. The crew called PAN PAN[1] to Amberley approach air traffic control and turned toward the aerodrome to conduct an approach to runway 15. After ATC advised of significant crosswinds for that runway and mindful of their very limited forward visibility, the crew re‑positioned for an approach to runway 04.
During the turn onto the base leg of the runway 04 approach, the cowling fractured into 2 sections, with the right side separating from the aircraft and the left side moving downward and away from the windshield, remaining attached to the aircraft. The final approach and landing were uneventful.
Engineering aspects
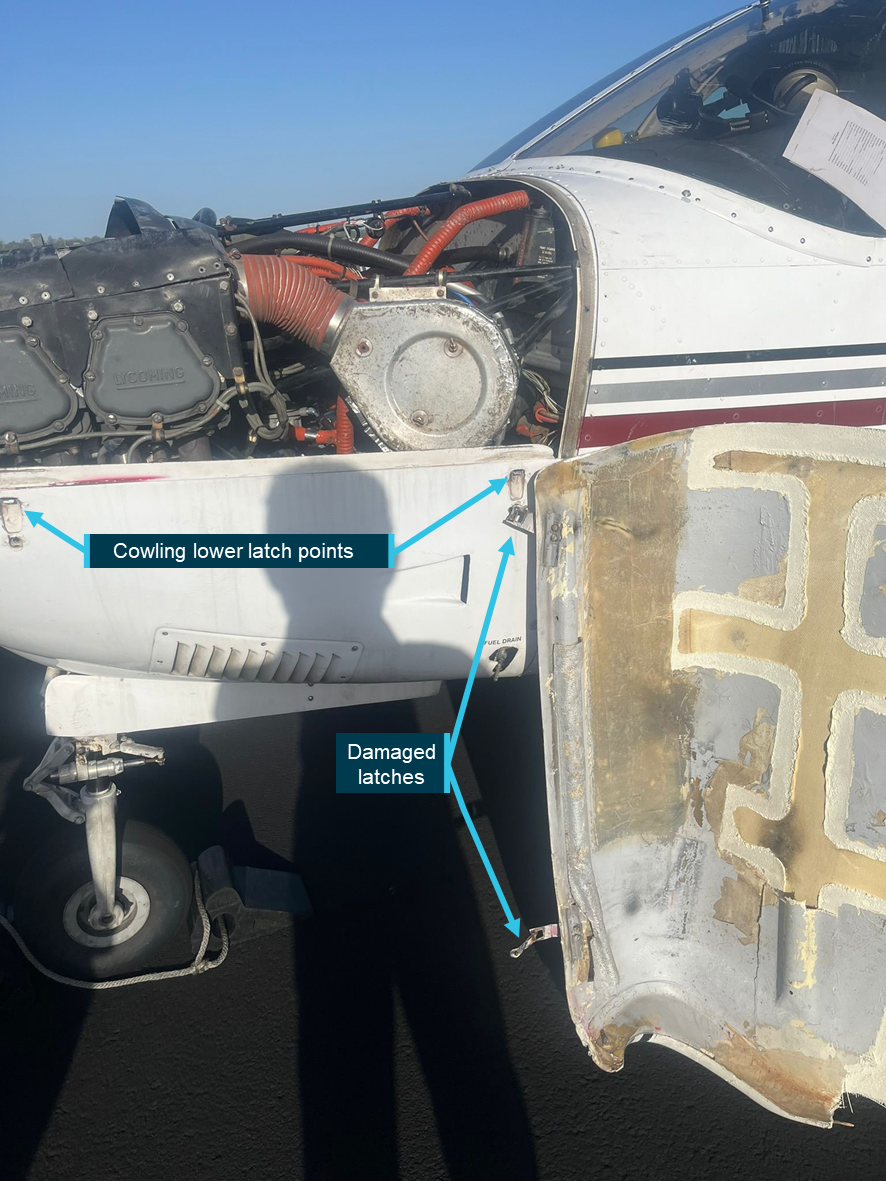
The PA-28 engine upper cowling is a shaped single-piece composite fibre structure that affixes to the lower cowling with 4 over-centre toggle style latches (2 on each side). The instructor reported that all latches were checked for security and tightness during the aircraft’s pre-flight inspection and noted that the flight had operated normally for around 3 hours before the separation. No defects or related issues were annotated in the aircraft’s maintenance release.
The reason/s for the cowl separation remain unknown.
Figure 1: Remaining cowl section and left separation points
Source: Supplied by operator, annotated by the ATSB
Safety message
The well-managed response to this significant in-flight emergency ensured the safe recovery of the aircraft and crew. The methodical approach to the problem assessment, decision-making and utilisation of ATC assistance is a good illustration of best-practice emergency management.
The unintended and sudden in-flight separation of cowlings or other airframe components has the potential to interfere with aircraft controllability, engine operation, or – in the worst-case scenario – cause pilot incapacitation should the components forcefully enter the cockpit through the windshield.
Maintenance attention and airworthiness inspections must have regard to the security and ongoing mechanical condition of all cowlings, panels and their fixtures.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-061
Occurrence date
12/11/2025
Location
8 km north-west of Amberley Airport
State
Queensland
Occurrence class
Serious Incident
Aviation occurrence category
Diversion/return, Fuselage/wings/empennage, Objects falling from aircraft
Highest injury level
None
Brief release date
23/12/2025
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-28R
Sector
Piston
Operation type
Part 142 Integrated and multi-crew pilot flight training
In August 2024, a Saab 340B aircraft was being operated on a scheduled air passenger transport flight from Canberra, Australian Capital Territory, to Sydney, New South Wales.
During the approach to Sydney, the flight crew reported hearing a sound consistent with a pressurisation issue and detected an increase in cabin pressure. A normal approach and landing was conducted. Post-flight inspection found a VHF antenna had separated from the fuselage with an associated fracture of the fuselage skin. The antenna remained attached to the aircraft by its cabling.
The ATSB received a request for assistance from the Civil Aviation Safety Authority (CASA) to conduct a technical examination of the antenna installation. The ATSB commenced an external investigation under the provisions of the Transport Safety Investigation Act 2003.
The ATSB has concluded the examination of the installation of the antenna and provided CASA with an examination report.
Any enquiries relating to the investigation should be directed to CASA.
Aircraft details
Manufacturer
Saab Aircraft Co.
Model
Saab 340B
Registration
VH-VEA
Serial number
340B-406
Aircraft operator
Vee H Aviation Pty Ltd
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
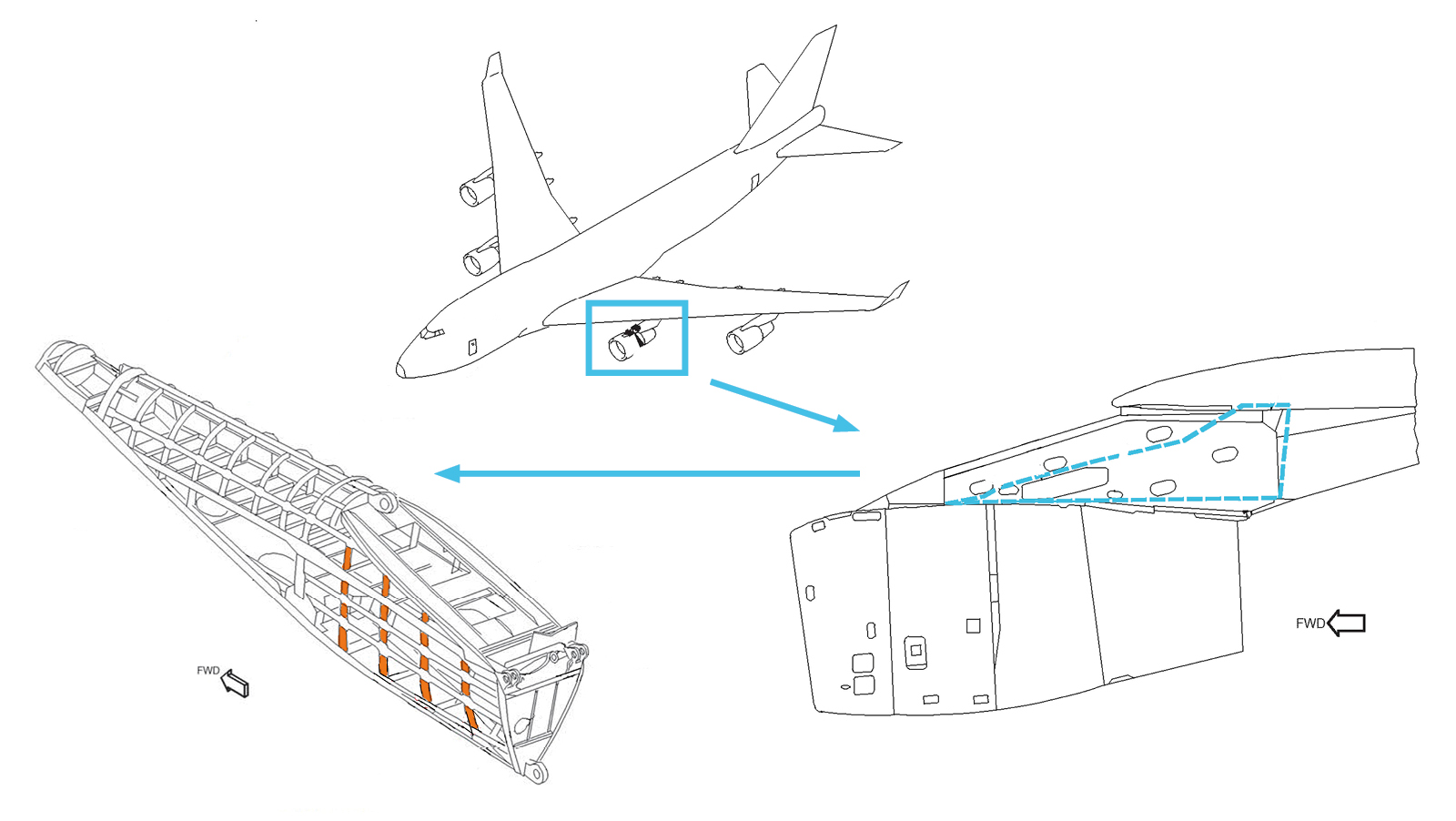
On 5 October 2016, a Qantas-operated Boeing 747-438 aircraft, registered VH-OJT (Figure 1) was undergoing routine maintenance at a contracted repair and overhaul facility in the Hong Kong Special Administrative Region (SAR) in the People’s Republic of China. Inspection of the No. 2[1] engine pylon identified cracking of four outboard strut ribs from within the torque box of the pylon (Figure 2).
Following technical advice from Boeing, the No. 2 engine was removed from its wing installation to allow access to the pylon and removal of the cracked strut ribs. The aircraft was repaired and, after completing the maintenance visit, it was returned to regular passenger service. The cracked ribs were sent to Boeing’s facilities in the United States for specialist metallurgical examination.
Figure 1: Qantas Boeing 747-438 aircraft, registered VH-OJT
Source: Christopher Chai
Pylon inspection requirements
The engines on a Boeing 747 aircraft are mounted to pylons located on the underside of each wing. The pylons transmit thrust from the engine to the airframe and are designed to withstand flight loads from normal operation along with transient dynamic loading in the event of an engine failure. Hydraulic, fuel, electrical and air conditioning lines all pass through the pylon structure.
Boeing’s ongoing maintenance requirements included an inspection of the engine pylon every 48 months. A general visual inspection within the torque box for corrosion damage was required along with a more detailed inspection for cracking of the ribs. The procedures noted that during the inspection, particular attention should be applied to the cutaway where stringers passed through each rib.
Qantas reported to the ATSB that several years prior to this occurrence, it had independently increased the frequency of the zonal inspections from 48 to 24 months due to repeated instances of corrosion and cracking damage within the pylon region. That new inspection interval was formalised by Qantas within its maintenance documentation for its 747 fleet.[2]
Figure 2: Boeing 747 engine pylon showing the location of the cracking (highlighted)
Source: Boeing, annotated by the ATSB
Manufacturer’s examination
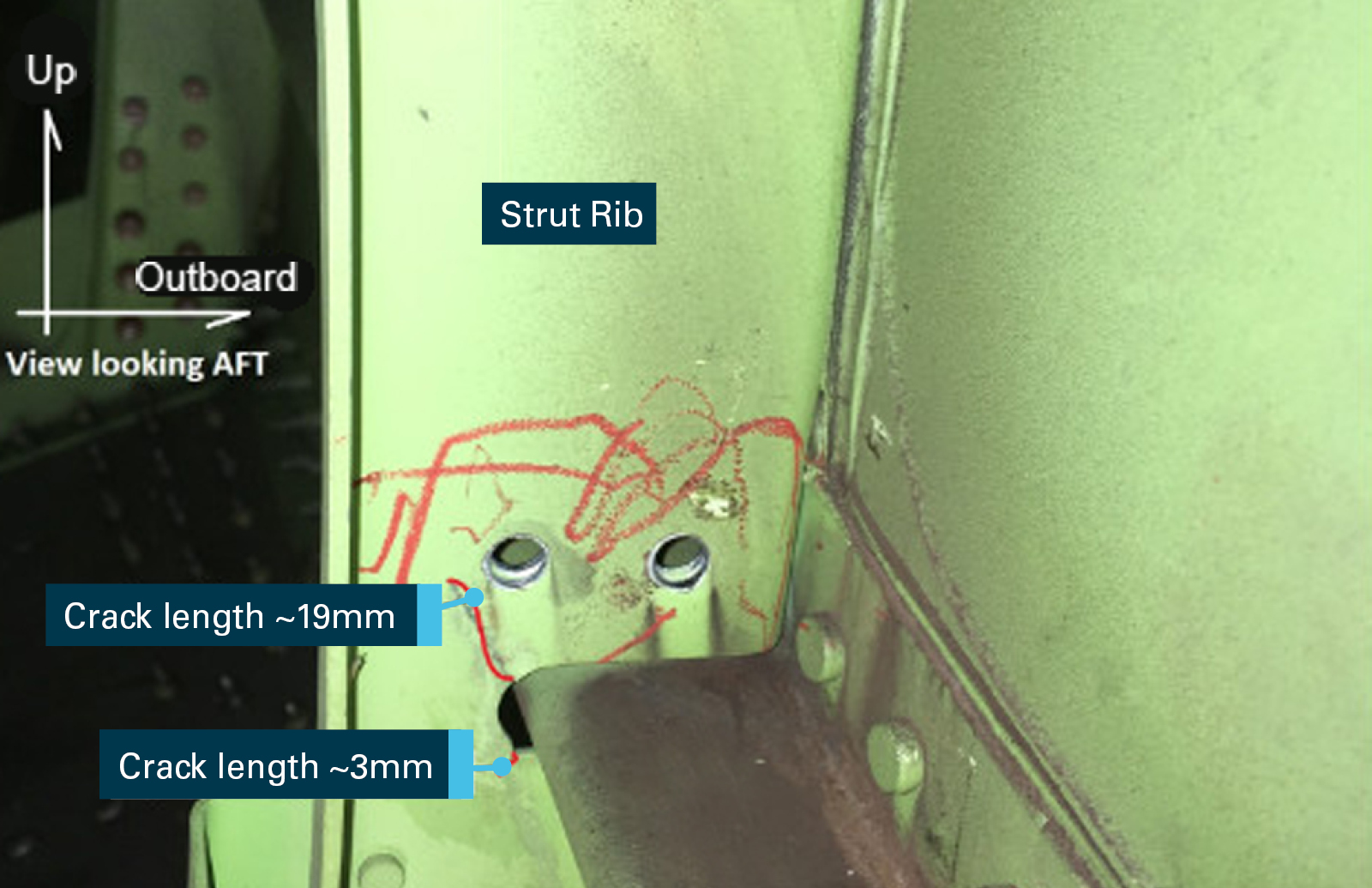
Following removal from the aircraft, four cracked outboard strut ribs were sent to Boeing for metallurgical examination and fracture analysis. The examination confirmed that five cracks had developed in the strut ribs, all emanating from the rib cutaway region, ranging in length from 3—19 mm (Figure 3 to Figure 5). Boeing’s report[3] contained the following detail:
Optical examination of the fracture surfaces was conducted and no anomalies were found that might otherwise have contributed to the development of the cracking.
Scanning electron microscopy (SEM) of the fracture surfaces did not find any aberrations or defects on the surfaces of the strut ribs that might have otherwise contributed to the development of the cracking.
SEM analysis of the fracture surfaces confirmed that each strut rib had striations and crack-progression marks consistent with fatigue cracking. No evidence was found of ductile tearing or plastic deformation at the crack origins, which might otherwise suggest that the fatigue cracking had initiated due to excessive vibration or torque loads from a transient engine event.
Metallographic examination of the aluminium alloy microstructure from each rib did not reveal any abnormalities that could have led to the fracture of the strut ribs.
Chemical analysis of each strut rib found the composition met the materials specifications, as listed within the engineering drawings.
Hardness and conductivity measurements from each strut rib confirmed that they were within the correct range, as listed within the engineering drawings.
The ribs were painted and primed in accordance with manufacturing specifications.
Boeing also conducted a structural loads analysis on the pylon, which confirmed that despite the presence of the cracking, the No. 2 engine pylon retained sufficient residual strength for all certified loading conditions.
Figure 3: A strut rib in-situ within the No. 2 pylon with two cracks identified
Source: Boeing, annotated by the ATSB
Figure 4: The strut rib from Figure 3 after removal from the pylon
Source: Boeing, annotated by the ATSB
Figure 5: Close-up of the cracking in the cutaway region shown at Figure 4
Source: Boeing, annotated by the ATSB
Aircraft history
On 24 June 2016, a few months before the detection of the pylon cracks, VH-OJT sustained a failure of the low-pressure turbine from the No. 2 engine during the take-off roll. This resulted in a high-speed seizure of the engine resulting in significant vibration and torque loads on the pylon. Following removal of that engine, the pylon was inspected and no damage to the critical structural members was evident.
Maintenance records noted that when the cracks were discovered in the Hong Kong SAR, the aircraft had accumulated 79,928 hours and 8,313 landings. There were no other identified defects reported from previous inspections on the No. 2 strut support assembly for VH-OJT.
Safety analysis
Cracking of the engine pylon strut ribs
During routine maintenance on 5 October 2016, four strut ribs from the No. 2 engine pylon were found to have developed fatigue cracks. The parts met the manufacturer’s engineering drawing and material specifications. With no obvious defects detected, it is likely that the fatigue cracking developed from exposure to vibratory loading that occurred within the pylon during normal engine operation. A factor that may have contributed to the crack growth was the number of hours and flight cycles that the airframe had accumulated within its service life. The manufacturer’s analysis indicated that despite the crack damage to the ribs, the pylon retained sufficient residual strength for all load cases, which indicates that the aircraft remained safe to operate.
Approximately 6 months prior to the detection of the strut rib cracking, the No. 2 engine sustained a seizure that resulted in the transmission of significant vibratory and torque loads into the pylon structure. Metallurgical analysis of the fracture at the crack origins did not show any evidence of plastic deformation or tearing of the alloy that might otherwise suggest that the seizure was a contributing factor to the cracking.
Pylon inspection
When compared with the 48-month inspection interval recommended by the manufacturer, the 24‑month inspection interval set by Qantas provided greater opportunity for the timely detection of cracking and other defects within the pylon. The reduced inspection interval proved effective in this case, detecting cracks before they reached a level considered by the manufacturer to be a safety risk.
Findings
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
The fatigue cracking in four outboard strut ribs in the No. 2 engine pylon is likely to have developed from exposure to vibratory loading within the pylon during normal engine operation over the aircraft’s service life.
The extent of fatigue cracking in the ribs did not affect the structural integrity of the pylon for all certified load cases, which meant that the aircraft’s safe operation was not affected.
Safety message
The Qantas Boeing 747 maintenance program for the engine pylon area is completed at a higher frequency and in more detail than is required by Boeing. This enhanced inspection regime was effective in detecting cracking of the strut rib assembly, before the cracks reached a level considered to be a safety risk.
This occurrence highlights the importance for vigilance during ongoing routine maintenance activities. It also highlights that, when relevant, operators should consider reviewing prescribed maintenance schedules in order to address issues that may develop as their aircraft age and accumulate time in service.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
The aim of the flight was to provide air experience (gliding) for a military pilot. During a loop, the instructor heard small noises but saw nothing amiss. On completion of the loop, the instructor observed a ripple on the top surface of the starboard wing and advised the other pilot to return to land. Subsequent inspection revealed a compression fracture on the top surface of the starboard wing.
On 12 September 2011 at about 1000, the pilot of a Cessna 210N aircraft, registered VH-JHF, was conducting low-level aerial survey operations near Bourke Aerodrome, New South Wales. After encountering a brief turbulence event, the pilot had difficulty in making elevator control inputs and in maintaining height. The aircraft subsequently landed safely. There were no injuries.
What the ATSB found
The ATSB found that the reported elevator control input difficulties resulted directly from the fracture of the aircraft’s two horizontal stabiliser rear attachment brackets. The forward spar of the horizontal stabiliser was also extensively cracked. The fractures and cracking were all consistent with metal fatigue and, as such, were typical of the damage sustained by aircraft as they age and move beyond the manufacturer’s originally intended design life. Many manufacturers have addressed the growing potential for this type of damage by introducing supplemental inspections to the principal aircraft maintenance requirements.
The Australian Civil Aviation Regulations 1988 (CAR) were being misinterpreted by some class B aircraft registration holders, to the extent that they believed that their aircraft was exempt from the manufacturer’s supplemental inspections when their aircraft was maintained using the CASA maintenance schedule. While the CASA maintenance schedule did not make any specific reference to the incorporation of the manufacturer’s supplemental inspections, it was a CAR requirement that all aircraft be maintained in accordance with approved maintenance data that, by definition, included those inspections.
What's been done as a result
As a result of this occurrence, on 19 September 2011 the Civil Aviation Safety Authority (CASA) issued Airworthiness Bulletin AWB 55-001 issue 2; highlighting the failure of horizontal stabilisers on Cessna 200 series aircraft. The AWB made recommendations on the maintenance schedule and inspection of the stabiliser in order to ensure the structural integrity of the area.
CASA also published a series of Discussion Papers in December 2012, detailing a range of options for developing updated continuing airworthiness regulations for all aircraft not used in regular public transport operations. This included options for reform of maintenance program requirements for non-RPT aircraft – to bring the regulations up to date with modern technology and current international standards and practice.
The outcomes from the discussion papers were unresolved at the time of writing and therefore the Australian Transport Safety Bureau has recommended that CASA proceed with its program of regulatory reform to ensure that all aircraft involved in general aviation operations are maintained using the most appropriate maintenance schedule for the aircraft type, and to also ensure that the provisions of CAR Schedule 5 are clarified in relation to the incorporation of all relevant supplemental inspections specified for the aircraft type.
Safety message
This occurrence highlights the importance of comprehensive, periodic maintenance inspections and the role of supplemental inspections in maintaining ageing airframes. The ATSB strongly encourages registration holders of class B aircraft to review their aircraft’s maintenance schedule to determine if it is the most appropriate for their aircraft and to ensure that it adequately provides for the continuing airworthiness of the aircraft.
VH-EBQ departed Cairns for Narita at 1202 local time. At 1221, a 'PAN' call (urgency message) was made, and the pilot requested an Air Traffic Control (ATC) clearance to return to Cairns. The captain stated that as the aircraft was climbing through Flight Level (FL) 200, moderate airframe vibration was felt. Checks revealed no abnormal cockpit indications. The second officer carried out a visual inspection from the cabin and noticed a damaged wing panel on the upper inboard trailing edge of the right-hand wing.
A return to Cairns was initiated and a clearance to dump fuel was obtained. Cairns ATC advised the aircraft that they had diverted an Australian Airlines Boeing 737 (B737) to escort the aircraft during the return to Cairns. A fuel dump of approximately 25,000 kg was carried out, followed by a descent and circling approach to runway 33. The captain stated that with the flaps extended, there was a slight tendency for the aircraft to roll to the right. The aircraft was landed at 1259 without further incident.
The escorting B737 landed approximately 5 min ahead of VH-EBQ. A readout of the digital flight data recorder was made to determine the data recorded on climb and during the subsequent landing at Cairns. Examination of this data showed that acceleration traces had minor inconsistencies or scatter as the aircraft was climbing through a recorded pressure altitude of FL 205 from 1214 07 to 1214 13. It is possible that the wing panel failure occurred at this time. No other anomalies were observed in the recorded data to indicate that the loss of a wing panel had occurred.
Data recorded during the landing at Cairns was consistent with a crosswind landing and no evidence of airframe vibration or other anomalies was observed in the recorded data. The failure of the right-hand inboard trailing edge fibre reinforced plastic panel was accompanied by the loss of a 2.7 m by 18 cm section of the fore flap trailing edge, and some damage to the mid-flap. The operator had previously had some 20 incidents involving this panel on Boeing 747 aircraft.
On 19 January 1991, the same panel failed on VH-EBP in flight between Sydney and Narita. The manufacturer indicated that there had been several incidents in the previous 18 months resulting from cracking, delamination and separation of this panel.
The possible related causes for failure of the panel were
(a) Damage caused by personnel stepping on the panel.
(b) Damage caused by tyre burst.
(c) Manufacturing anomalies.
(d) Misrigging. (The panel is an aerodynamic surface and is fixed in position with screw jacks to preload it with flaps retracted.)
The panel is subject to a coin 'tap test' to check for delamination, and a push test on both upper and lower surfaces at each 'A' check (400 hrs). VH-EBQ was last inspected on 8 December 1990. When the trailing edge flaps are fully retracted and the fuel tanks are full, the trailing edge of the fixed panel is deflected upwards by as much as 4.5 cm by contact with the flaps. The operator has re-rigged the trailing edge panels so that the maximum deflection is 3.5 cm, thus reducing pre-load stress.
In addition, 'NO STEP' signs have been painted on the panels to reduce possible damage during maintenance. The failed panel from VH-EBQ was not available for examination; however, the subsequent failed panel from VH-EBP was available, and a specialist examination was carried out. Specialist opinion was that both failures were of a similar type, whereby trailing edges had peeled off as a result of debonding and bending due to pre-load rather than aerodynamic forces.
The manufacturer has incorporated design changes to overcome this type of failure. The operator has increased the frequency of periodic inspections of the panel, and it is considered that sufficient corrective action has been taken to overcome the problem. A comprehensive investigation of Air Traffic Services (ATS) aspects was carried out. The investigation concluded that the decisions and actions taken by the ATS personnel involved in the handling of the situation were prompt and effective.
The provision of an escort aircraft was justified in view of the information received initially from VH-EBQ and is consistent with the relevant operational practices and techniques documented in the Airways Operations Instructions (AOI). The captain of VH-EBQ initially felt some concern about the provision of an escort aircraft because of a lack of a clear understanding as to the function of the escort aircraft in relationship to his aircraft.
Selection of the aircraft to perform the intercept/escort was in accordance with published AOI guidelines, and implementation of the escort action was efficient and effective. Consideration of weather conditions was not included as a factor in determining the provision of an escort aircraft in the current AOI.
On arrival at Sydney, the helicopter landed near the helipad and ground- taxied to the concrete apron in the general aviation parking area. The pilot intended to park in a confined space, adjacent to buildings and hangars on the north-eastern extremity of the apron. A number of aircraft were parked in close proximity to the west and south of the intended parking position. A grassed area to the east was free of obstacles. Ground marshalling assistance was not available. The surface wind was from the south-east at 10-15 kts.
The helicopter taxied to the intended parking position and stopped on an easterly heading. Witness evidence concerning the events which followed was not consistent. The pilot reported sensing a rocking motion which he interpreted as the onset of ground resonance. The helicopter was lifted off and turned towards the building. During this manoeuvre, an extreme vibration commenced which caused the pilot to experience a loss of vision and led to a loss of control of the helicopter. The passenger later recalled that the helicopter completed a 180 degree turn on the ground onto a westerly heading before the rocking motion was felt and the pilot lifted the helicopter off the ground. A ground witness seated inside the building observed the helicopter come to a halt on an easterly heading. It then became airborne and completed a hover turn left onto a westerly heading, at a height of approximately 8-10 feet. As the helicopter settled momentarily, it appeared to be rocking slightly and touched down on each wheel individually, suggesting the pilot was experiencing minor control difficulties.
The helicopter became airborne a second time and was observed to turn right onto a northerly heading, facing a building adjacent to the apron. Severe pitching oscillations commenced as the helicopter climbed to a height of about 30 ft. After several oscillations, the helicopter yawed and rolled to the left, travelling in a westerly direction towards a parked Learjet. The angle of bank increased to 90 degrees and the nose began to drop at about the time the main rotor blades struck the tailplane of the Learjet and the concrete apron. Debris was scattered over a wide area. The fuselage was propelled forward such that the nose of the helicopter collided with the closed doors of a hangar. The helicopter then impacted heavily with the apron on its left side. The tail boom separated and the extensively damaged fuselage came to rest lying on its left side, with the left engine continuing to run.
An extensive technical investigation, which was hampered by the degree of impact damage, did not reveal any evidence of a pre-existing mechanical fault or defect. The investigation was unable to positively establish the reasons for the oscillations reported by the pilot as being the onset of ground resonance, or the source of the extreme vibration which caused the pilot to lose vision and control of the helicopter. However, it was noted that the helicopter was operated in close proximity to a building in wind conditions which favoured recirculation of airflow through the main rotor disc. A possible source of vibration was the interaction of main rotor downwash and the tail rotor . It was also noted that the helicopter was taxied into a confined area where the manoeuvring options available to the pilot were limited.
SIGNIFICANT FACTORS
The following factors were considered relevant to the development of the accident:
1. The helicopter was ground-taxied to a parking position which was in close proximity to buildings and hangars.
2. The parking position and the wind conditions were conducive to the onset of main rotor recirculation.
3. The pilot reported the suspected onset of ground resonance.
4. During an attempt to recover from suspected ground resonance, an extreme vibration developed which led to the loss of control of the helicopter.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation.
What happened
On 19 January 2020, a Boeing 737-800 departed Brisbane, Queensland for a commercial passenger flight to Melbourne, Victoria. There were 6 crew and 178 passengers on board.
Passing FL 250 on climb near Gold Coast Airport, Queensland, a cabin crew member advised the flight crew that a passenger alerted them to a panel hanging off the rear of the aircraft’s left wing. The flight crew requested that the cabin crew further investigate, and discontinued the climb and levelled off at FL 300.
The cabin crew subsequently showed pictures to the flight crew of the dislodged panel on the trailing edge flap area of the left wing. The crew then contacted air traffic control and requested a clearance to descend and return to Brisbane. The aircraft landed without incident and taxied to the gate.
Engineering inspection
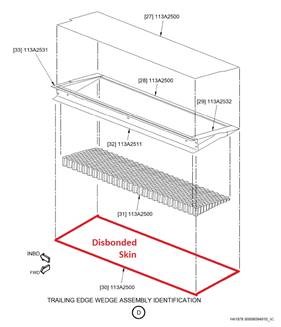
Following the incident, the engineering inspection revealed that the inboard trailing edge flap on the left wing had delaminated (Figure 1). The engineers determined that the delamination was due to moisture ingress and excess heat from the engine exhaust.
Figure 1: Delaminated section on the aircraft’s left wing
Source: Operator’s engineering department
Figure 2: Diagram of trailing edge assembly
Source: Operator’s engineering department
Safety action
As a result of this incident, the manufacturer and operator have advised the ATSB that they are taking the following ongoing safety actions:
Manufacturer
Boeing will be supplying a modified metallic assembly to be installed on aircraft.
Operator
The operator conducted a fleet inspection of its aircraft aged 10 years old or older and found 7 other aircraft had delamination findings recorded. Due to delamination findings, the inspection program was expanded to flaps on aircraft 6 years old or older, to identify potential early defects on younger aircraft.
A full damage analysis of the completed inspections and expanded program will support the determination of an effective threshold interval for introducing scheduled inspections via a new aircraft maintenance program task.
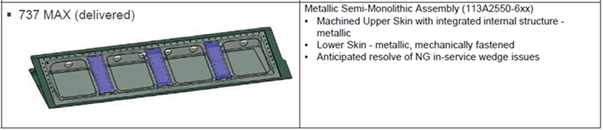
Introduction of a modification program to replace the composite bonded assembly wedge with a new design metallic semi-monolithic assembly (Figure 3).
Figure 3: Diagram of new metallic semi-monolithic assembly for trailing edge flap
Source: Operator’s engineering department
Safety message
This incident provides a reminder that although flight crews conduct extensive pre-flight inspections, unexpected failures may still occur in flight. In this situation, the flight crew took all possible precautions by following the relevant procedures, conducting additional checks to assess the situation, providing clear communications to ATC and returning the aircraft to land.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.