Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 4 August 2025, an amateur-built Lancair IV departed Orange Airport, New South Wales, at 0652 local time, intending to fly to Bankstown Airport.
During cruise, the aircraft sustained an electrical system failure, resulting in numerous electrically driven systems failing. The pilot then made the decision to conduct an air return to Orange Airport, rather than continue the flight towards Bankstown.
Orange Airport consists of primary runway 11/29 which is 2,213 m long and is a sealed surface with a secondary runway 04/22 which is a 964 m long unsealed surface.
Due to the electrical malfunction, several systems of the aircraft were impacted, including the landing gear and VHF radio communication systems. The pilot used their mobile phone to communicate with a ground station to aid in facilitating their arrival at Orange Airport.
As the landing gear system is electrically controlled and hydraulically operated, due to the electrical failure, the primary method of the gear extension was not functional.
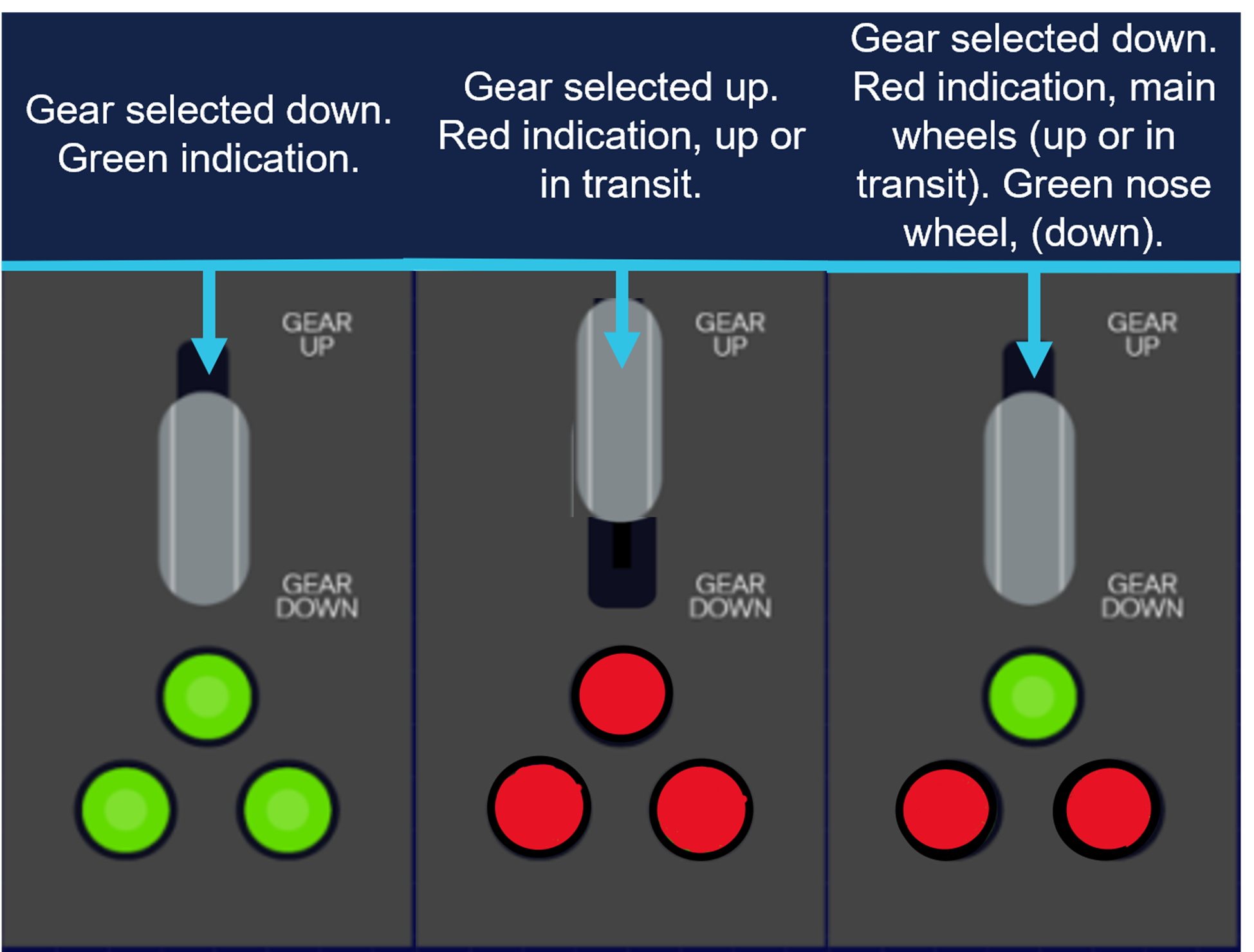
During the initial approach to the primary runway, the pilot manually selected the landing gear ‘down’ to extend the landing gear. Once manually selected ‘down’, the undercarriage extension indicator showed that only the nose gear had locked ‘down’, indicating (green), with the main gear, not indicating that it had ‘locked’ down (Figure 1).
Figure 1: Generic representation of landing gear selection
Source: ATSB representation of landing gear selection and indication. May not be indicative to type of aircraft.
The pilot proceeded to conduct several low passes of the runway to try to ascertain the condition of the landing gear with people on the ground.
However, after not being able to confirm the gear was fully down and locked, the pilot then made the decision to conduct a precautionary landing on the non-sealed cross strip, runway 04.
The pilot conducted the approach and landed, however on touchdown the main undercarriage legs collapsed, and the aircraft slid on the nosewheel (front of the aircraft) and rudder (rear of the aircraft) before coming to rest at the fence at the end of the runway.
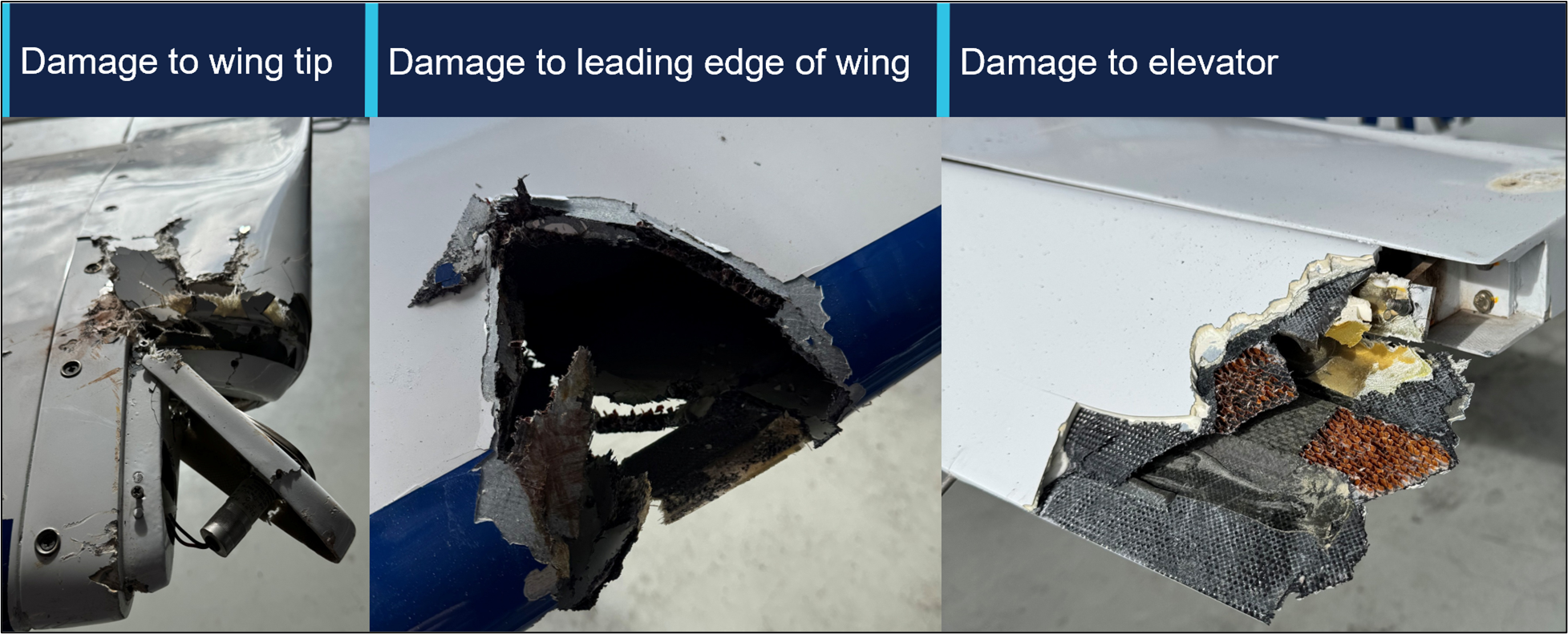
The aircraft incurred some minor damage (Figure 2) to the wingtip and elevator with no injuries to the pilot.
Figure 2: Damage to aircraft
Source: Operator, annotated by the ATSB
Subsequent engineering inspections found the electrical system had failed due to a defective voltage regulator.
Safety message
This occurrence illustrates that a good knowledge of aircraft systems coupled with sound decision‑making can help facilitate a positive outcome to an emergency.
Aircraft rely on hydraulic or electrical systems to extend and retract the landing gear. Should any component in these systems fail, pilots may be left with no choice but to manually extend the undercarriage or potentially execute a wheels-up landing.
Applying a structured and proactive approach to identifying and managing threats and errors, influences the safety of the flight.
In this instance, the pilot was able to identify the aircraft system failure and make several calculated risk-based decisions to manage the emergency. This was achieved by using various resources at their disposal, such as their mobile phone, to seek ground assistance in the absence of normal VHF radio.
In emergency situations, pilots need to utilise all the available resources at their disposal. Maintaining a degree of flexibility and adapting to select the most appropriate landing area can minimise risk, limit damage and maximise survivability.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-039
Occurrence date
04/08/2025
Location
Orange Airport
State
New South Wales
Aviation occurrence category
Collision with terrain, Diversion/return, Electrical system, Landing gear/indication, Runway excursion, Wheels up landing
On 28 August 2025, a pilot and a passenger in a Piper Aircraft PA-28 were participating in the Outback Air Race from Daly Waters Airport to Royal Australian Air Force Base Tindal, Northern Territory. After the engine was started, the pilot detected a tripped circuit breaker and requested that a maintainer attend the aircraft to assess the fault. The maintainer found that the alternator was unserviceable and charged the battery to allow the aircraft to fly to Tindal where further maintenance could be conducted.
En route to Tindal, the aircraft lost electrical power and the pilot was unable to communicate using the aircraft’s radio. The aircraft was subsequently climbed into restricted airspace without clearance and continued to the airport while the pilot and passenger communicated with fellow race participants on a mobile phone group chat application.
At the same time, a formation of 2 Lockheed Martin F-35 aircraft was returning to Tindal. Unaware that the PA-28 was inbound, air traffic control cleared the formation to join left base and land on the runway. While the second F-35 completed the turn to final approach, the PA-28 also joined final in close proximity. Separation between the aircraft reduced to approximately 72 m laterally and 25 ft vertically before the PA-28 subsequently landed behind the F-35.
What the ATSB found
The ATSB found that after identifying a fault with the alternator, the licensed aircraft maintenance engineer encouraged the pilot to conduct the flight without assessing the time the battery could supply the aircraft with electrical power. Additionally, they did not record the issue or maintenance activity on the aircraft’s maintenance release.
It also identified that, prior to departure, the pilot did not conduct contingency planning to prepare for a loss of electrical power in flight. In addition, during the flight the pilot did not monitor the aircraft’s electrical system. Subsequently, the aircraft lost electrical power and the pilot was unable to communicate with air traffic control via the aircraft’s radio, and the aircraft could not be detected by the surveillance systems in use.
In addition, it was found that the pilot did not divert to the closest airport or follow advice to remain outside controlled airspace, and the aircraft entered controlled airspace without the required clearance. Subsequently, the aircraft joined final approach in close proximity to an F-35 approaching the same runway.
The ATSB also found that when conducting a visual check of the F-35 formation’s approach path, the tower controller did not detect the PA-28 on approach to the runway.
Safety message
This incident highlights the importance of clear communication between maintenance personnel and pilots. Recording of defects and subsequent maintenance actions on the aircraft’s maintenance release is central to ensuring that all parties share a common understanding of identified faults, the anticipated in-flight effects and their impact on the overall airworthiness of the aircraft.
Pilots are also reminded that if the aircraft has an increased risk of an abnormal event, contingency planning and identifying potential courses of action prior to take-off can reduce workload and help to facilitate a safe outcome. In addition, following published emergency procedures in the En Route Supplement Australia will ensure that action taken aligns with air traffic control expectations. This is particularly important in situations involving interruptions to electrical power, where communication or surveillance capability is affected.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
Overview
On 28 August 2025, a pilot was participating in the Outback Air Race (OAR) (see the section titled Outback Air Race) in a Piper Aircraft Inc. PA-28-236 (PA-28) aircraft, registered VH‑TKX and using callsign ‘Air Race 9’. They planned to conduct a flight under the visual flight rules[1] from Daly Waters Airport to Royal Australian Air Force (RAAF) Base Tindal (Tindal), Northern Territory, on stage 4 of the 9-stage race, with a passenger who had been accompanying them throughout the event.
Maintenance prior to the departure
On starting the aircraft’s engine at Daly Waters Airport that morning, the pilot observed that the alternator circuit breaker had tripped. After trying unsuccessfully to reset the circuit breaker, they shut down the engine and requested assistance from the licensed aircraft maintenance engineer (LAME) that had been provided by the race organiser to assist participants with maintenance issues.
The LAME determined that the alternator was unserviceable, and that the issue could not be rectified at Daly Waters as they required space in a workshop to do the work and spare parts, which were available at Tindal. During the assessment, they identified a loose alternator attachment bolt, which they tightened. They also charged the aircraft battery. The LAME recalled that the pilot was aware that the flight would be conducted with the battery providing electrical power (see the section titled Maintenance actions).
The pilot confirmed that they were aware that the flight would be conducted with the battery providing electrical power, but when taxiing for departure, they made a final attempt at resetting the alternator’s circuit breaker, which was successful. No entry was made on the maintenance release to record that the alternator was unserviceable or that maintenance had been conducted prior to departing Daly Waters.
The OAR flight manager, who was not at the airport at the time, received a phone call from the pilot prior to the flight, to discuss the issue and the impact on their expected departure time. The flight manager recalled that the pilot told them that the alternator was not working and that the LAME had told them they would probably have sufficient battery-supplied electrical power to conduct the flight to Tindal. They further recalled that the pilot was willing to conduct the flight under these circumstances. In addition, they advised that the pilot requested to depart as soon as possible, to allow them to arrive at Tindal before the maintenance facility closed for the day.
The flight
After being repositioned in the race departure sequence, the aircraft departed Daly Waters at 1211 local time. At 1217, it flew over the ‘Gate out’, commencing the time trial. The pilot conducted the race leg, which was completed at 1257 by flying through ‘Gate in’, a position 39.5 NM (about 73 km) to the south-east of Tindal (Figure 1).
Figure 1: PA-28 track
Source: Google Earth with fight radar tracking, annotated by the ATSB
Coincident with the conduct of the race leg, a formation of 2 Lockheed Martin F-35 Lighting II (F-35) aircraft, callsign ‘Blackbird’, was conducting operations to the south‑west of Tindal. Each aircraft had a single pilot on board. At 1252, they finished their operation and were cleared by Tindal Air Traffic Control (ATC) to return to Tindal. At the time, they were advised by ATC of multiple aircraft participating in the air race, inbound to Tindal from the south-east, following the Stuart Highway at an altitude of 1,500 ft. To facilitate a faster return, the controller instructed the pilots of the F-35s to track for the left base leg of the circuit for runway 32R,[2] instead of joining for a low initial and pitch.[3]
At approximately 1302, the pilot of the PA-28 observed a series of progressive failures of the aircraft’s electrical components including:
the transponder
the radios
one of the G5 units
the GPS navigation unit
the autopilot
the GI 275 unit.
They also recalled detecting an acrid burning smell in the cockpit. No longer able to communicate through their headsets, the pilot discussed the situation with the passenger, recalling that communication was difficult due to the level of noise in the cabin. At 1304, the passenger of the PA-28 communicated with fellow race participants via a group chat[4] (using a mobile telephone application), advising that:
they had lost electrical power, and the radio had failed
they were 10 minutes away from Tindal
they might have to land at Homebush Park aircraft landing area (ALA).
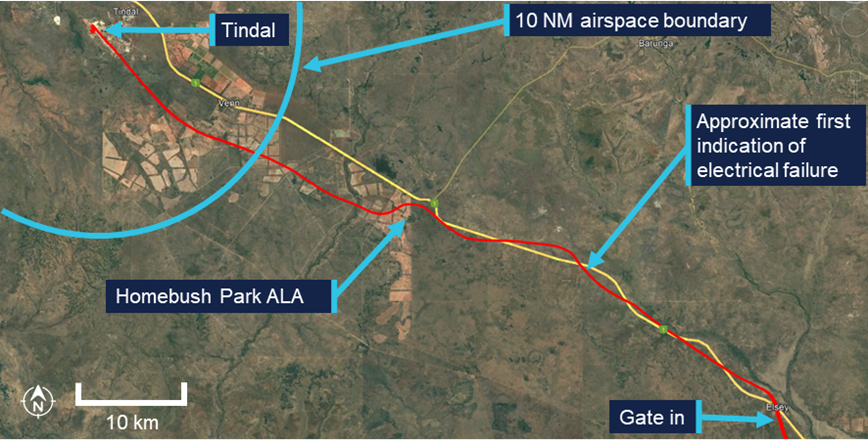
The ALA was approximately 18 NM (33 km) to the south-east of Tindal and outside controlled airspace (Figure 2). At 1306, they flew over the ALA, and asked, via the group chat, if they should land there or continue to Tindal. Having not received a response, 1 minute later they wrote in the chat that they were 7 minutes from Tindal, were heading there directly and required the ‘airways cleared’.
At around this time, the aircraft commenced a climb from 1,500 ft to 4,000 ft. The pilot stated that they commenced a climb to ensure they had additional gliding range if the engine failed, as they were unsure of the source of the burning smell. As the airspace above 1,500 ft was an active military restricted area (see the section titled Royal Australian Air Force Base Tindal), the aircraft entered controlled airspace without a clearance. The pilot later reported being aware of this, but considered that ATC was aware of their position.
Figure 2: PA-28 track (in red) from ‘Gate in’ to Tindal
Source: Google Earth with fight radar tracking, annotated by the ATSB
At 1308, multiple race participants posted the telephone number for both Tindal Approach and Tower on the group chat and advised the pilot to call Tindal ATC. The PA‑28 occupants responded stating they were unable to make a telephone call due to the noise in the cockpit. They were then advised that one of the other race participants was attempting to call Tindal ATC. The pilot later advised that their headset was not equipped with Bluetooth connectivity and, while the passenger’s headset was equipped, they had previously been unsuccessful when trying to use that functionality.
At 1310, the Tindal approach controller received a phone call from a member of the group chat advising that they were receiving messages from the occupants of an aircraft holding over Homebush Park with an electrical failure.[5] During the call, the controller advised the caller that it was unsafe for the PA-28 to land at Tindal due to the level of traffic and instructed that the aircraft land or hold at Homebush Park and, if required, the PA-28 pilot should call ATC directly. A message was posted to the group chat advising the PA-28 pilot of these instructions. The PA-28 occupants responded in the group chat that they were not landing at Homebush Park and instead were tracking direct to the runway at Tindal and were climbing to 3,500 ft.
During the phone call, the approach controller advised the F-35 pilots that one of the race participants was subject to an emergency. At this time, the F‑35s were approximately 30 NM (56 km) to the south and tracking towards the airport.
At 1311, a third, different member of the group chat also wrote that ATC had instructed the PA-28 to land at Homebush Park. However, the PA-28 pilot continued to climb and track for the runway at Tindal, responding in the group chat that it was too late and requesting runway 32.
Concurrently, the approach planner (see the section titled Royal Australian Air Force Base Tindal – Air traffic control) requested a supervisor to assist as they had 2 additional OAR participants, unrelated to the emergency, holding outside restricted airspace (see the section titled Air traffic control actions), and they were concerned that they were not maintaining separation from each other. When the supervisor entered the control room, the approach controller advised them that they had 2 F-35s returning and that they had received a phone call about an aircraft with an emergency and, other than they were holding over Homebush Park ALA to diagnose an electrical fault, they had few details.
At 1312, the member of the group chat who had called the approach controller 2 minutes earlier, called again and on this occasion, the approach supervisor answered the call. This call lasted 6 minutes during which the caller advised that the PA-28 was 3 minutes from the threshold, they were coming into land, and they could see the runway.
The approach supervisor advised that it took them time to establish that the caller was not in the PA-28 and was relaying information from the group chat. It was also initially unclear that the caller was simultaneously relaying information to somebody else who was entering the information into the group chat. During the call, the supervisor recalled passing information that the 2 F-35s were on approach and also instructed that the PA‑28 remain outside controlled airspace. The supervisor was still on the telephone with the caller and was standing behind the approach controller advising that there was an inbound aircraft, when the near collision occurred.
Also at 1312, a different member of the group chat posted a question to the PA-28 occupants asking if they wanted them to declare a PAN (see the section titled In-flight emergencies), to which the PA-28 responded that they did. The pilot later advised that as they considered that a PAN had been declared on their behalf, they thought that other traffic would be cleared from their planned flight path. They further advised that they had access to their tablet device running the AvPlan electronic flight bag (EFB). This showed the 2 air race participants holding outside controlled airspace, which they incorrectly assumed meant that ATC were holding them to clear the airspace for the PA-28 to continue. None of the air traffic controllers recalled a PAN being declared on behalf of the PA-28.
At 1313, the F-35 formation leader called the tower controller on the radio at 5 NM (9 km) (Figure 3 and Table 1). One minute later, after visually checking the base and final legs of the circuit and not sighting the PA-28, the tower controller cleared the formation to land. At this time a member of the group chat wrote in the chat that there was an F-35 on a 3 NM (6 km) final, likely relaying traffic information given by the approach supervisor during the telephone call.
Also at this time, an additional phone call was made by the OAR flight manager to the tower, which was answered by the tower supervisor. The flight manager advised the tower supervisor that a PA-28 had experienced an electrical failure somewhere between Daly Waters and Tindal and may have had issues. The tower supervisor was on the phone with the caller when the near collision occurred.
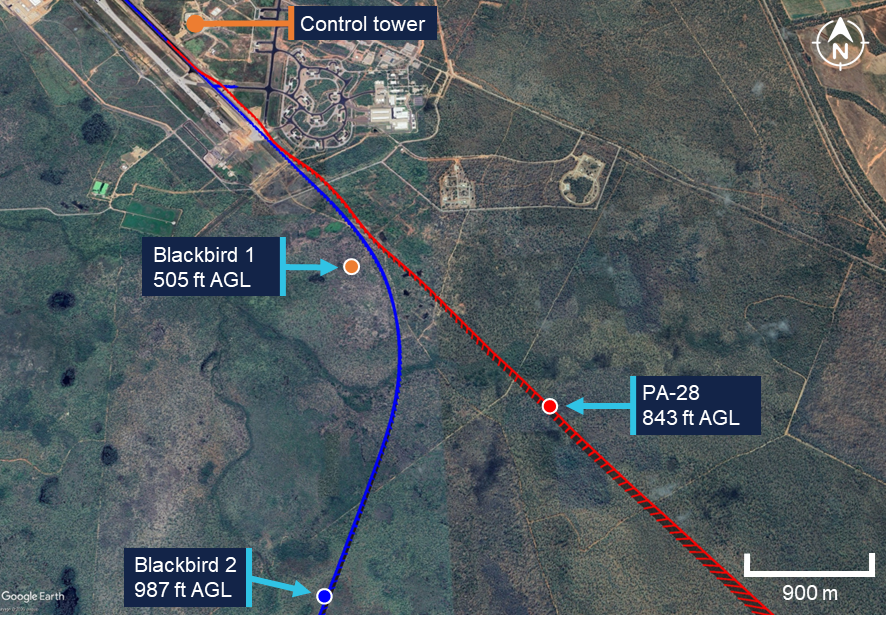
Figure 3: Aircraft tracks with events
The red track is the PA-28 inbound from Homebush Park ALA, the blue track is the track of both F-35 aircraft tracking in company. Source: Google Earth with fight radar tracking, annotated by the ATSB
Table 1: Key events
Time
Description
A
1307:40
PA-28 commenced climb above 1,500 ft
B
1310:00
PA-28 told to expect landing at Homebush Park via group chat
C
1311:00
PA-28 directed again to land at Homebush Park via group chat
D
1311:36
PA-28 peak of climb 3,910 ft
E
1312:00
PA-28 occupants asked if they wanted to declare a PAN via group chat
F
1312:16
Approach received a 6-minute-long phone call advising location of the PA-28
G
1313:24
Blackbird (F-35) formation called tower controller at 5 NM
H
1314:19
Tower controller cleared Blackbird formation to land
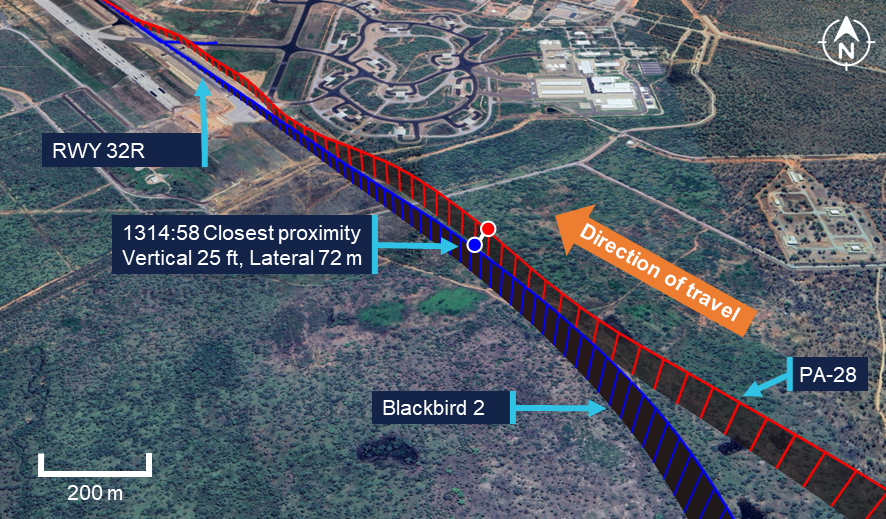
As the PA-28 joined final approach, its pilot observed the 2 F‑35s joining the circuit from their left. The first F-35 (Blackbird 1) joined final in front of the PA‑28, while the second F‑35 (Blackbird 2) turned and joined final at approximately the same location as the PA‑28 (Figure 4). Flight data showed that separation between the PA‑28 and the second F‑35 reduced to approximately 72 m laterally and 25 ft vertically. The PA‑28 pilot then manoeuvred their aircraft to the right to increase separation, while continuing towards the runway.
The PA-28 pilot advised that they assumed that the F-35 pilots would have been informed of their emergency and would maintain separation. They also assumed that the PA-28 had priority due to the PAN declaration.
Figure 4: Tracks of PA-28 and F-35
Source: Google Earth with recorded fight data, annotated by the ATSB
The pilot of Blackbird 2 recalled seeing the PA-28 over their right wing tip as they completed their turn onto final. They notified the tower controller of an aircraft on short final and continued to land. In response, the tower controller instructed the PA-28 to go around immediately. However, due to the aircraft’s electrical failure, the PA-28 pilot did not receive the instruction and continued to land behind Blackbird 2. The PA-28 pilot advised they landed on the right edge of the runway to avoid the wake turbulence from the F-35.
The following day, the alternator on the PA-28 was replaced at Tindal and the pilot and passenger continued with the race. The maintenance organisation at Tindal determined that the alternator failed due to an internal electrical defect.
Context
Pilot information
The pilot of the PA-28 held a Commercial Pilot Licence (Aeroplane) and instrument rating and had a class 1 aviation medical certificate. They had a total of 365 hours flying experience, of which 250 were on the PA-28. They had flown 24 hours in the previous 90 days.
Both F-35 pilots fully met the RAAF requirements to operate the aircraft.
Aircraft information
VH-TKX was a Piper Aircraft PA-28-236, a 4-seat, low-wing, fixed-undercarriage aircraft with a piston engine. The aircraft was manufactured in 1978 and first registered in Australia in 1983. It was equipped with an upgraded Garmin GI 275 electronic flight instrument as the engine indicating system and 2 Garmin G5 electronic flight instruments providing an attitude indicator and horizontal situation indicator. The GI 275 did not have backup power. The G5s each had a backup battery designed to power the unit for 4 hours independently of the aircraft’s electrical system. The aircraft maintainer advised that the display of the G5 could be affected during a loss of electrical power due to associated interruptions to input data signals.
The aircraft was maintained in accordance with schedule 5 of the Civil Aviation Regulations 1988, which required a periodic inspection every 100 flight hours or 12 months, whichever came first. The last periodic inspection was conducted on 30 June 2025, and there were no outstanding items recorded on the aircraft’s maintenance release. At the time of the incident, the aircraft had accumulated 4,181 hours total time in service.
Pilot operating handbook
The pilot operating handbook (POH) stated that the required actions following an electrical failure were to:
select the alternator switch to OFF
minimise the electrical load
land as soon as practical.
It also stated that when the alternator failed the battery would supply the electrical load, but did not state how long this would last.
The POH also stated that if smoke or fumes were detected in the cabin, this indicated an electrical fire, which required that the master switch, cabin heat and defroster be selected to OFF and air vents be opened to clear smoke and fumes from the cabin. It also required that the aircraft land as soon as practicable.
Maintenance actions
The LAME advised that when they assessed that the alternator was unserviceable, they sought to get the aircraft to a workshop at Tindal for repair. They made an assessment, without checking the electrical load requirements (and therefore the likely usable time of battery power), that the aircraft, having no retractable gear or electric flaps, and modern avionics equipment which did not use much power, would likely be able to complete the planned flight with only the battery providing the required electrical power. They recalled communicating this assessment to the pilot but did not recall whether they specifically stated that the alternator was unserviceable.
The LAME reported that they charged the battery as a contingency. They also advised that they considered their role was to advise a pilot what the problem was and that it was the responsibility of the pilot to make the decision as to whether to conduct the flight. However, while they reported that they didn’t want to get involved in operational decision‑making, they felt that they encouraged the pilot to conduct the flight.
In hindsight, they also identified a number of measures that could have been discussed with the pilot to mitigate the risk of an in-flight electrical failure. These included waiting until the military-controlled airspace was de-active and providing an escort aircraft.
Outback Air Race
The 2025 Outback Air Race (OAR) was a fundraising event for the Royal Flying Doctor Service with approximately 40 aircraft participating in the 9-stage time trial across outback Australia. The race was conducted between 24 August 2025 and 7 September 2025 commencing at Yulara, Northern Territory, flying via:
Alice Springs
Tennant Creek
Daly Waters
Katherine (Tindal)
Kununurra
Broome
Onslow
Exmouth
and finishing at Carnarvon, Western Australia.
In the lead up to the event, race participants were provided with briefings on items including race rules and airspace requirements, as well as being provided with a guide for how to conduct the race. Additionally, a supplement to the guide was provided which described the features of each stage of the race, and the airspace requirements, including radio call examples unique to each stage. In addition, a brief was conducted each morning for all race participants to clarify any queries. Noting the race’s remote nature, the OAR organisers also provided a LAME and designated aviation medical examiner to assist during the event.
The concept was a time trial event with the time commencing at a predetermined ground feature, referred to as ‘Gate out’ and ending with a ground feature some way from the destination airport, referred to as ‘Gate in’. This allowed pilots to pay full attention to departure and landing procedures without the pressures of the race construct. To assist with maintaining aircraft separation during the race, the OAR had sequenced aircraft to depart based on their relative speed.
As the stage from Daly Waters to Tindal was due to enter military airspace, the race organisers liaised with Tindal ATC and 75 Squadron[6] to facilitate arrivals and departures, ideally deconflicting with the F-35 operating windows as much as possible. A coded clearance, ‘Route Outback’ was developed to simplify the airways clearance into Tindal, which required the aircraft to track 1 NM (2 km) to the north of the Stuart Highway at 1,500 ft.
ATC liaised with the OAR flight manager, Tindal Base Aviation Safety Officer and 75 Squadron to coordinate flights arriving at Tindal on the day. It was agreed that during the F-35 operating windows, OAR aircraft would arrive with 15-minute spacing and outside the F-35 operating windows the aircraft would arrive with 5-minute spacing. The F-35 operating windows were scheduled for 0945–1300 and 1430–1645 local time.
Royal Australian Air Force Base Tindal
General information
Tindal was a joint military and civilian user airport operated by the RAAF. The airport had one runway, 14/32. At the time of the incident, the runway was closed due to works and the parallel taxiway ‘A’ was being used as a runway, designated 14L/32R.
When the tower at Tindal was active, the area within 10 NM (19 km) of the airport became controlled airspace, requiring a clearance from ATC to enter. Sectors of restricted airspace also became active during tower hours. When active, this airspace also required a clearance to enter and included:
between 10–20 NM (19–37 km) from the airport above 1,500 ft
between 20–30 NM (37–56 km) from the airport above 2,500 ft.
Outside of tower hours, the airport operated as a non-controlled airport and the restricted airspace was not active.
The structure of Tindal airspace was published by Airservices Australia in the Tindal Visual Navigation Chart (Figure 5). Additional information about operating at Tindal was published in the En Route Supplement Australia (ERSA), including 2 phone numbers for ATC enquiries.
Figure 5: Tindal airspace during tower hours
Source: Airservices Australia, annotated by the ATSB
Air traffic control
At the time of the occurrence, Tindal air traffic control was comprised of 5 positions. Approach consisted of an approach controller, an approach supervisor and an approach planner. In the control tower were a tower controller and a tower supervisor with a dedicated communications line to the approach controllers. Only the controllers in the control tower had visibility of the airport and runway. All controllers were members of the RAAF, had a current proficiency check and each had experience operating at Tindal for at least 12 months.
Tindal ATC utilised a combination of primary surveillance radar (PSR), secondary surveillance radar (SSR) and air ground air (AGA) communication systems. On the day of the incident, the PSR was not available.
Both approach and tower controllers had access to tablet devices with the OzRunways electronic flight bag (EFB) installed. These displayed aircraft as traffic when a pilot was using the same software on a device in the aircraft and it was configured to broadcast the aircraft’s position.
The controllers advised that during the morning the air race aircraft were arriving with about 10–15-minute spacing, however the aircraft had not been adhering to the standard clearance, with some aircraft operating above the agreed altitude when they were outside controlled airspace. In addition, as agreed with the race managers, there were no flight plans submitted, and ATC had preprepared flight strips ready for each inbound aircraft.
Previous emergency
Earlier the same day, another air race aircraft experienced an alternator failure also resulting in an electrical failure. The pilot of this aircraft called Tindal ATC directly using their mobile phone, advising them of their emergency, and received a clearance to enter controlled airspace and land at Tindal.
Air traffic control actions
Approach
The approach controller advised that during the F-35 morning operating window, the longer spacing between the arriving air race aircraft enabled them to be held at the control zone boundary without creating a proximity hazard with other participating aircraft. When the OAR aircraft arrived earlier with a similar electrical emergency, the controllers had held the final formation of F-35s (the incident formation) on the ground until the aircraft landed. This delay resulted in this formation returning to the airport about 15 minutes after the agreed operating window had passed, and spacing between the air race aircraft had reduced. The controllers advised that they observed a string of aircraft on the SSR coming along the Stuart Highway. Additionally, the pilot of the occurrence PA-28 advised they were using a 3-minute separation rather than the agreed 5-minute separation.
The approach controller also advised that normally when the F-35s returned to base they returned with minimal fuel. Therefore, when the F-35 formation advised they were inbound, the controller decided to expedite their return while there were not many other aircraft in the area.
At that stage, one race aircraft was already cleared for a visual approach, and they were in the process of transferring responsibility for this aircraft to the tower controller. They instructed the next 2 OAR aircraft to hold outside controlled airspace. They were then contacted by an inbound helicopter, which they also advised to remain outside controlled airspace. At the same time, the approach planner observed that separation between the 2 OAR aircraft holding outside controlled airspace was reducing and they were coordinating with the approach controller to obtain a clearance for one aircraft to climb into controlled airspace to create vertical separation.
The first phone call from an OAR participant about the emergency aircraft was taken by the approach controller. They recalled that earlier in the day, another of the air race aircraft had also experienced a complete electrical failure, and they were initially unsure if this was the emergency from earlier misread in the group chat or if it was a new emergency (see the section titled Previous emergency). After requesting that the aircraft hold or land at Homebush Park, they concluded the call.
Subsequently, they contacted the tower controller via the internal line to discuss bringing the F-35s in quickly to facilitate the approach of an emergency aircraft with a possible electrical issue.
The approach supervisor had been on a break when the planner requested that they return to duty and, just after they entered the room, they answered an incoming telephone call. At that stage, they had just received a quick briefing from the approach controller, using the SSR screen to gain situational awareness of the traffic and had been advised of the aircraft with an emergency.
They recalled that it took some time to determine that the caller was not in the aircraft but was on the ground reading group chat messages. During the conversation they were told that the emergency aircraft was 3 minutes from the threshold and had the runway in sight, but could not recall how far through the call this information was received. Additionally, they recalled passing information about the F-35s on approach, and advised the caller that the emergency aircraft should remain outside controlled airspace. It was during this call they heard on the tower frequency that the near collision had occurred.
Tower
The tower supervisor had taken the telephone call from the OAR flight manager and was trying to ascertain information about the PA-28 to provide to the tower controller. Both the tower supervisor and controller were looking on the radar screen for a return to identify the aircraft’s position. In addition, the tower controller looked at the OzRunways EFB for traffic but did not identify any within the control zone. The tower supervisor advised that, while normally their duties included periodically visually scanning for other aircraft with binoculars, they were unable to do so during the phone call. In addition, they advised that sighting small aircraft such as a PA-28 was difficult when their exact position was not known.
At the time of the occurrence, the tower controller was controlling both the tower airspace and ground movements. Leading up to the near collision, several of the recently arrived air race aircraft on the ground were requesting clearance and directions to the refuelling bay and parking bays. Additionally, some of these aircraft had left their transponders on, which created clutter on the SSR screen. They recalled being initially aware of an emergency aircraft when discussing the plan to bring the F-35s back with the approach controller. They were also aware that the supervisor was likely talking to someone about the same aircraft however, they believed that the aircraft was outside controlled airspace.
The tower controller reported that, prior to clearing the F-35 formation to land, they conducted a visual scan of their final approach path for traffic, hazards or obstructions. At this time, the PA-28 was 2 NM (4 km) from the runway and 1.2 NM (2 km) from Blackbird 2 on a converging flight path (Figure 6). They further advised that their scan involved looking from the departure end down the runway, along the projected final approach path and around base to see the F-35s on their base turn. From this point they reported that they watched Blackbird 1 land.
Once that aircraft had landed, they looked back up the runway and final to watch Blackbird 2 on final approach. It was at this time that they observed the PA-28 for the first time, and in close proximity to the F-35.
Figure 6: Aircraft positions at the time of F-35 formation landing clearance (1314)
Source: Google Earth with recorded fight data, annotated by the ATSB
Regulations and guidance
Operations in controlled airspace
The requirements for operations in controlled airspace were contained in the Aeronautical Information Publication (AIP), which stated that:
a pilot in command of an aircraft must not enter a control zone or a control area that is a Class A, B, C, D, or E airspace without ATC clearance unless it is a VFR aircraft entering Class E airspace.
In-flight emergencies
When encountering an in-flight emergency, pilots are trained to communicate with air traffic control for assistance by making an emergency declaration. Depending on the nature of the emergency, this declaration can be either:
A MAYDAY call, indicating that the aircraft and occupants are threatened by grave and immediate danger and require immediate assistance
A PAN call, when encountering a less urgent situation, but requiring attention and assistance.
When receiving an emergency declaration, ATC will acknowledge the request, gather more information regarding the nature of the emergency and provide assistance as required.
The AIP contained requirements specific to communication failure that stated:
In the event of a total loss of communication, an aircraft shall:
a. Try to re-establish communication by all other means
Additionally, the ERSA Emergency Procedures for radio failure stated that if the failure occurs in uncontrolled airspace when operating under the visual flight rules, the aircraft was:
to remain in Class G [non-controlled] airspace and land at the nearest suitable airport.
Operations without a radio
Where a radio is inoperative prior to a flight the AIP stated:
Where repair facilities are not available, flight to the nearest appropriate repair facility may proceed in class G [uncontrolled] airspace in VMC only. If flight to the nearest appropriate repair facility entails flight in controlled airspace, the flight may proceed provided that ATS is advised of the radio failure and a clearance for the flight is obtained from ATC.
The AIP also stated that:
An aircraft not equipped with an operative radio may operate at, or in the vicinity of a non-controlled certified or military aerodrome provided that:
a. the aircraft is operated VMC by day; and
b. The aircraft arrives or departs in the company of another radio-equipped aircraft that is flown by a radio qualified pilot which will allow the latter to make radio calls on behalf of both aircraft.
Safety analysis
On 28 August 2025, a pilot and passenger, in a Piper Aircraft PA-28, were participating in stage 4 of the Outback Air Race from Daly Waters Airport to RAAF Base Tindal, Northern Territory. The aircraft lost electrical power during the flight, with the pilot electing to continue to Tindal. On final approach, the aircraft came in close proximity to a Lockheed Martin F-35 that was approaching the same runway.
This analysis will discuss the maintenance conducted prior to departure. In addition, it will examine the pilot’s actions prior to departure, in-flight and in response to the loss of electrical power. The analysis will also consider the actions of air traffic control at Tindal.
Maintenance
Prior to departure, the pilot identified a fault with the alternator and requested assistance from the race-provided LAME. After determining that the alternator was unserviceable, and wanting to get the aircraft to Tindal for maintenance, the LAME encouraged the pilot to conduct the flight. Recognising the need to maximise battery power, they charged the battery prior to departure. However, they did not assess the expected electrical load of the aircraft or the capacity of the battery to determine if it would be able to provide sufficient electrical power for the planned flight. Instead, they provided a level of assurance to the pilot that the battery power was sufficient. In addition, they did not discuss the fault with the pilot in detail nor contingency planning around a failure in flight.
Moreover, no entry was made in the maintenance release to record the alternator issue or the work conducted. Recording this entry was a legislated requirement and such documentation provides the opportunity for pilots and maintenance personnel to have a complete understanding of the nature of the unserviceability.
Planning and monitoring
Prior to the flight, the pilot was aware that maintenance had been conducted on the alternator and that only the battery was supplying electrical power. Therefore, they were aware of an increased risk of losing electrical power during the flight.
In that context, given the increased impact of a total electrical failure when flying to a controlled airport, contingency planning for this scenario should have been conducted prior to departure. Planning on the ground would have identified Homebush Park ALA as a viable alternate Class G airspace destination. It would also have ensured that any action taken aligned with published emergency procedures.
The pilot reported that prior to departure, they successfully reset the alternator’s circuit breaker, and that prior to the electrical failure the aircraft was operating normally. However, the installed ammeter would have shown that the alternator was not operating correctly. Therefore, it is likely the pilot did not monitor the aircraft’s electrical system effectively during the flight.
Pilot actions after the loss of electrical power
When the aircraft was about 15 km from Homebush Park ALA, the electrical charge in the battery depleted sufficiently to result in a loss of electrical power and the pilot was unable to communicate with ATC via radio. However, the pilot had access to a telephone and was given information about how to call ATC directly. This did not occur as the cockpit noise was reportedly too loud to effectively communicate in this manner. In addition, while the passenger’s headset was Bluetooth-enabled, they did not attempt to utilise the functionality due to difficulties using it in the past.
The pilot was concerned about the loss of electrical power and also considered that a possibility of an engine failure existed, due to the detected fumes. The pilot operating handbook (POH) advised that the aircraft should be landed as soon as practicable in such situations. Furthermore, at the time of the electrical power loss, the aircraft was in visual meteorological conditions, in non-controlled airspace and close to Homebush Park ALA. Emergency procedures in the ERSA advised that if the aircraft was in Class G airspace when an emergency occurred, they should remain in non-controlled airspace and land at the nearest suitable airport.
Instead, the pilot communicated via a group chat and fellow race participants relayed information to ATC while the aircraft was without electrical power. During this chat, the pilot advised that they required a PAN declared, after which they incorrectly believed that they had priority to approach and land at Tindal. While declaring a PAN was appropriate given the nature of the emergency, without direct communication with ATC they did not receive confirmation that the PAN had been received. Furthermore, they did not follow advice that ATC had instructed them to remain outside controlled airspace and to land at Homebush Park ALA, consistent with radio failure procedures. It is possible that this was influenced by perceived operational pressure to complete the flight to Tindal to ensure that they arrived in time for the planned maintenance to be conducted. In addition, the pilot was advised via the group chat of the presence of an F-35 on their planned approach path, indicating that traffic had not been cleared for their approach contrary to their expectation.
Air traffic control
ATC had several technologies available to assist in aircraft identification and facilitate the provision of separation. However, the primary radar was not available and, due to the loss of electrical power, the PA-28 was not visible on the secondary surveillance radar. Furthermore, while ATC had access to the OzRunways EFB software, it was unable to show the PA-28 as traffic as the pilot was running a different EFB application.
The approach controller received the first phone call from an OAR participant providing relay information from the PA-28 pilot approximately 5 minutes before the incident. As they directed the PA-28 to remain outside controlled airspace and thought the pilot would use their mobile phone to call and request a clearance, they did not consider the aircraft would enter controlled airspace. However, they advised the F-35 pilots of a possible emergency aircraft and changed their tracking instructions to join the base leg of the circuit. Consequently, the F-35 pilots believed that ATC had knowledge of the aircraft’s location and were providing separation.
The approach supervisor answered a call from an OAR participant, approximately 3 minutes prior to the near collision. They considered that the PA-28 was remaining outside controlled airspace and initially thought the caller was in the aircraft. However, as they clarified the situation and were advised that the PA-28 was 3 minutes from the runway and had the runway in sight, the PA-28 was joining final in close proximity to the second F-35. It could not be determined if there was sufficient time for the approach controllers to assess the information as credible and relay it to the tower controllers in time for action to be taken to prevent the occurrence.
Concurrently, 2 minutes before the incident, the tower supervisor also received a phone call about the PA-28. Although information provided in the call included the nature of the emergency and the aircraft’s callsign, the details provided were limited and did not include the aircraft’s position. As a result, they attempted to identify the aircraft on the SSR screen rather than acquire them visually. Without knowing its approximate position, it was unlikely that conducting a visual scan would have successfully located the aircraft. In addition, as the phone call continued through to the near collision there was limited opportunity to conduct the scan.
The tower controller conducted a visual scan when clearing the F-35 formation to land. However, at the time the PA-28 was approximately 2 NM (4 km) from the runway threshold and away from the approach path of the formation where the controller’s scan was focused. In addition, while they were aware of the existence of an aircraft with an emergency, they believed that it was remaining outside the control zone.
Consequently, while the aircraft was close enough to be visible to the controller, they did not detect it during their visual scan when clearing the formation to land. Following this visual scan, the controller watched the first F-35 through to landing so they did not sight the PA-28 before the near collision occurred.
Finally, while well intentioned, the multiple telephone calls from several participants in the race to different ATC personnel created confusion that aggravated the situation. Had specific individuals been nominated to contact ATC and the PA-28 occupants in a coordinated manner, communication of the situation (and the plan to resolve it) would have been clearer to all involved. This may have prevented the occurrence.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the near collision involving Piper PA-28, VH-TKX and a Lockheed Marting F-35 Lightning II, at Royal Australian Air Force Base Tindal, Northern Territory, on 28 August 2025.
Contributing factors
After identifying a fault with the alternator, the licensed aircraft maintenance engineer encouraged the pilot to conduct the flight without assessing the time the battery could supply the aircraft with electrical power. Additionally, they did not record the issue or maintenance activity on the aircraft’s maintenance release.
Prior to departure, the pilot did not conduct contingency planning to prepare for a loss of electrical power in-flight. In addition, during the flight the pilot did not effectively monitor the aircraft’s electrical system. Subsequently, the aircraft lost electrical power and the pilot was unable to communicate with air traffic control via the aircraft’s radio, and the aircraft could not be detected by the surveillance systems in use.
The pilot did not divert to the closest airport or follow advice to remain outside controlled airspace, and the aircraft entered controlled airspace without the required clearance. Subsequently, the aircraft joined final approach in close proximity to an F‑35 approaching the same runway.
When conducting a visual check of the F-35 formation’s approach path, the tower controller did not detect the PA-28 on approach to the runway.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot of the PA-28
pilots of the F-35s
Outback Air Race maintenance engineer
Outback Air Race flight manager
owner / maintainer of the PA-28
air traffic controllers
Defence Flight Safety Bureau
recorded data from the GPS unit on the aircraft.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of the PA-28
pilots of the F-35s
Outback Air Race maintenance engineer
Outback Air Race flight manager
owner / maintainer of the PA-28
air traffic controllers
Defence Flight Safety Bureau
Civil Aviation Safety Authority.
Submissions were received from the:
pilot of the PA-28
Outback Air Race flight manager
air traffic controllers
Defence Flight Safety Bureau.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2]Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
[3]A military-specific manoeuvre where the aircraft joins an extended centreline of the duty runway then conducts a high‑speed pass over the runway before turning 180° and slowing to join the downwind leg of the circuit.
[4]The group chat was set up between the race management and participants to share important information.
[5]As the phone calls were not recorded the ATSB was unable to verify the content of the conversation.
[6]75 Squadron operated F-35 aircraft from Tindal.
Occurrence summary
Investigation number
AO-2025-051
Occurrence date
28/08/2025
Occurrence time and timezone
1315 Central Standard Time
Location
RAAF Base Tindal
State
Northern Territory
Report release date
19/03/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Electrical system, Near collision, Radar/surveillance
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the ATSB to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation. This statement is published as a report in accordance with section 25 of the TSI Act, capturing information from the investigation up to the time of discontinuance.
The occurrence
On 14 May 2020 at about 0030 Western Standard Time,[1] an Airbus A330-203 aircraft registered VH-EBL, was operating as Qantas flight QF044, a scheduled passenger service between Sydney, Australia and Denpasar, Indonesia. While in the cruise at flight level 390[2] and abeam the Royal Australian Air Force Curtin aerodrome near the West Australian coast, the first officer’s primary flight, navigation and multipurpose control displays lost power and went blank. Accompanying this, the autopilot disconnected, the cockpit Master Warning light illuminated with an aural alert and multiple electronic centralised aircraft monitor (ECAM) messages presented on the engine/warning display.
The flight crew assumed manual aircraft control and worked to complete the appropriate response checklists and to better understand the issue. At 0038, the crew made a PAN[3] call to air traffic control (ATC) advising of the electrical problem and the possible need to divert. That decision was made at 0044 and the crew advised ATC that they would be diverting the aircraft to Broome – approximately 170 km from their position.
The flight crew reported that while some inoperative systems were restored during the diversion, other systems remained unavailable. All flight, navigation and multipurpose controls on the captain’s side of the flight deck remained functional throughout the flight. The approach to and landing on runway 10 at Broome was uneventful and the aircraft touched down at 0150.
Overview of the investigation
Following notification of the occurrence, the ATSB initiated an investigation under the Transport Safety Investigation Act 2003, for the purposes of examining the electrical systems event and the flight crew’s response. Information was obtained from the aircraft manufacturer and operator, including formal technical and operational investigation reports from both Airbus and Qantas. ATSB investigators interviewed both flight crew and the information thus provided was correlated against the technical and operational reports.
In summary, based on information gathered during the investigation, it was found that the electrical systems event had originated within the aircraft’s number-two integrated drive generator (IDG) and generator control unit (GCU) systems. The event produced abnormal behaviours in related electrical systems which were not immediately or definitively indicative of an IDG or GCU fault – making the task of fault diagnosis difficult. Indeed, engineering staff examining the aircraft after arrival in Broome and following relocation under special authority to Brisbane, were unable to replicate the systems behaviour reported by the flight crew.
Reasons for the discontinuation
Following a review of the investigation and the information gathered, the ATSB has discontinued its investigation of this occurrence as a result of the following principal considerations:
The flight crew, despite receiving unclear information from the monitoring systems, recognised that the aircraft’s systems were significantly degraded and appropriately managed the risks by diverting to the nearest suitable airport.
The aircraft flight crew’s responses to the system failures during the diversion effectively managed the risks presented by the degraded aircraft systems.
The approach and landing at the diversion airport was appropriately managed and uneventful.
The operator and manufacturer’s combined investigations into the technical origins of the electrical systems event, while unable to conclusively identify root cause, did isolate the areas of likely contribution.
Both manufacturer and aircraft operator have undertaken proactive safety action in response to the technical failure areas of concern.
The operator has similarly assessed the operational and logistical issues arising from the use of Broome as a diversionary destination.
As such, the ATSB considered it was unlikely that further independent investigation would identify any systemic safety issues or important safety lessons.
The evidence collected during this investigation remains available to be used in future investigations or safety studies. The ATSB will also monitor for any similar occurrences that may indicate a need to undertake a further safety investigation.
On arrival in the circuit area at Wedderburn, the pilot was unable to extend the landing gear by the normal method. The failure of the gear to extend was accompanied by a very loud high-pitched noise in the headset and speaker systems. His attempts to lower the landing gear by the manual emergency system were also unsuccessful.
As a result, the pilot elected to return to Bankstown. However, on arrival in the circuit, he was unable to communicate by radio to the Tower or other aircraft. Air traffic control staff recognised the pilot was experiencing difficulties with the landing gear and called out the emergency services. When the services were in place the aerodrome was closed and the pilot advised by signal light that he was cleared to land.
The aircraft subsequently landed on runway 11 with the landing gear retracted. An investigation revealed a fault in the alternator field circuit which prevented the battery from being charged. The landing gear failed to extend by the normal means due to low battery voltage. The pilot was unable to lower the gear by the manual system because he could not gain access to the emergency gear extension handle due to an incorrectly fitted piece of interior trim. It was not determined how the trim came to be incorrectly fitted.
Occurrence summary
Investigation number
199303630
Occurrence date
06/11/1993
Location
Bankstown
State
New South Wales
Report release date
13/09/1994
Report status
Final
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Electrical system, Landing gear/indication, Wheels up landing
During the pre-flight check at Los Angeles, when the Standby Power switch was selected to Battery, the captain's electronic navigation displays went blank, the upper Engine Indication and Crew Alerting System (EICAS) display transferred to the lower screen, and an additional message 'Standby Bus Main' was displayed. It was later determined that the standby inverter was missing from the aircraft. Investigation determined that the inverter had been removed in Sydney on the previous day, to service another aircraft.
Maintenance engineers involved with the removal did not raise the appropriate documentation as they were unaware of the requirements of the company Policy and Procedures Manual. No formal shift handover was conducted, consequently subsequent shift personnel were unaware of the missing component and released the aircraft for service. The aircraft was then flown to Los Angeles.
During the departure preflight cockpit check at Sydney, the correct responses were displayed when the standby power test was performed but the crew were not alerted to the additional 'Standby Bus Main' message as the checklist does not mention it. EICAS display transfer to the lower screen was not noticed as the cockpit was sunlit and the captain's navigation instrument displays were selected to low intensity at the time.
Significant factors
1. The maintenance crew was unaware of the required documentation procedures.
2. The maintenance crew did not conduct a formal shift handover.
3. The cockpit checklist was deficient with regard to testing the standby power system.
Safety action
As a result of this investigation the operator advised that they had initiated the following safety actions in respect to the deficiencies relating to the training of certifying engineers on the requirements of the company Policy and Procedures manual:
1. The course notes for the LAME Introduction Course were distributed to all LAMEs including those at line stations. A where to find it booklet was also given to AMEs. These actions were completed by the end of August.
2. Maintenance Memo Number M1884 was issued to alert all LAMEs to their responsibility to follow approved procedures. It provided information as to which volume would be relevant to the particular work area.
3. In conjunction with item 2, Department Heads checked and, in some cases, improved the availability of the appropriate P.&P. Manuals in their areas. This was completed prior to the end of August.
4. In order to provide a concise and accurate analysis of incidents for those persons who need to know we have introduced a Quality Alert Bulletin. The objective of which is to ensure all benefit from the lessons learned. The information is depersonalised for obvious reasons.
5. While there was nothing wrong with the existing procedure for serviceable transfer (Vol. 5 chapter 3-40-05) we took the opportunity to emphasise its existence when it was revised.
Maintenance Memo M1880 refers.' The Bureau of Air Safety Investigation made the following interim recommendations on 9 February 1994:
IR940015
The Bureau of Air Safety Investigation recommends that the Civil Aviation Authority liaise with the Boeing Commercial Airplane Company, in conjunction with the Australian operator, to amend the B747-438 Flight Deck Preparation Checklist to include reference to additional EICAS messages that will be displayed when an unacceptable condition exists with the standby power system.
The CAA response stated, in part: 'The Authority believes that the abnormal indication of the Captain’s display blanking and EICAS transfer to the secondary screen should have been sufficient indication that there was a problem with the aircraft systems. We do not believe it is reasonable to expect aircraft systems to compensate for abnormal maintenance actions and the range of inappropriate actions that are possible would make such an approach difficult to address. Nevertheless, the Authority will raise the matter of amendment to the B747-400 Flight Deck Preparation Checklist to highlight that further investigation of any unusual indications during flight deck preparation checks is necessary.'
The operator response stated: 'I have enclosed a copy of a revised page for the 747-400 Operations Manual. This revision has been written as a result of the referenced A.S.I.R. The revision is highlighted by a margin line bar and will be processed as part of a general revision to go to printing at the end of the week. Rather than make the comment specific to the Standby Power check, I have included it as part of the preamble to the whole flight deck preparation. I feel that this is more appropriate as there are potentially other areas where a similar problem could occur should these circumstances ever arise again.
IR940016
The Bureau of Air Safety Investigation recommends that (the operator) conduct a review of policy relating to shift handover procedures to include directions for individuals as well as supervisors.
The operator response stated, in part: 'The reason the static inverter was not fitted to VH-OJB was that the engineer who removed the inverter failed to carry out the requirements of the Policy and Procedures manual in regards to not entering in the aircraft log book or work package that the inverter had been removed from the aircraft to service the other aircraft. By making an entry as required the person removing the item is also fulfilling the requirements of an individual handover as this entry has to be acquitted prior to the Maintenance Release being certified.
After the investigation of this incident the engineer involved was counselled and disciplinary action was effected against him. As well the Policy and Procedures manual reference to the actions required when cannibalising aircraft components has been amended to clarify the requirements when carrying out this function. These procedures have since been widely distributed to all Sydney Line Maintenance staff.'
Shortly after take-off the warning annunciator for the 26V AC bus supply illuminated followed by a strong electrical burning smell. Power was removed from the bus and the smell diminished. After a successful landing the investigation disclosed that a power supply diode had overheated and failed.
On the flight from Flinders Island an electrical failure occurred. The pilot continued to Latrobe Valley and made a landing approach behind another aircraft. On final approach, for runway 21, the aircraft was too low, and the pilot advanced the throttle to correct for this. The engine missed then fired again. The pilot checked the carburettor heat setting and found that it was in the hot position. He pumped the throttle, and the engine kept losing and gaining power and then ran normally.
Because of the low height and the terrain ahead, which included a power line, the pilot elected to put the aircraft down in a small clear area. A very heavy touchdown followed, and the aircraft ran through a fence before stopping.
Following the accident the aircraft was found to contain an adequate amount of fuel. No inspection of the engine or its systems was carried out, and the reason for the interruption of power was not determined.
Significant Factors
The following factors were considered relevant to the development of the accident:
1. A partial engine power loss and engine rough running for an undetermined reason.
2. The decision, by the pilot, to land in a small but immediately adjacent clear area.
3. The aircraft was landed heavily.
Occurrence summary
Investigation number
199400816
Occurrence date
01/04/1994
Location
1 km north-north-east of Latrobe Valley
State
Victoria
Report release date
28/06/1994
Report status
Final
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Electrical system, Forced/precautionary landing, Hard landing
On 7 January 2008, a Boeing Company 747 438 aircraft, registered VH-OJM, was being operated on a scheduled international regular public transport service between London, England and Bangkok, Thailand. The aircraft had 346 passengers and 19 crew on board, including four flight crew.
At about 0837 UTC, while the aircraft was at about 21,000 feet on descent to Bangkok International Suvarnabhumi Airport, the customer service manager (CSM) notified the flight crew that a substantial water leak had occurred in the forward galley.
Between approximately 0840 and 0852, cockpit indications showed a number of electrical bus and system failures that indicated alternating current (AC) buses 2, 1 and 3 were not powered. The status of AC bus 4 appeared normal and some systems were powered by batteries.
The captain's primary flight display, navigation display, and some other instruments were available in a degraded mode. Standby instruments and the aircraft's instrument landing system were also available. The crew conducted an approach to runway 01 Right in day visual meteorological conditions and the aircraft landed at 0907.
On 11 January 2008, the aircraft manufacturer issued a Multi Operator Message to operators of 747 400 series aircraft, containing advice and instructions for the inspection and repair of main equipment centre drip shields. The manufacturer is preparing an inspection and repair alert service bulletin on the same subject that is scheduled for release by May 2008.
On 11 January 2008, the aircraft operator issued a Cabin Standing Order and a Flight Standing Order requiring cabin and flight crews to treat and report abnormal water accumulation in galley areas.
Summary
On 7 January 2008, a Boeing Company 747-438 aircraft, registered VH-OJM, was being operated on a scheduled international regular public transport service between London, England and Bangkok, Thailand. The aircraft had 346 passengers and 19 crew on board, including four flight crew. On descent to Bangkok International Airport, the customer service manager notified the flight crew that a substantial water leak had occurred in the forward galley.
The cockpit indications progressively showed a number of electrical power-related malfunctions, and many of the aircraft's communication, navigation, monitoring and flight guidance systems were affected. A number of flight and navigation display and other instruments were available in degraded mode and the standby instruments and instrument landing system were also available. The aircraft's engines and hydraulic and pneumatic systems were largely unaffected and an approach was made to Bangkok in day visual meteorological conditions.
The investigation found the galley leak was from an overflowing drain after a drain line had been blocked with ice that formed due to an inoperable drain line heater. The water flowed forward and through a decompression panel into the aircraft's main equipment centre before leaking onto three of the aircraft's four generator control units, causing them to malfunction and shut down.
The investigation identified a number of safety issues in regard to the protection of aircraft systems from liquids, and other factors including the provision of information to flight crews. In response, the aircraft manufacturer and operator implemented a number of safety actions intended to prevent a recurrence. In addition, the United States Federal Aviation Administration issued a notice of proposed rulemaking to adopt a new airworthiness directive for certain 747-400 and 747-400D series aircraft to install improved water protection. The Australian Transport Safety Bureau has issued two safety recommendations and one safety advisory notice as a result of the investigation.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation.
What happened
On 6 September 2018, a Boeing 737-476 freighter was in the hanger at Brisbane Airport, Queensland undergoing routine maintenance. The crew reported that the cockpit voice recorder (CVR) was not testing and the circuit breaker was tripping.
While engineers were conducting troubleshooting on the aircraft, they discovered a heat damaged wiring loom located in the aft[1] lower cargo hold ceiling, adjacent to the CVR mount rack. The wires were severely burnt in a localised area with melted insulation and evidence of a possible fire. Engineers suspect this may have been caused by swarf[2] damaging the wiring and causing it to arc. Swarf ingress in the wiring loom was discovered from previous cargo conversion work.
Figure 1: Heat damaged wiring loom
Source: Operator’s engineering department
Safety message
This incident highlights the importance of ensuring that while an aircraft is in maintenance, that all aircraft components are checked thoroughly to ensure proper functionality. When conducting any work on an aircraft, it is also vital to ensure that all areas are thoroughly cleaned to ensure no debris is left behind, as it may cause faults to the aircraft and its systems.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.