When the aircraft reported at the position reporting point after Mt Isa, it was found that it was not tracking on the route expected by air traffic controllers. There was no confliction with other aircraft, and the aircraft was recleared along the route it was tracking.
Earlier in the day the original flight plan was submitted to track via air route A575 after passing Mt Isa. This plan was later cancelled and another submitted to track via air route A464 after Mt Isa. The first route is the preferred tracking, and the amendment resulted from the possibility of adverse weather on air route R575.
Prior to departure from Brisbane information indicated that weather was now suitable on R575. The airline company operations personnel checked if the Brisbane Briefing Office held a flight plan on the aircraft, and when they were advised that the office did not hold a plan another plan was submitted for the aircraft to track via air route R575. However, as the first two plans had been submitted by the airlines base in Bangkok through Melbourne (normal practice), Brisbane was unaware of the existence of a plan for the aircraft. As a result, a cancellation message was not sent prior to the third plan being submitted.
Flight Progress Strips are prepared for each plan by two sections in the Brisbane control centre and distributed to controllers who will become responsible for the control of each aircraft. On this occasion, when the third plan was submitted it was assumed that it was a duplication of one of the previous plans, probably because no cancellation message was received, and no strips were prepared for the controllers. As a result, the controllers assumed that the aircraft would track via air route A464 after Mt Isa.
The controller who received the Mt Isa position report marked the information on the strip for the next position reporting point along air route A464 and not along R575, the point that the aircraft advised it would report at next. He then co-ordinated the Mt Isa position with the next controller responsible for the aircraft. This controller also had strips for air route A464 and was not aware the aircraft was tracking via air route R575 until the next position report from the aircraft.
F-ODGX planned Melbourne to Sydney via Strathbogie, designated route W32, Cullerin, Bindook and Oakdale to Sydney. Due to limitations, the computer aided strip printing system (CASPS) did not recognise waypoint Oakdale in the flight plan as valid and consequently could not print the strips.
An airways data system officer (ADSO) in the Melbourne area approach control centre (AACC) amended the plan which was then re-run with errors and omissions such as speed, flight level and route.
As a consequence, the Melbourne sector 2 and 7 enroute flight progress strips then incorrectly indicated that the flight was tracking via Strathbogie, W32, waypoint Cullerin to Sydney. Coincidently, the Sydney AACC advised non receipt of plan details on F-ODGX. The flight plan forwarded was the incorrect amended version.
F-ODGX's airways clearance was to track via Strathbogie to Sydney. On departure, the clearance was amended to track direct to Cullerin. The amended clearance was accepted by the pilot because it was on the flight planned route. At 130 NM from Melbourne, the aircraft was given a Rivet 1 arrival by Melbourne Sector 2. The pilot's readback of the clearance was unintelligible. At 160 NM from Sydney the aircraft was given an instruction to enter the holding pattern at 70 NM Sydney, with the requirement to reach flight level (FL) 210 by 70 NM from Sydney. This holding pattern is published on the Standard Instrument Arrival (STAR) plates and is located on the 230 radial, 70 NM from Sydney. On the route which the pilot followed, from Cullerin to Bindook, there is no published holding pattern at 70 NM Sydney. The pilot did not query the holding instruction reference the direction of the turn or the inbound radials.
Due to Sydney arrival sector also working from incorrect flight progress strip information, the flight planning error was not detected until the arrivals radar controller observed the aircraft making a left turn towards Bindook instead of a right turn towards Rivet.
At the time of this incident, another aircraft was tracking from Wagga Wagga to Bindook at FL210. Had the arrivals controller not observed and adjusted the incorrect turn by F-ODGX, a loss of separation standards may have occurred.
The incorrect routing of F-ODGX would have been rectified at the clearance delivery stage if the correct flight plan had been presented to the controllers handling the flight.
Significant Factors
1. The CASPS waypoint data was not compatible with the current air route structure.
2. The ADSO incorrectly amended the original flight plan.
3. The Melbourne sector controller did not obtain a valid readback of the STAR clearance.
4. The pilot did not query the inconsistent holding instruction.
Safety Actions
The Civil Aviation Authority Air Traffic Services has initiated new procedures regarding the method and circumstances in which filed flight plans may be re-run through the CASPS equipment.
The pilot of VH-TJL reported ready at the holding point for runway 23 and was cleared for take-off. He had noticed the landing lights of Singapore Airlines SIA227 on a 7-mile final and queried the clearance. The air traffic controller confirmed that he was cleared for an immediate take-off.
As VH-TJL commenced to roll, SIA227, which was now on a 2.5 mile final at approximately 600 feet, was cleared to land, but the pilot elected to make a missed approach and commenced a go-around. In the air traffic controller's opinion, an unsafe situation could develop if VH-TJL climbed up towards the overflying Boeing 747, so cancelled its take-off clearance. The take-off was rejected from below V1 speed, and after completing checklist procedures the aircraft taxied from the runway. Garuda Airlines GIA227 on a 3-mile final was cleared to land but also went around.
Pre-dawn conditions existed at the airport with light and variable winds on the ground, but aircraft reported strong south-easterly winds with moderate to severe turbulence above 500 feet which may have allowed a faster than normal final approach. A CAA investigation with supporting information, found that a breakdown in separation standards had not occurred, and runway separation standards would have been maintained if either aircraft had continued its approach for landing.
After departure the pilot's intention was to track through the Oakey restricted airspace if possible. He contacted Brisbane Flight Watch and requested the status of the Oakey airspace. The operator advised him that the airspace was de-activated. As the pilot believed that this was unusual, he asked for confirmation that the airspace was not active. The response was that that was correct.
The pilot then continued towards Toowoomba and monitored the Oakey MTAF, while operating his transponder in altitude reporting mode. A short time later he heard Brisbane Flight Service make an all-stations call asking the aircraft west of Oakey to call Oakey. He acknowledged that transmission and called Oakey. At this time, he was advised that his aircraft was some eight miles inside controlled airspace.
When the pilot advised the Oakey controller what had transpired the controller undertook to contact Brisbane. The airspace had been active for most of the day.
The Brisbane Flight Service officer was unable to explain why he had told the pilot that the airspace was not active. He had checked the status board and noted that the airspace was active but had reported it as not active. Workload at the time was normal for the position.
VH-BPZ was en route from Wynyard to Phillip Island, cruising at 8000 feet and estimating the Marsh reporting point at 0555 UTC. VH-OZT was en route from Moorabbin to Wynyard, cruising at 9000 feet and also estimating Marsh at 0555 UTC. At 0551 UTC the pilot of VH-OZT called Melbourne Flight Service requesting traffic for descent to Wynyard. VH-OZT was advised of traffic (VH-EXC) inbound to Wynyard from the south. About 15 seconds later, the pilot of VH-BPZ asked flight service about "the Navajo for Wynyard". Flight service then gave traffic information to BPZ and OZT on each other's locations/estimates. The two aircraft then effected mutual separation.
The investigation determined that the flight service workload was heavy at the time of the occurrence. Both western sectors were combined at one console, but the traffic was confined to only one of the sectors. The console was staffed by two Flight Service Officers, one acting as a co-ordinator and the other as a traffic information officer. Prior to the occurrence, the traffic information officer had considered the traffic implications of VH-BPZ and VH-OZT but had concluded that they would have 1000 feet vertical separation at the time of passing. Therefore, when VH-OZT requested traffic for descent, the officer concentrated on traffic in the immediate Wynyard area and overlooked VH-BPZ.
Significant Factors
The following factors were considered relevant to the development of the occurrence:
1. The flight service workload in the sector of the occurrence was heavy at the time of the occurrence.
2. The traffic information officer had previously assessed the traffic situation of the two aircraft involved and had dismissed them as traffic for each other on the basis of 1000 feet vertical separation. A reassessment was not made when the pilot of VH-OZT requested traffic for descent.
At 1503 Eastern Standard Time on 27 May 2014, mutual traffic information was not passed to the flight crews of a Department of Defence (Defence) Boeing CH‑47 Chinook helicopter (CH‑47), and a Cessna 172S, registered VH‑PFU (PFU), operating in the circuit area at Townsville Airport, Queensland. At the time, the Defence air traffic controller with jurisdiction over the circuit area (the tower controller), had six other aircraft on frequency. All of the aircraft were operating under visual flight rules in visual meteorological conditions.
The complexity of aircraft operations, and a high level of radio frequency use, resulted in high workload for the tower controller and the tower supervisor.
The flight crew of the CH‑47 had been issued with a clearance limit of a point on the coast north‑east of the airport. At the same time, the flight crew of PFU were tracking on the centreline of runway 07 as instructed by the tower controller. As the flight crew of the CH‑47 turned left to commence an orbit at the clearance limit, they sighted PFU in close proximity. The flight crew reversed the turn, tracking away from PFU.
Seeing that the CH‑47 had commenced a turn away from the track of PFU, the tower controller did not provide traffic on PFU, but instead provided traffic on another aircraft that the CH‑47 was to track behind. Additionally, traffic on the CH‑47 was not passed to the flight crew of PFU. When the flight crew of the CH‑47 first reported sighting PFU, surveillance data indicated that the aircraft were at the same altitude and separated by about 0.5 NM (1 km).
What the ATSB found
The ATSB found that mutual traffic information was not passed to the flight crews of the CH‑47 and PFU prior to them coming into proximity. Then, when the flight crew of the CH‑47 reported PFU in sight, the tower controller did not pass traffic on that aircraft as they believed that the proximity risk had been resolved by the CH‑47 turning away. At the time of the occurrence, compromised separation recovery training deficiencies existed within Defence.
What's been done as a result
Actions by Defence in relation to compromised separation recovery training have adequately addressed the identified training deficiencies. In addition, Defence has reinforced to controllers, via briefings, the importance of workload and traffic management.
Safety message
The impact of workload can be insidious, the affected person(s) not realising an increase until it has reached a high level. The ATSB suggests that consciously self-monitoring and actively monitoring the workload of colleagues can assist a work group to better manage workload. Holding aircraft on the ground or outside the airspace are valuable tools for an air traffic controller. The ATSB also notes that flight crew operating under visual flight rules in Class C airspace should remain aware that the provision of an air traffic service does not negate their responsibility to see and avoid.
Context
Personnel information
Townsville Tower was staffed by three Department of Defence (Defence) air traffic controllers, the:
supervisor
tower controller
surface movement controller.
Each controller was correctly endorsed and no fatigue‑related issues were identified. The supervisor was also endorsed in all tower and approach positions. The tower controller and supervisor had completed the then Defence compromised separation recovery training as part of Townsville’s overall air traffic control training package, not as a stand-alone training element.
Airspace information
Defence was the controlling authority for the Class C airspace[6] around Townsville Airport and, with the circuit active, the tower controller was responsible for separating and sequencing aircraft within 5 NM (9 km) of the airport at and below 1,500 ft. The Class C airspace outside the circuit area was the responsibility of the Defence-employed approach controller. Defence controllers use the same control techniques as Airservices Australia controllers when controlling civil, or a combination of civil and military aircraft.
Procedures at Townsville permitted standard transfers of responsibility between approach and tower controllers when the circuit was active. One of these standard transfers was the use of Kissing Point as a clearance limit for helicopters tracking inbound from the east. Once the pilot of the occurrence CH-47 contacted the tower controller, irrespective of distance from Townsville Airport, the approach controller would generally have no tracking restrictions on the helicopter’s arrival. This was not the case when the helicopter was carrying an external load.
Clearance limits
A clearance limit is issued to the flight crew of an aircraft when the controller is unable to authorise an aircraft to proceed beyond a certain point or place. When a clearance limit is imposed by a controller, the flight crew must hold at that point until issued with an onwards clearance. Holding involves either a holding pattern or an orbit, which may be documented or the controller may stipulate the type and direction. Often, holding at a clearance limit is not required, as the controller is able to provide an onwards clearance prior to the aircraft reaching the limit. In these cases, the clearance limit would have been imposed to assure separation as the aircraft progressed along its track.
Separation assurance can be either strategic or tactical. Strategic separation assurance includes the development of air traffic practices to reduce the likelihood of aircraft coming into conflict, particularly where traffic frequency congestion may impair control actions. Tactical separation assurance is an activity conducted by the controller that includes traffic planning and conflict avoidance.
The Defence operational documentation for air traffic control stipulated that all military helicopters arriving at Townsville Airport from the east, when the circuit was active, would be tracked via Kissing Point. In this case, Kissing Point was stipulated as the clearance limit. The approach controller, when first contacted by the flight crew of the inbound military helicopter, would issue this clearance and clearance limit. The tower controller would then be responsible for cancelling the clearance limit and providing separation between the helicopter and all other aircraft within 5 NM (9 km) of Townsville. The documentation did not include the direction of turn for a helicopter holding at Kissing Point.
Traffic information
Traffic information is issued by an air traffic controller, to alert a pilot to other known or observed air traffic. This traffic may be in proximity to their position or intended route, and the issued traffic information helps the pilot avoid a collision. When aircraft are operating under visual flight rules (VFR) in Class C airspace, separation is not required. However, mutual traffic information is required when, in the controller’s judgement, one aircraft may observe another aircraft and could be uncertain of their intention.
Traffic information should be concise and, to assist flight crew in identifying other aircraft, may include the following information if deemed relevant by the controller:
aircraft identification
type and description, if unusual
position information
direction of flight or route of the aircraft
level
intentions of the pilot.
The provision of traffic information, and the content of that information, is reliant on the controller’s assessment of the underlying need. The initial provision of traffic information to the flight crew of an aircraft tracking to join the circuit could be general in nature; for example ‘the circuit is active on runway 01 and 07’. The information would then become more specific as the aircraft tracked closer to the circuit; for example, providing the type and location of those aircraft that the flight crew of the joining aircraft would encounter.
Compromised separation recovery training
Compromised separation recovery actions are important emergency response actions. They need to be implemented by controllers promptly and accurately when determined that separation standards have been, or will shortly be compromised. To ensure emergency response actions are conducted effectively, they need to be regularly practiced. Skill decay is more likely to occur when tasks are rarely performed (Arthur and others 1998), as is the case for compromised separation recovery actions during actual controlling.
Controllers are required to issue safety alerts to pilots of aircraft as a priority when the controller becomes aware that aircraft are considered to be in unsafe proximity to other aircraft. This is the case unless a pilot advises that action is being taken to resolve the situation, or that the other aircraft is in sight.
At the time of this occurrence, Defence controllers were not provided with stand-alone, regular practical refresher training in identifying and responding to compromised separation scenarios. An ATSB investigation into a loss of separation (LOS) at Williamtown (Newcastle Airport), New South Wales in 2011[7] found that Defence had not provided compromised separation recovery training as part of initial or ongoing controller training. In addition, an ATSB research report into LOS between aircraft in Australian airspace, which was released in October 2013,[8] found that controller actions to manage a compromised separation occurrence were not effective for Defence-employed controllers and those employed by Airservices Australia. Finally, after this occurrence at Townsville, in October 2014 the ATSB released a report into a LOS at Darwin, Northern Territory[9] that identified a safety issue in relation to the provision of compromised separation recovery training for Defence-employed controllers.
Related occurrences
The ATSB research report AR-2012-034 Loss of separation between aircraft in Australian airspace – January 2008 to June 2012 found that ‘assessing and planning’ or ‘monitoring and checking’ errors were involved in most individual controller actions that contributed to LOS occurrences. Ineffective management of compromised separation before it became a LOS was categorised as an assessing and planning error. Monitoring and checking errors included controller actions associated with maintaining awareness of traffic disposition.
In addition, the ATSB research report found that of the LOS occurrences in which ATC actions were contributory, about one quarter involved communication errors. These included not passing traffic information to pilots once separation was compromised. The research report found that task demands were the most common type of local condition identified in LOS occurrences where controllers were involved – in particular, high workload and distractions. Common in all ATC environments, these local conditions were more common in the tower environment.
Though this occurrence at Townsville did not involve a LOS, as no separation was required in Class C airspace between VFR aircraft, the error types are relevant. However, a review of the ATSB occurrence database did not identify any similar occurrences where mutual traffic was not provided to VFR aircraft in Class C airspace.
At 1503 Eastern Standard Time[1] on 24 May 2014, mutual traffic information (see the section titled Traffic information) was not passed to the flight crews of a Department of Defence (Defence) Boeing CH‑47 Chinook helicopter (the occurrence CH‑47) and a Cessna Aircraft Company 172S, registered VH‑PFU (PFU). Both aircraft were operating in the circuit area at Townsville Airport, Queensland (Figure 1). As neither flight crew were advised of the other aircraft, and aircraft proximity became a concern, the flight crew of the occurrence CH‑47 reversed the direction of their turn to remain clear.
At the time, the Defence air traffic controller with jurisdiction over the circuit area (the tower controller) had the following aircraft on frequency:
a Defence CH‑47 operating circuits from and to a helipad 1 NM (2 km) to the west of the airfield
a Defence Beechcraft King Air 350 (King Air) conducting circuits on runway 01[2]
a Robinson Helicopter Co R22 (R22) operating to the south
a McDonnell Douglas Helicopter Company 369E (MD500) inbound from the south-west
PFU conducting circuits on runway 07
two Defence Sikorsky Black Hawk helicopters (Black Hawks) tracking from the south to a location 2 NM (4 km) to the south-east of the airport
the occurrence CH‑47 tracking along the coast from the east south-east to a clearance limit of Kissing Point (see the section titled Clearance limits)
an aircraft holding on the ground for departure from runway 01.
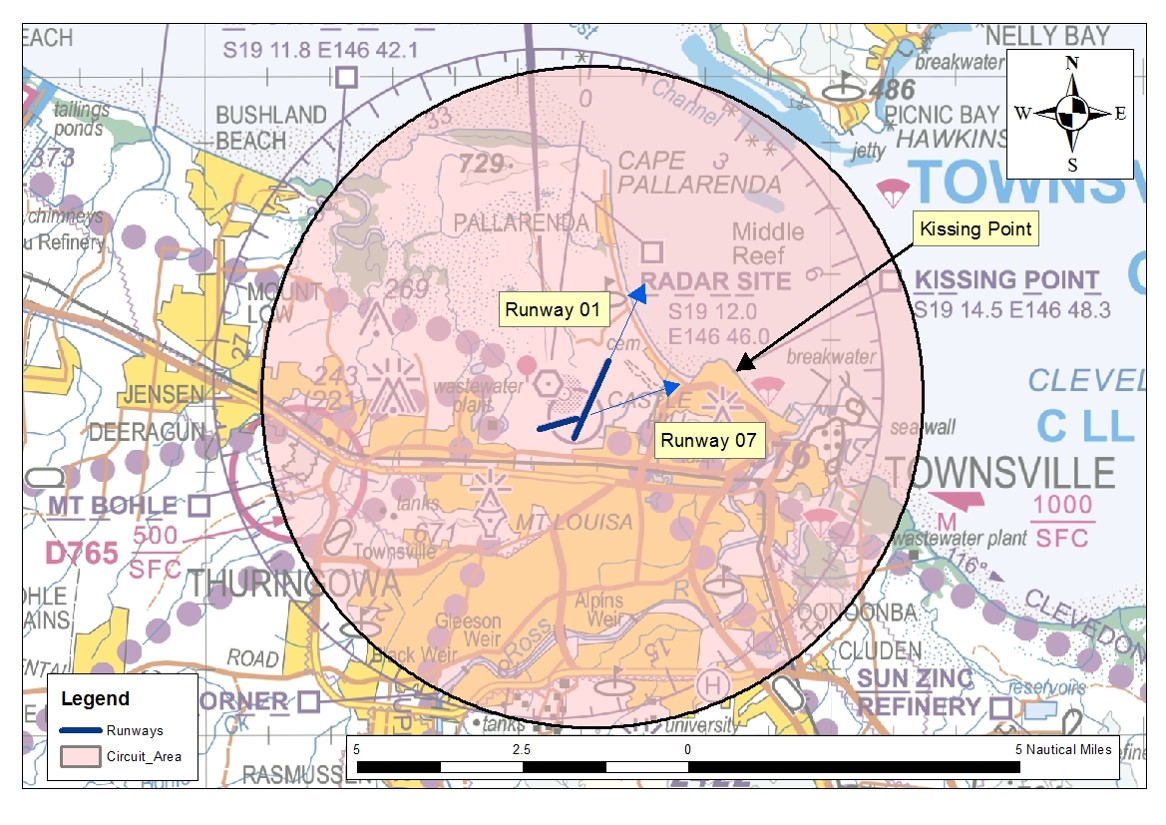
Figure 1: Townsville circuit area (shaded), showing the runways in use and Kissing Point
All of the aircraft were operating under visual flight rules (VFR)[3] in visual meteorological conditions[4] below 1,500 ft above mean sea level within the 5 NM (9 km) circuit area. The Townsville Control Tower was staffed by a tower supervisor, the tower controller and the surface movement controller.
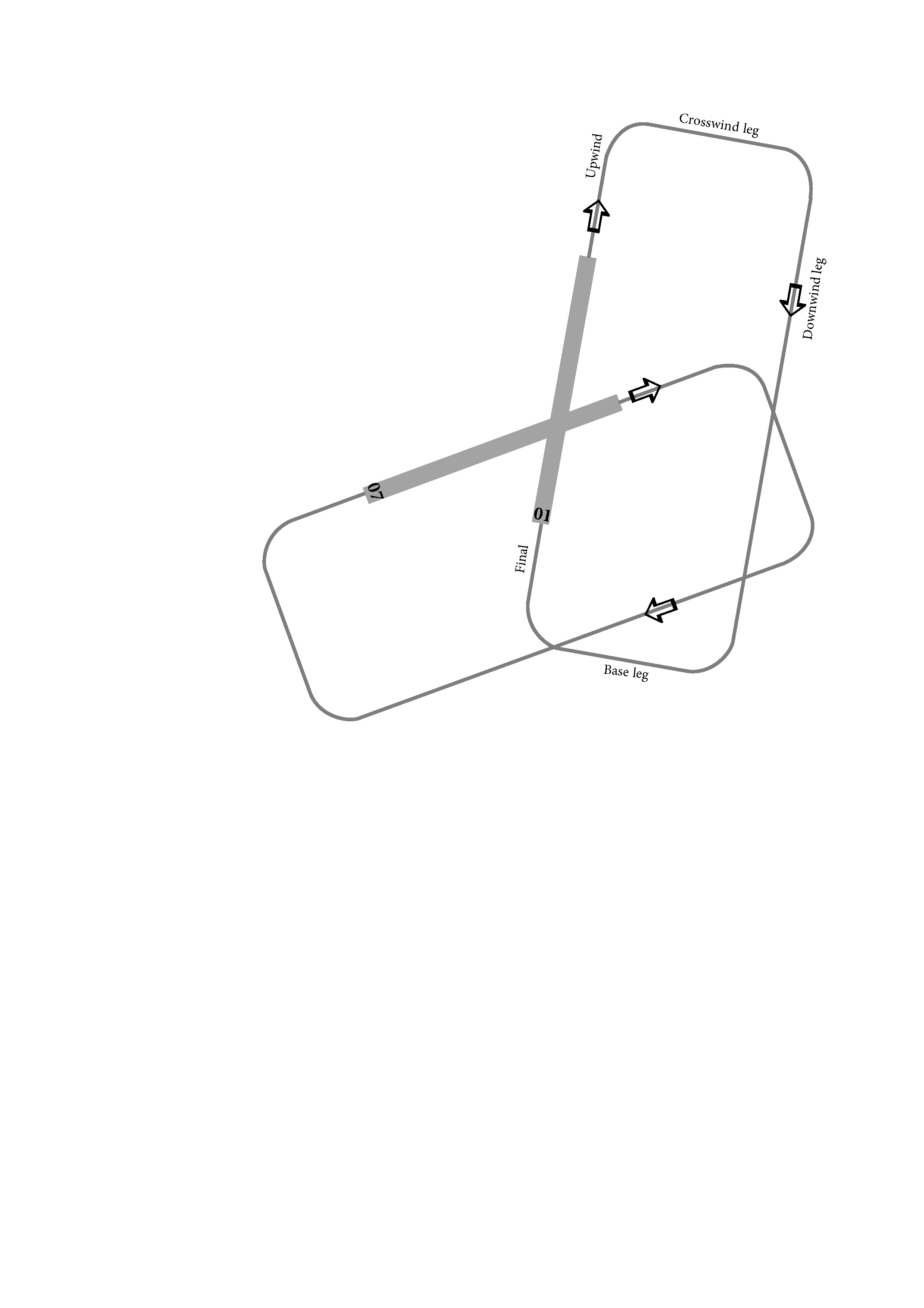
As the crosswind on runway 01 was up to 15 kt, PFU was conducting circuits on runway 07. The pilot of the King Air was conducting circuits on runway 01 (Figure 2). Both aircraft were conducting right-hand circuits, which maintained them to the east and south of Townsville Airport. To manage the sequence between the two aircraft, and to facilitate the other traffic operating within the area, the tower controller issued instructions at different times to extend various legs of the circuit. The mix of traffic under the tower controller’s jurisdiction resulted in a high workload and a high level of radio transmissions on the tower frequency.
Figure 2: Diagram showing the legs of a circuit
Source: ATSB
The CH‑47, which was operating in the circuit to the helipad to the west of the airfield, had earlier entered the circuit area via Kissing Point. The pilot of that CH-47 was advised of PFU by the tower controller on two occasions; at 1447 and at 1452. The call signs of that CH-47, which was operating to the west of the airfield, and the occurrence CH‑47 that was tracking for Kissing Point, contained the same root word with numbers that differed by one digit – Brahman 104 and Brahman 106 respectively.
At 1500, the tower controller acknowledged the first call by the flight crew of the occurrence CH‑47, when the aircraft was about 7.5 NM (14 km) to the east. No information on the traffic in the circuit area was provided to the flight crew of the occurrence CH‑47, or to any aircraft in the circuit on the occurrence CH‑47. At that time:
PFU was on final for runway 07
the King Air was late downwind for runway 01
the R22 was at the southern circuit boundary
the CH‑47 operating to the helipad to the west of the airport was on the ground awaiting clearance to become airborne
the MD500 was about to land at Townsville
the two Black Hawk helicopters were about 8 NM (15 km) to the south-east.
Between then and the next transmission from the flight crew of the occurrence CH‑47 to the tower controller at about 1503, there were 21 separate radio transmissions involving the tower controller and other aircraft. The second transmission from the flight crew, advising that the occurrence CH‑47 was approaching Kissing Point (Figure 1), was not acknowledged by the tower controller who then cleared the King Air to conduct a touch-and-go landing,[5] and provided tracking instructions to the crew of the R22. At this time:
the occurrence CH‑47 was about 4.5 NM (8 km) to the east
PFU was about 1.5 NM (3 km) upwind for runway 07
the King Air was about 1.5 NM (3 km) final for runway 01
the R22 was about 4 NM (7 km) to the south
the CH‑47 operating to helipad to the west of the airfield was still on the ground awaiting clearance to become airborne
the MD500 had landed
the two Black Hawk helicopters were about 4.5 NM (8 km) to the south-east.
Forty-nine seconds later, the flight crew of the occurrence CH‑47 reported at Kissing Point and advised the tower controller that there was another aircraft in their vicinity. Surveillance data shows that, at that time, the occurrence CH‑47 entered a left turn towards the coastline, before reversing to the right and away from the coast and PFU.
Seeing that the occurrence CH‑47 had commenced a turn away from the PFU’s track, the tower controller did not provide traffic on PFU to the crew of the occurrence CH-47 but, instead provided traffic on the King Air, as the crew of the occurrence CH‑47 had to sight and pass behind that aircraft before it could track towards the airfield. Traffic on the occurrence CH‑47 was also not passed to the flight crew of PFU.
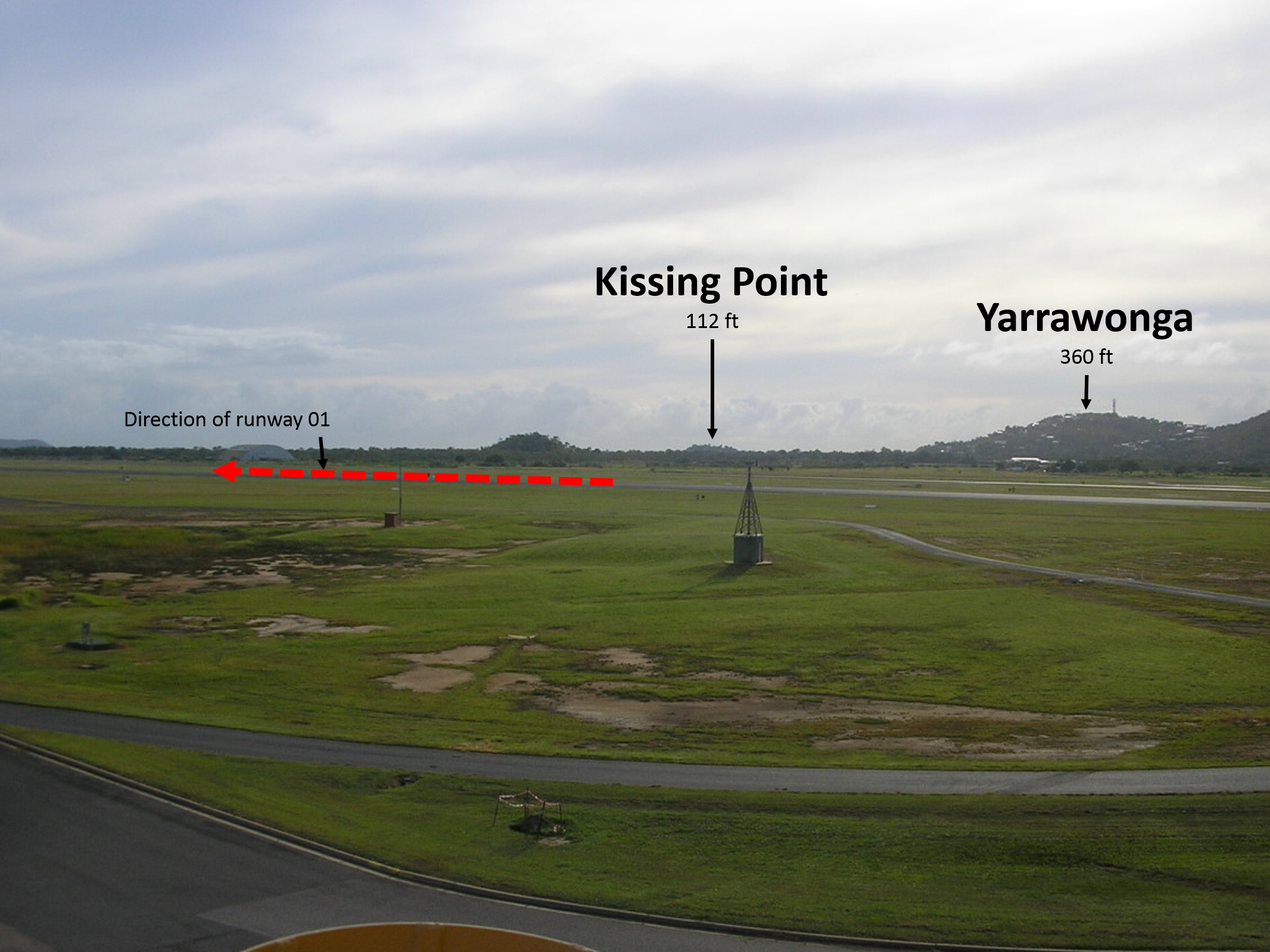
Of note, due to the topography to the east and north-east of the airport (Figure 3), and the operating height of the helicopter, the tower controller was unable to see the occurrence CH‑47 until just prior to its arrival at Kissing Point. This was the first time the tower controller was aware that the occurrence CH‑47 had an external load, requiring the controller to amend their traffic plan. The plan had been for the aircraft to track south of the airfield and fly over the city of Townsville, then to cross the upwind centreline of runway 01. With an external load, the aircraft was required to track to the west of the airport to a helipad just to the north of runway 07. This kept the occurrence CH‑47 away from built-up areas.
Figure 3: The tower controller’s view east-north-east towards Kissing Point, including relevant terrain height and the direction of runway 01
Source: Defence, modified by the ATSB
The crew of the occurrence CH‑47 subsequently sighted the King Air and tracked behind that aircraft, then to the west of the airfield for the helipad. The flight crew of PFU continued tracking upwind until advised by the tower controller to make a right circuit for runway 07.
When the flight crew of the occurrence CH‑47 first reported sighting PFU, surveillance data indicated that their aircraft and PFU were at the same altitude and separated by about 0.5 NM (1 km). However, the flight crew of the occurrence CH‑47 later reported that separation reduced to about 300 m and that, until they commenced the right turn, a collision risk had existed. The flight crew of PFU later reported that they saw the occurrence CH‑47 shortly after becoming airborne from runway 07, at a distance of 2 or 3 NM (4 or 6 km). They believed that:
at no stage did the occurrence CH‑47 come close enough to warrant anything but monitoring
The sources of information during the investigation included the:
Department of Defence
air traffic controllers involved in the incident
flight crew of VH-PFU
flight crew of the occurrence Boeing CH‑47 Chinook helicopter.
References
Arthur, W Bennett, W Stanush, PL & McNelly, TL 1998, Factors that influence skill decay and retention: A quantitative review and analysis, Human Performance, vol. 11, pp. 57–101.
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Department of Defence, the Civil Aviation Safety Authority, the air traffic controllers involved in the occurrence, the operator of VH-PFU and the flight crews of the occurrence Boeing CH‑47 Chinook helicopter and of VH‑PFU.
Submissions were received from the Department of Defence and the Civil Aviation Safety Authority. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Safety issues and actions
The safety issues identified during this investigation are listed in the Findings and Safety issues and actions sections of this report. The ATSB expects that all safety issues identified by the investigation should be addressed by the relevant organisation(s). In addressing those issues, the ATSB prefers to encourage relevant organisation(s) to proactively initiate safety action, rather than to issue formal safety recommendations or safety advisory notices.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are repeated separately on the ATSB website to facilitate monitoring by interested parties. Where relevant the safety issues and actions will be updated on the ATSB website as information comes to hand.
Compromised separation recovery training
Compromised separation recovery training deficiencies existed within the Department of Defence at the time of the occurrence, increasing the risk of inappropriate management of aircraft in close proximity.
Note: This safety issue was identified as part of ATSB investigation AO-2012-131 as safety issue AO-2012-131-SI-05 and resulted in the ATSB issuing safety recommendation AO‑2012‑131‑SR‑042 on 2 October 2014 (after the date of this occurrence at Townsville). The information below is a summary of the action taken by the Department of Defence (Defence) at that time. That action resulted in the ATSB determining that, overall, the safety action by Defence adequately addressed safety issue AO-2012-131-SI-05.
From the evidence available, the following findings are made with respect to the air traffic control information error involving a Department of Defence Boeing CH‑47 Chinook helicopter and a Cessna Aircraft Company 172S, registered VH‑PFU, near Townsville Airport, Queensland on 27 May 2014. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
Due to the busy environment, and possibly the similarity between two Boeing CH‑47 Chinook helicopter call signs, the controller did not pass mutual traffic and was not monitoring the occurrence helicopter and the Cessna Aircraft Company 172S in case of a proximity event.
The tower controller and tower supervisor assessed that, as the occurrence Boeing CH‑47 Chinook helicopter flight crew had identified the Cessna Aircraft Company 172S in proximity and had initiated a turn away, the proximity event was resolved. This meant that the flight crew of the two aircraft had to determine their own actions based solely on their observation of the other aircraft.
Other factors that increased risk
Compromised separation recovery training deficiencies existed within the Department of Defence at the time of the occurrence, increasing the risk of inappropriate management of aircraft in close proximity. [Safety issue]
Helicopter flight crews were not required to advise the tower controllers of the carriage of external loads that prevented them flying over built-up areas. This reduced the controller’s situation awareness and reduced the time available to develop an appropriate traffic management plan.
The location of the Kissing Point clearance limit within the Townsville circuit area increased the risk of an aircraft holding at that position coming into proximity with aircraft operating in the circuit.
Safety analysis
Introduction
An air traffic control information error at Townsville Airport, Queensland, on 27 May 2014 involved a Department of Defence (Defence) Boeing CH-47 Chinook (the occurrence CH-47), and a Cessna 172 registered VH-PFU (PFU). The information error positioned the two aircraft in close proximity in the circuit area, without the provision of relevant traffic information.
This analysis discusses the relevant controller actions, local conditions and relevant risk controls in place at Townsville Airport at the time of the occurrence.
Traffic not passed
The number of aircraft on the tower controller’s frequency, the mix of operation types and the locations of those operations resulted in a high workload for the tower controller and tower supervisor. The tower controller reported that their workload was more than they could handle and that they asked the supervisor for assistance. The supervisor provided assistance by conducting the necessary coordination and assisting with sequencing. However, the efforts to reduce the workload, including holding aircraft on the ground and not accepting additional inbound aircraft, were not sufficient and workload remained high.
The occurrence CH‑47 was about 7.5 NM (14 km) to the east when the flight crew first contacted the tower controller. PFU was on final for runway 07. As a result, neither flight crew would have been able to sight the other. However, both flight crew were familiar with the circuit traffic pattern on runway 07, and how helicopters tracked coastal via Kissing Point. Therefore, the provision of traffic at that time would have alerted both flight crew to the presence of the other aircraft in the circuit area, and of their intentions. Of note, during this period the tower controller’s workload was high, providing tracking instructions to numerous aircraft.
The provision of traffic when the occurrence CH‑47 contacted the tower controller a second time when approaching Kissing Point, with the occurrence CH‑47 about 4.5 NM (8 km) to the east of the airfield and about 3 NM (6 km) east of PFU at that time, would have increased the likelihood of the flight crews sighting each other. The flight crew of PFU later reported that they saw the occurrence CH‑47 shortly after becoming airborne from runway 07, though they did not advise the tower controller as they were aware of the controller’s high workload at the time.
The tower controller had passed traffic to flight crews in the lead-up to this occurrence, demonstrating that they were aware of the requirement to pass traffic and of the content of traffic information. More relevant in this instance, the controller had passed mutual traffic to the flight crew of PFU and the previous CH‑47 tracking via Kissing Point. The Defence investigation into this occurrence found that the tower controller did not realise that mutual traffic had not been passed to the flight crews of the occurrence CH‑47 and PFU. The similarity in the call signs of the previous CH‑47 and the occurrence CH‑47 may have influenced the tower controller into thinking that they had passed the required traffic information.
A controller’s first priority is to separate aircraft, and then to provide traffic information. At the time the flight crew of the occurrence CH‑47 reported approaching Kissing Point, the Defence Beechcraft King Air 350 (King Air) was on about 1.5 NM (3 km) final for runway 01, awaiting a clearance for a touch-and-go landing. Also, the tower controller needed to provide tracking instructions to the flight crew of a Robinson Helicopter Co R22 that was about 4 NM (7 km) south of the airport. Additionally, a transmission from the flight crew of one of the two Defence Sikorsky Black Hawk helicopters (Black Hawk) to the south of the airport may have been sufficient to interrupt the tower controller’s activities. This would explain the controller responding to the flight crew of the Black Hawk, instead of passing traffic to the flight crews of the occurrence CH‑47 and PFU. This likely resulted in the tower controller losing awareness of the need to pass traffic to these aircraft.
If the tower controller had passed mutual traffic to the flight crews of the occurrence CH‑47 and PFU prior to the occurrence CH‑47 arriving at Kissing Point, both flight crew would have been better able to manage their flight paths in relation to the other. Additionally, had the traffic information been passed earlier, the King Air would have been the only 'relevant' traffic for the flight crew of the occurrence CH‑47 when at Kissing Point.
In this occurrence, it is likely that the tower controller’s high workload resulted in a need for increased monitoring. This would likely have further added to their workload and, in combination with the large number of radio calls during this time, impacted on their ability to manage the traffic.
Management of the proximity event
The report by the flight crew of the occurrence CH‑47 that there was an aircraft in proximity when they arrived at Kissing Point should have been a sufficient trigger to the tower controller that traffic on PFU had not been provided. However, as the controller was now aware that the flight crew of the occurrence CH‑47 had PFU in sight, and the controller could see that the occurrence CH‑47 had commenced a right turn away from the flight path of PFU, the controller deemed that traffic information was not required and that the proximity risk had been resolved. But, the flight crew of the occurrence CH‑47 were not aware of the intentions of the flight crew of PFU. Equally, the tower controller did not know if the flight crew of PFU had seen, and were monitoring the occurrence CH‑47. The flight crew of the two aircraft determined their own actions based solely on what they could observe of the other aircraft.
Compromised separation recovery training
A conflict occurs when the distance between aircraft, as well as their relative positions and speed, may compromise the safety of the aircraft. On recognising such a situation, the controller is required to issue a safety alert, unless the pilot of one aircraft advises that action is being taken to resolve the situation, or that the other aircraft is in sight. The tower controller reported that in this case, both aircraft were in sight and the controller and supervisor both assessed that, as the flight crew of the occurrence CH‑47 had reported PFU in sight and turned away, the safety of neither aircraft was compromised.
At the time of the occurrence, compromised separation recovery training deficiencies had been identified and were being addressed within Defence. Though there is insufficient evidence that these deficiencies played a part in this occurrence, such training is an important defence against loss of separation and near-collision situations.
Advance knowledge of external load operations
Defence helicopter documentation for operations at Townsville Airport stipulated that, when operating with external loads, the helicopter should be flown clear of built-up or populated areas. Specifically, flight over people, buildings, vehicles or items of value must only occur if totally unavoidable. These precautions mitigated the risk of injury or damage in the event of accidental or emergency load release. In the context of the Townsville circuit area, these operating requirements meant that Defence helicopters carrying out external load operations were to track coastal until north-west of the extended centreline of runway 01, then along the western side of the airport to one of a number of helipads.
Though the tower controller and tower supervisor were aware of these requirements, until the tower controller sighted the occurrence CH‑47 approaching Kissing Point, they were not aware that it had an external load. The intended traffic sequence required the occurrence CH‑47 to track from Kissing Point south to right base for runway 01, then across runway 01 to land on the helipad just north of runway 07. On sighting the occurrence CH‑47 carrying an external load, the tower controller’s traffic plan had to be amended to track the helicopter away from built-up areas.
A documented procedure that required helicopter crews to advise air traffic control that they were carrying an external load, which could restrict manoeuvring, would result in better situation awareness for tower controllers and better inform their traffic management planning. In this occurrence, such additional information would likely have precluded the need for the tower controller to rapidly re-assess the disposition of the circuit traffic and to require the occurrence CH‑47 to sight and pass behind the King Air.
Kissing Point as a clearance limit
The Defence Townsville documentation that stipulated Kissing Point as a clearance limit was a form of strategic separation assurance. However, Kissing Point is located within the 5 NM (9 km) circuit area on the extended centreline of runway 07 (see Figure 1), 3 NM (6 km) east of Townsville. A standard clearance limit located further from Townsville would have provided better separation assurance between joining aircraft and those in the circuit area.
Though there was no evidence that a clearance limit further from Townsville would have avoided this proximity event, the controller is only part of a wider system designed to provide for safe aviation operations. A well-designed system should include strategic separation assurance that supports the controller. This could include holding aircraft in locations away from known high traffic areas, where the absence of one component (in this case the provision of mutual traffic) does not result in a compromised safety system.
Purpose of safety investigations & publishing information
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
The pilot of a Piper PA‑34 aircraft, registered VH-FEJ (FEJ), submitted a flight plan from Archerfield to Cairns via Townsville, Queensland. Prior to departure, air traffic control (ATC) at Archerfield updated the flight plan from visual flight rules (VFR) to instrument flight rules (IFR) at the pilot’s request.
The updated flight plan was transmitted via a change message to the various ATC agencies responsible for the aircraft. Townsville ATC, operated by the Department of Defence, utilised computer printed flight progress strips (strips) and the strip for FEJ was printed prior to the change message being processed, indicating that FEJ was a VFR flight.
When the pilot of FEJ contacted Townsville Approach, he requested a runway 01 instrument landing system approach. The Approach controller cleared the aircraft to track direct to the initial approach fix and, once the aircraft was within 36 NM, cleared the pilot of FEJ to descend to 4,000 ft.
Shortly after, the Approach controller became concerned about FEJ maintaining visual meteorological conditions given the weather in the area and queried the pilot on the aircraft’s flight category. On being advised that FEJ was an IFR flight and in cloud, the Approach controller immediately instructed the pilot to stop the descent at 5,500 ft. By the time the pilot was able to arrest the aircraft’s descent, FEJ had reached 5,200 ft. Though FEJ did not descend below the lowest safe altitude on the aircraft’s track, terrain clearance on track was not assured until FEJ climbed back to 5,500 ft. Shortly after, the pilot became visual and FEJ landed without further incident.
As a result of this occurrence, the Department of Defence has advised the ATSB that controllers are now required to check flight progress strips thoroughly prior to passing them to Approach, ensuring that the data was correct.
At about 0349 Eastern Daylight-saving Time, the Melbourne aerodrome controller cleared an Emirates Airlines, Boeing Company 777-31H/ER aircraft registered A6-EGG for take-off on runway 16.
The crew believed that the runway lights were on a low setting and conducted the take-off. Once airborne the pilots advised the approach controller that they believed that the lights were on a low intensity. A subsequent check of the airport lighting system revealed that runway 16 lights were turned off.
Had the crew queried the status of the runway lights, the aerodrome controller would have been able to identify that they had not been turned on as believed and corrected the situation.
This incident highlights the potential hazards associated with skill based human error and the need for increased vigilance when working in isolation in a safety critical environment.
Airservices Australia, advised the ATSB that they were in the process of standardising the operation of runway lighting controls at Towers and would propagate a national ATC instruction pending the related change effective 28 June 2012.
On 25 February 2010, a Piper Aircraft Corp Chieftain PA-31-350 aircraft, registered VH-BCQ, was being operated on a charter passenger flight from Mackay to Clermont Aerodrome, Queensland. Unable to land at either Clermont or the planned alternate aerodrome of Mackay due to deteriorating weather conditions, the flight diverted to Proserpine/Whitsunday Coast Aerodrome.
The pilot in command requested air traffic services (ATS) to arrange for a person to be on the ground at Proserpine/Whitsunday Aerodrome to ensure that the aerodrome lighting would be on for their arrival. This request was not actioned, but ATS provided the crew with a frequency for the pilot activated lighting system at the aerodrome. However, that frequency was decommissioned 10 days earlier, and a new frequency introduced.
On approach to Proserpine, the flight crew were unable to activate the aerodrome lighting. With critical fuel, and given weather considerations, the flight crew landed the aircraft without runway lighting at around 1957 Eastern Standard Time.
The investigation identified two minor safety issues; one relating to the practices used within the air traffic control group for the effective review and communication of notices to airmen, and the other the risk of out-of-date operational documentation.
The air navigation service provider advised that in response to this occurrence, it will conduct an internal education program to highlight the effect on safety when relevant information is not considered appropriately or reviewed before being provided to pilots.
The incorrect operational documentation has since been updated and the regional council managing Proserpine Aerodrome has instigated safety action relevant to their organisation.
Preliminary investigation was undertaken into a category 4
occurrence involving a Cessna 310R aircraft that had been issued a
clearance to cross runway 06 at Jandakot Airport while a Cessna
Citation 550 aircraft was on final approach to land. The Citation
had been issued a landing clearance. The ATSB has terminated the
investigation based on information from Airservices Australia that
there had been an inadvertent omission by the controller in
following an established check procedure. There was relatively
little safety benefit to be gained from continuing the
investigation compared with other priorities.
Status: Downgraded the occurrence to category 5
and investigation discontinued.