Entry to a closed taxiway involving Pilatus PC-12/47E, VH-FXJ, Adelaide Airport, South Australia, on 4 November 2024
Final report
Report release date: 24/06/2025
Investigation summary
What happened
On 4 November 2024, a Pilatus Aircraft PC-12/47E, registered VH-FXJ, and operated by the Royal Flying Doctor Service as Flydoc 543, taxied for departure at Adelaide Airport to conduct a medical transport flight to Pinnaroo Airport, South Australia. On board were a pilot and a flight nurse.
During taxi, after being incorrectly cleared to enter a NOTAMed closed section of taxiway, the pilot did not question the clearance, and the aircraft entered the taxiway and struck an unserviceability light used to identify the closed section. The pilot then continued with the departure.
There was no damage to the aircraft and no injuries as a result of this incident.
What the ATSB found
The ATSB found that, although both the air traffic controller and pilot were aware that the taxiway was closed, the aircraft was cleared and entered the area and consequently struck the light. Additionally, while there were indications via radio transmissions that an unserviceability light had been damaged, the pilot incorrectly assessed that the aircraft had not struck it and continued the flight without an inspection.
The ATSB also found that the lighting used to identify the entrance to the closed taxiway was insufficient to draw the pilot’s attention and the markers, required by the method of working plan, had not been used. In addition, the method of working plan, while stating that the closed area needed to be defined in accordance with the Civil Aviation Safety Regulations (CASR) Part 139 (Aerodromes) Manual of Standards 2019 (MOS), did not specify how many lights were required to denote the closed area.
In addition, the ATSB identified The Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019 section relating to the temporary closure of a taxiway at night did not:
- provide a recommendation that when operating on an aerodrome with significant obscuring background lighting, consideration be given to increasing the span of unserviceability lights, similar to the recommendation provided for markers to cross the entire closed area
- specify that both markers and unserviceability lights were required.
What has been done as a result
CASA is currently writing Advisory Circular (AC) 139.C-15 v1.0 - Safe planning and conduct for aerodrome works and has undertaken to include guidance on the use of both unserviceability cones and lights to designate closed taxiways at night. That guidance will include consideration of the detrimental effect background lighting can have on identifying closed infrastructure.
As a result of this incident, Airservices Australia released a standardised directive to Adelaide Tower air traffic controllers to clarify the occurrence management and reporting requirements following this incident. Operational command authority escalation was added to the Airservices focus area questions for initial and renewal assessments completed in October 2024.
Safety message
This incident highlights the importance of effective communication and potential for expectation bias. If flight crews receive a clearance that contradicts a NOTAM or current ATIS information, they should question the clearance before continuing.
Additionally, although the CASR Part 139 MOS did not specify a minimum number of lights to identify closed ground movement areas, it did state they should be identified as clearly as possible. When considering the adequacy of unserviceability lighting, operators should consider any obscuring background lighting and consider increasing the span of lighting if required.
Finally, if there is a possibility that an object has been struck by an aircraft, it should be checked for damage before continued flight.
The occurrence
On 4 November 2024, a Pilatus Aircraft PC-12/47E, registered VH-FXJ and operated by the Royal Flying Doctor Service as Flydoc 543, taxied for departure at Adelaide Airport to conduct a medical transport flight to Pinnaroo Airport, South Australia. On board the aircraft were a pilot and a flight nurse.
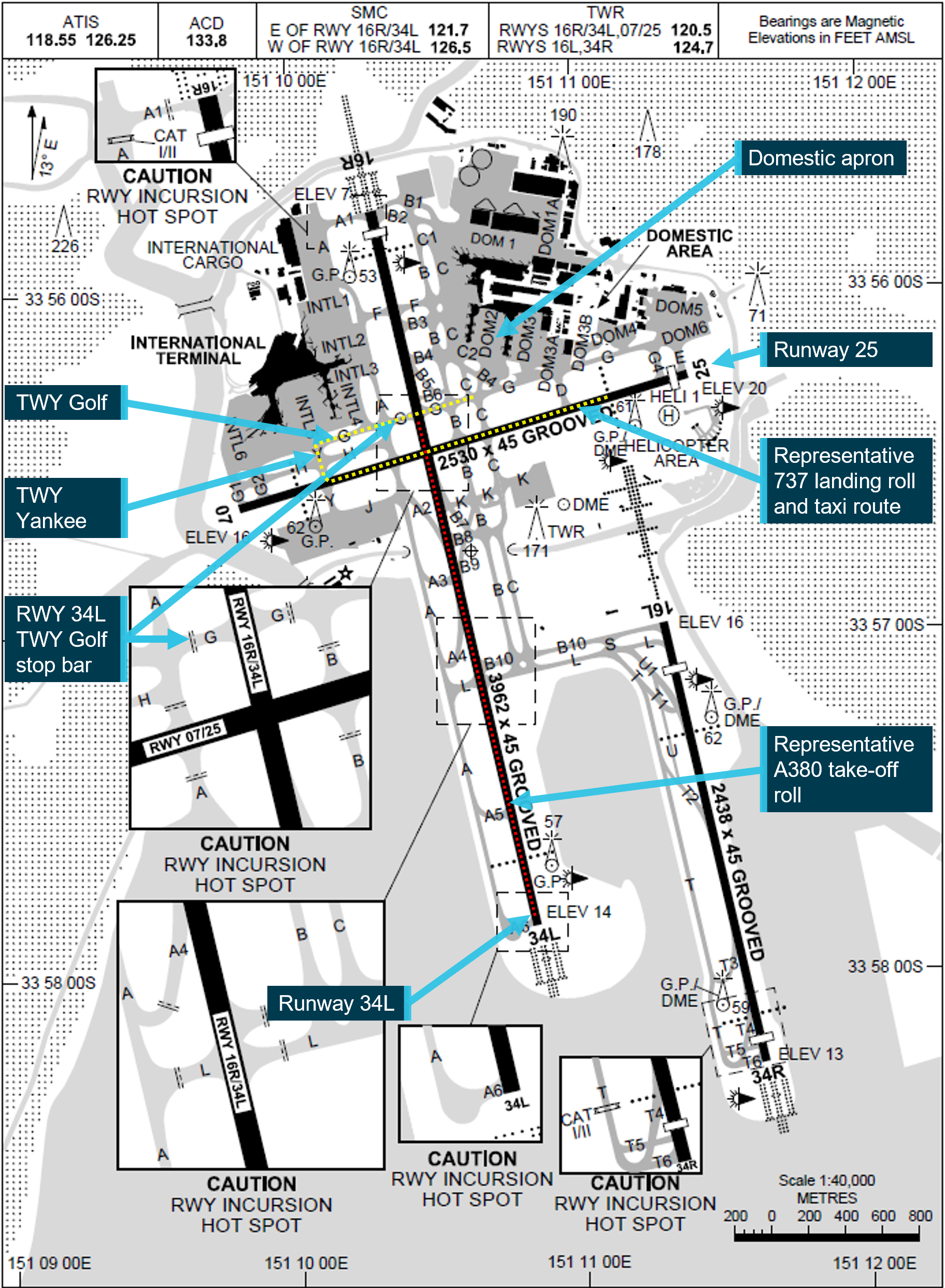
At the time of departure there was an active NOTAM[1] for multiple taxiway closures, including an area on taxiway A6 between taxiway K and holding point B2, due to work in progress on the grass beside the taxiway (Figure 1). The same information was broadcast on the Adelaide ATIS.[2] The closed section of taxiway was marked as unserviceable by 3 red lights across the taxiway at multiple entrances to the taxiway. The pilot reported being aware of the taxiway closures.
This was the pilot’s second flight from Adelaide during their duty period that night. On the first flight, the pilot had received the expected taxi clearance from the Adelaide ground air traffic service operator (controller) to taxi via taxiway D1, before entering and backtracking runway 23.[3] This taxi clearance avoided the unserviceable areas of the taxiway.
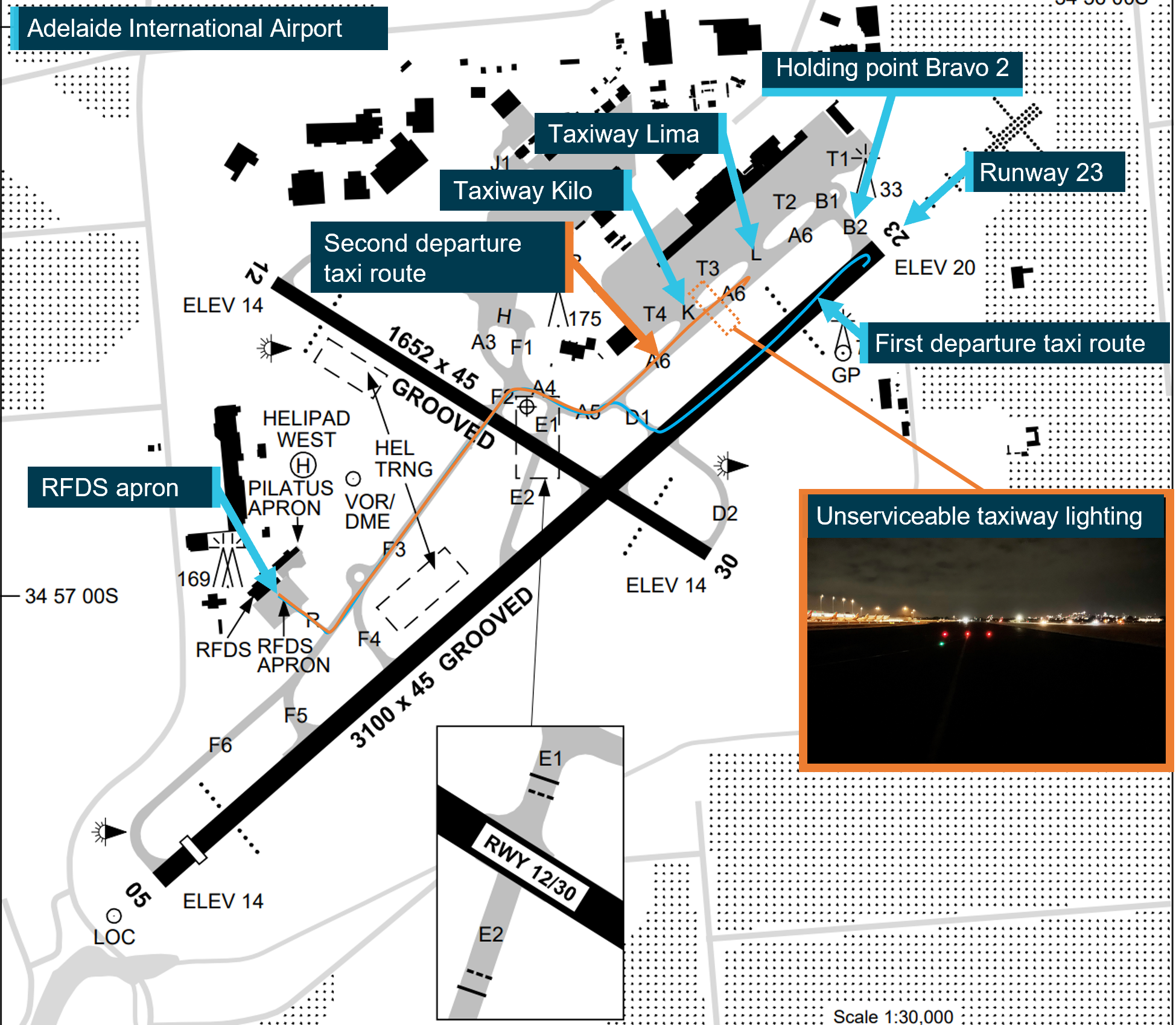
The image shows both taxi routes taken by Flydoc 543 and the position of the unserviceable taxiway lights. The blue line is the taxi route for the first flight, the orange line is the taxi route for the incident flight. The view of the unserviceable taxiway lights was taken on 14 November 2024. It is an exemplar image of the lights on the night the incident took place. Source: Airservices Australia, Adelaide Airport, and Flightradar24; annotated by the ATSB
At 0309, the pilot taxied for departure on the incident flight. They expected to receive the same taxi clearance for the planned departure on runway 23. However, the clearance received was:
Flydoc 543 on Foxtrot cross runway 12 taxi holding point Bravo 2 runway 23.
This clearance required the aircraft to taxi through the unserviceable area. The pilot did not question the clearance, assuming that the works had ended early.
The pilot later reported that they did not detect the red lights across the taxiway. As they entered the closed section, unknown to the pilot, the aircraft most likely struck the centre unserviceability light. Shortly after, the controller advised the pilot they had entered the closed taxiway and requested they stop and conduct a 180° turn:
…Flydoc 543 that taxiway’s closed, apologies, can you do a 180 there?
A works safety officer, in a nearby aerodrome safety car, offered to remove the red lights on the taxiway before the aircraft taxied back through them. When they entered the taxiway, they detected debris and advised the controller via the ground radio frequency that this would need to be removed:
Adelaide Ground, Works 60, there is debris on taxiway, sorry taxiway Alpha 6 from the red light, I just need a moment to pick that up…
advising a short time later:
Adelaide Ground, Works 60, the debris has been picked up as well as the red lights on Alpha 6.
The controller then asked the pilot if they wished to continue and, after confirming with the flight nurse that they had not felt anything, the pilot advised the controller that they would continue with the departure.
After the operator was advised of the incident the aircraft was grounded, pending an inspection. The post-incident inspection found no damage to the aircraft associated with striking the taxiway light. There were no injuries.
Context
Aircraft information
VH-FXJ was a Pilatus Aircraft PC-12/47E which was manufactured in 2015 and issued serial number 1541. On 10 August 2015, it was registered in Australia with the operator. It was powered by a Pratt & Whitney PT6A-67P turbine engine driving a four-bladed, variable-pitch Hartzell propeller.
Pilot information
The pilot held a commercial pilot licence (aeroplane), an instrument rating and a class 1 aviation medical certificate. They had about 6,375 hours of flight experience at the time of the incident. A total of 1,650 hours had been accrued in PC‑12 aircraft, of which 128 were in the previous 90 days.
The pilot later reported that, at the time of the occurrence, they were fully alert and wide awake. They had been on duty for 5 hours when the incident occurred and awake for approximately 6 hours. In the previous 48 hours, the pilot had received 18 hours of sleep.
They also stated that if they thought they had hit something, they would have returned to the apron to have the aircraft checked by maintenance personnel.
Adelaide Airport
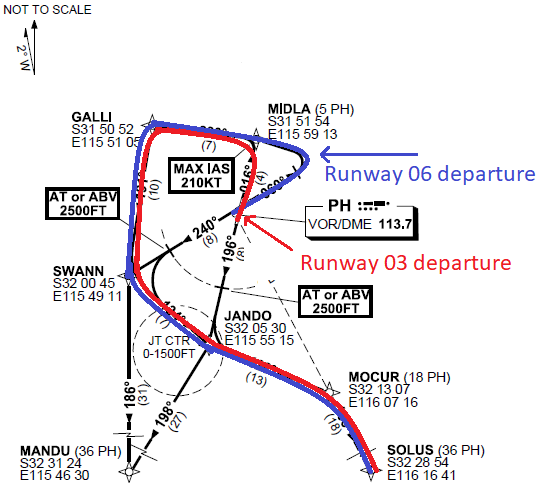
At the time of the incident, NOTAM C0661 was active at Adelaide Airport. It stated, from 3–9 November, between 2300 and 0600 local time, taxiway A6 north of taxiway K, taxiway B1, taxiway B2, taxiway L, and holding bay 23 were closed due to work in progress (Figure 2). This meant that an aircraft departing from runway 23, was required to enter the runway at taxiway D1 and backtrack on the runway to the threshold.
Figure 2: Method of working plan
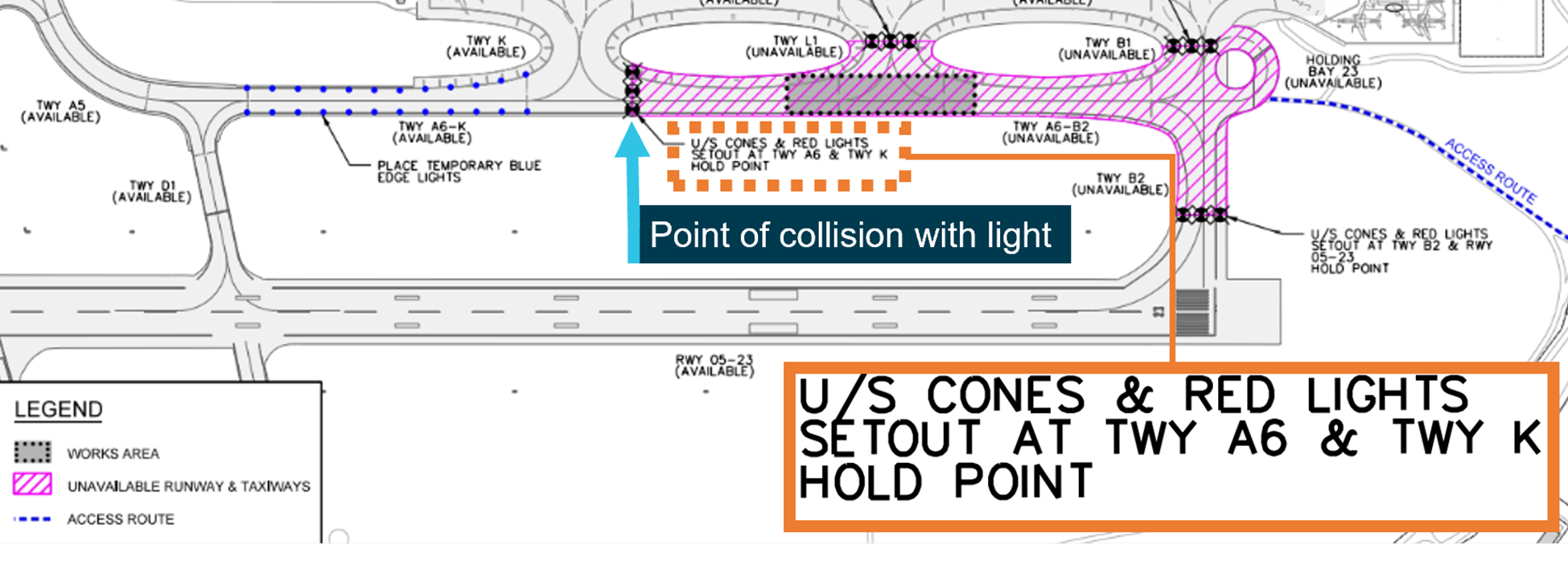
Source: Adelaide Airport, annotated by the ATSB
The NOTAM was accompanied by information on the ATIS that was broadcast from 0218 and valid at the time of departure. The ATIS stated that runway 23 was in use and taxiways B1, B2, L, A6 north of K, and the 23 holding bay were not available due to works.
The ATIS also stated the wind was from 200 degrees at 8 kt, visibility was greater than 10 km, temperature 16°C, and cloud cover was few[4] at 4,000 ft.
The method of working plan stated that the closed areas ‘will be defined by works limit markers in accordance with Civil Aviation Safety Authority Part 139 (Aerodromes) Manual of Standards’. The method of working plan required that both cones and lights were used and showed on a diagram where the works limit markers needed to be placed (Figure 2). However, it did not provide guidance regarding how many markers or lights should be used to identify the area.
Parts of the aircraft movement area that are unserviceable as a result of the works being carried out will be defined by unserviceability cones and red lights. These will be positioned as described below:
• Taxiway A6 – on the hold point to Taxiway K…
Adelaide Airport later advised the ATSB that 3 lights placed across the entrance to the taxiway, at 3 m intervals, was its standard practice. Additionally, the ATSB was informed that on the night of the incident the unserviceability cones, required by the method of working plan, had not been put in place, and this was its general practice for night works.
Taxiway A6 was approximately 35 m in width. The lights used were steady red lights and were designed to break into fragments when struck, minimising damage to aircraft.
Taxiway A also normally had green centreline taxi lights. While not outlined as a safety measure in the method of working plan, at the time of the incident, the green centreline taxi lights were extinguished in the closed section, to assist in identifying this area.
Air traffic control
The controller
The controller had been employed by Airservices Australia since 2005 and held the required ratings to provide air traffic services at Adelaide Airport. They held operational command authority (OCA), which designated them as the final decision-making authority within the tower when a tower supervisor was not available. They reported having previously completed night shifts as the only controller. In addition, they advised that there was a period of no aircraft movements prior to the pilot requesting taxi clearance, and during this period, they were completing company computer‑based training and felt alert and awake.
The controller also stated that, unless there was an emergency, the use of the runway for aircraft backtracking should be limited. They also stated that the operator required that their aircraft use the full runway length for departures. This meant, under normal circumstances, when runway 23 was in use, a taxi clearance would include taxi on A6 to holding point B2.
Further, the controller advised that there was no actual work being done to the taxiway, it was closed to provide clearance for the workers working on the grass adjacent to the taxiway. They stated that they did not think there would be anything on the taxiway that could damage the aircraft.
Airservices also advised that the controller had completed the following:
- assessment of renewal for its Adelaide tower endorsements – completed September 2024
- examination requirements for renewal of Adelaide tower endorsements – completed October 2024.
Airservices had identified OCA refresher training to be included in the financial year 2024/2025 mandatory training plan. However, at the time of the incident, the controller had not completed this training.
Airport communication facilities
Adelaide Airport’s control tower was operating at the time of the incident and was occupied by a single controller. Due to the low level of activity, the controller was operating as Adelaide Delivery (providing airway clearances), Adelaide Ground (providing surface movement and control), and Adelaide Tower (aerodrome controller). Although the positions operated on different frequencies, while the tower was occupied by a single controller, all communications were re-transmitted across all 3 frequencies.
Control tower systems
The integrated tower automation suite (INTAS) was in use by controllers at Adelaide Airport. The INTAS was capable of selecting a runway as closed. When activated, the INTAS workstation would highlight this on the status bar for the runway label, which changed the runway designator from grey (normal) to red. Additionally, an alert was also generated based on the runway status.
In the context of this occurrence, INTAS did not facilitate marking a taxiway as unserviceable or provide an alert if an aircraft was cleared onto an unserviceable taxiway.
The controller reported they were aware of the airport taxiway closures. As they had no available tools to mark a taxiway or region as restricted or closed, they had created a custom text box on their display to help remind them of the closure. The text box did not provide any visual change to the closed taxiway or provide an alert if an aircraft was cleared into the area.
Post-incident procedures
Regarding required action following an occurrence, the NAAM stated:
5.1.1.5 Relief from operational duty
Whenever practicable, relieve the ATSO[5] from operational duty following any potential ATS occurrence for which there may be an ATS attribution.
5.1.1.6 Risk assess continued operation
If the ATSO cannot be relieved from operational duty following a potential ATS occurrence, conduct a risk assessment to determine if the affected ATSO can continue operational duties.
If there is any degree of, or doubt about, ATS attribution and the ATSO will continue duty, record the outcome of the risk assessment in the ATS Risk Assessment and Management Record…
Post-incident actions
After the incident, the controller remained on duty and submitted an internal report and logged the incident in the tower’s physical logbook. The controller advised the ATSB that they were unaware that a risk assessment was required to be completed following an incident or that they were required to contact the Air Traffic Management Director, based in Melbourne.
At approximately 1030, after their scheduled shift was completed, the controller contacted the on-duty tower supervisor to ensure they were aware of the incident. They were then informed that their air traffic services approval had been temporarily withdrawn.
Airservices Australia later reported that if a risk assessment had been completed as soon as practicable after the incident occurred, the controller would probably have been found suitable to continue operation:
the risk assessment outcome would have likely resulted in the controller involved in the incident being able to remain on console with additional controls until the next scheduled controller arrived at 0530, had it been completed at the time.
The risk assessment controls likely would have focused on the following:
- welfare checks to ensure fatigue management
- assessment of the pending scheduled traffic.
Recorded data
Images
Several days after the incident, Adelaide Airport provided photographs of the unserviceability lights on taxiway A6, taken in similar conditions to those at the time of the incident. The images identified that the red unserviceability lights were difficult to see while on the southern end of taxiway A6 due to bright works lights beyond the unserviceable area (Figure 3). However they became more noticeable as the aircraft approached the closed area.
Figure 3: Approaching unserviceability lights
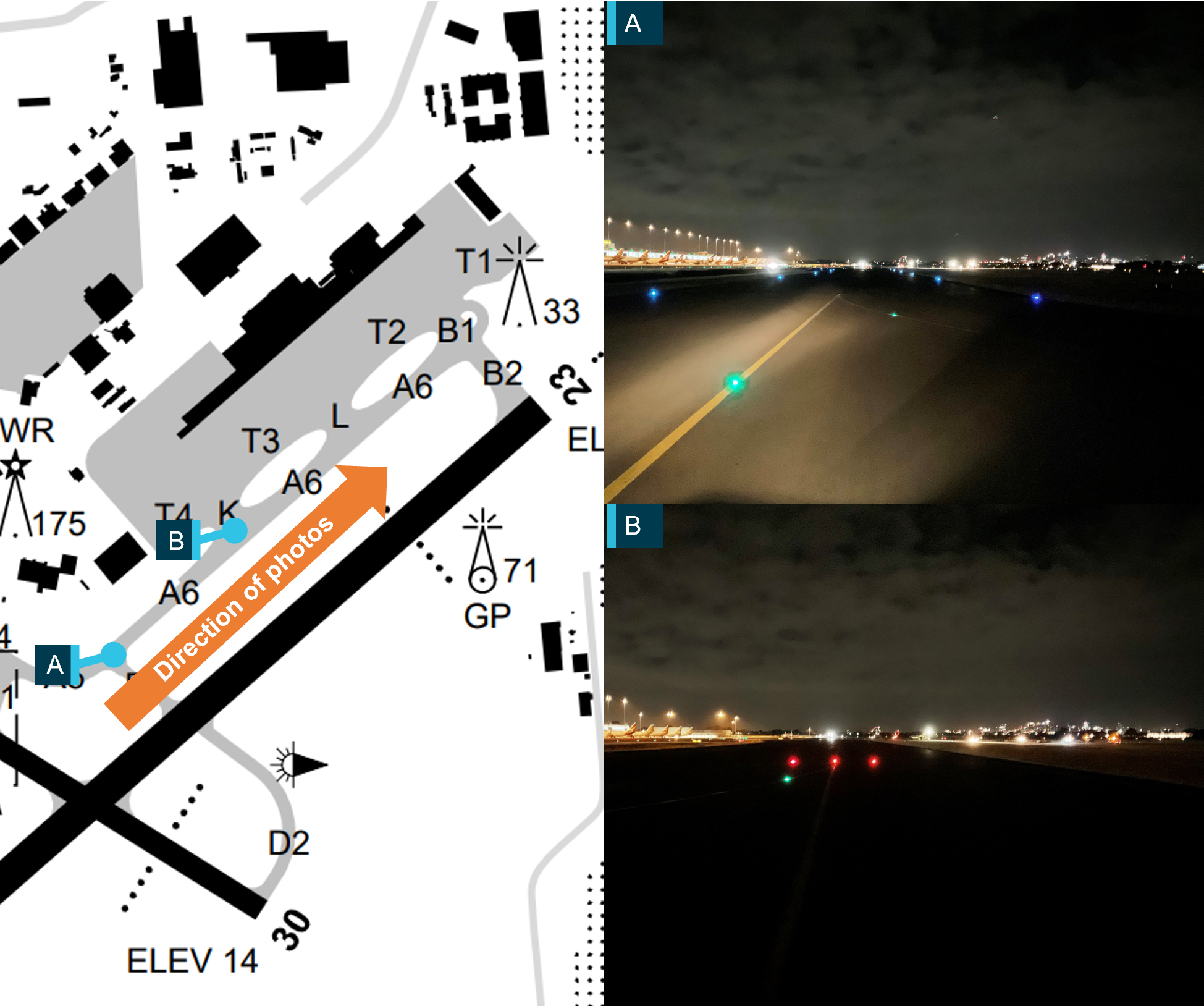
Image shown is an exemplar of the lighting on the night of the incident. The photo shown was taken several days after the incident occurred. Source: Adelaide Airport, annotated by the ATSB
Video imagery
Adelaide Airport also provided the ATSB with video footage of the incident. This showed the unserviceability lighting before and after the aircraft entered the area (Figure 4). It also showed that after completing a 180° turn and coming to a stop facing the 2 remaining red unserviceability lights, the aircraft remained stationary for approximately 4 minutes while ground personnel cleared the remaining lights and debris.
Figure 4: A6 unserviceability lighting before and after the occurrence
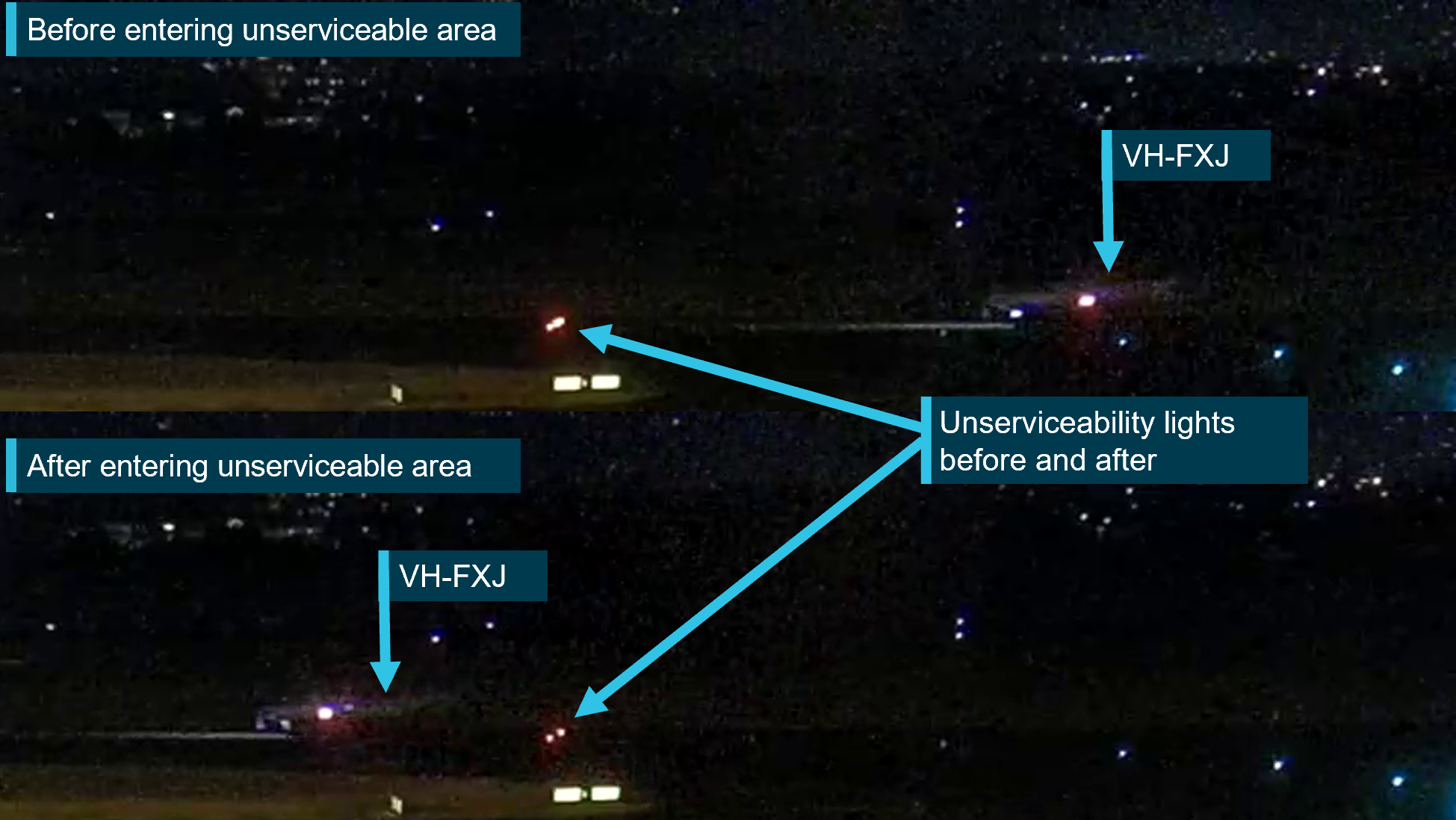
Source: Adelaide Airport, annotated by ATSB
Regulatory requirements
Unserviceability lights and markers
The Civil Aviation Safety Regulations (CASR) Part 139 (Aerodromes) Manual of Standards 2019 (MOS) Chapter 8 - Visual aids provided by aerodrome markings, markers, signals, signs, wind direction indicators etc stated:[6]
Division 2 - Markers
8.06 Introduction
(1) A marker must be lightweight and frangible…
8.108 Use of unserviceability markers…
(1) Unserviceability markers must consist of a white standard cone:
(a) with a horizontal red stripe 25 cm wide around its centre halfway up the cone so as to provide 3 bands of colour, namely, white-red-white
(2) Unserviceability markers must be placed at the entrance to, and across, any part of the movement area of an aerodrome (including a runway) that is not to be used by aircraft.
(3) At least 3 unserviceability markers must be displayed across the centreline of any portion of a taxiway, apron or holding bay that is unserviceable, whether or not it is possible for aircraft to safely taxi past the area that is unserviceable.
Note: CASA recommends that additional unserviceability markers be displayed, 3 m apart, continuously across the entire width of the runway, taxiway, apron or holding bay.
Regarding unserviceability lighting, Chapter 9 - Visual aids provided by aerodrome lighting Division 14 Works and unserviceable area lighting stated:
9.127 Lighting associated with closed and unserviceable areas
(1) If a runway or taxiway, or a portion of a runway or taxiway, is closed (a closed facility), all aerodrome lighting on the closed facility, and any visual aids leading a pilot into the closed facility, must be extinguished or obscured except the lighting for visual aids used to warn pilots of the closed facility.
(3) For a partial or complete closure of a manoeuvring area for less than 5 days, the aerodrome lights for the closed area must be:
(a) obscured with an opaque cover ….
(b) if not so obscured — electrically isolated or disabled to prevent their inadvertent activation.
9.131 Movement area access in the vicinity of unserviceable areas
(1) If a closed runway or taxiway, or a portion of a closed runway or taxiway (the closed area) is intersected by a runway or taxiway which is used at night, unserviceability lights must be placed across the entrance to the closed area at intervals not exceeding 3 m.
9.132 Characteristics of unserviceability lights
Unserviceability lights must:
(a) be steady red lights; and
(b) have:
(i) an intensity that is sufficient to ensure conspicuity considering the intensity of the adjacent lights and the general level of illumination against which they would normally be viewed; and
(ii) an average output of red main beam light not less than 10 cd.
CASA also later advised that markers and lights should be used at night to delineate an unserviceable area:
… the Part 139 MOS does not state that markers are only required during the day, therefore they are required at all times.
CASA also published Advisory Circular 139.C-09v1.0 - Visual Aids, Markings, Signals and Signs, which did not provide any further clarification for how to identify a temporary unserviceable taxiway. This AC advised that ‘Visual aids required for the management of works on the aerodrome are outside the scope of this AC and are addressed in AC 139.C-15 Safe planning and conduct of aerodrome works however, at the time of writing, AC 139.C-15 had not been published.
The International Civil Aviation Organization (ICAO) - Annex 14 Aerodromes section 7.1 Closed runways and taxiways or parts thereof subsection 7.1.1 provided the minimum standard for identifying a temporary closed taxiway, which stated that:
‘a closed marking shall be displayed on a runway or taxiway or portion thereof which is permanently closed to the use of all aircraft.’
7.1.3 stated that
‘…on a taxiway a closed marking shall be placed at least at each end of the taxiway or portion thereof closed.’
Note 1. — When an area is temporarily closed, frangible barriers or markings utilizing materials other than paint or other suitable means may be used to identify the closed area.
Annex 14 did not provide a definition of a frangible barrier.
In addition, 7.1.7 stated that:
In addition to closed markings, when the runway or taxiway or portion thereof closed is intercepted by a usable runway or taxiway which is used at night, unserviceability lights shall be placed across the entrance to the closed area at intervals not exceeding 3 m…
In section 7.4 Unserviceable areas subsection 7.4.1 stated
Unserviceability markers shall be displayed wherever any portion of a taxiway, apron or holding bay is unfit for the movement of aircraft but it is still possible for aircraft to bypass the area safely. On a movement area used at night, unserviceability lights shall be used.
Note 1.— Unserviceability markers and lights are used for such purposes as warning pilots of a hole in a taxiway or apron pavement or outlining a portion of pavement, such as on an apron, that is under repair. They are not suitable for use when a portion of a runway becomes unserviceable, nor on a taxiway when a major portion of the width becomes unserviceable. In such instances, the runway or taxiway is normally closed.
Safety analysis
Introduction
On the night of the incident, Adelaide Airport had temporary taxiway closures in place. These closures were broadcast on the ATIS and published in the Adelaide Airport NOTAMs. Although, both the pilot and the controller were aware of the temporary closures, the aircraft was cleared to and entered a temporary unserviceable area and collided with an unserviceability light, before proceeding to take-off.
Clearance to enter taxiway
Although, the occurrence time was early in the morning, the controller reported feeling alert. They were experienced in working as the sole controller in the tower and remained active by completing company computer-based training.
As the operator’s aircraft were required to use the full runway length for departure, it is likely that the controller gave the commonly-used taxi clearance, while momentarily forgetting about the taxiway closures. Furthermore, while the controller had created a custom text box on their display to help remind them of the closure, it was ineffective and there was no built-in alerting system if an aircraft was cleared onto the closed taxiway.
Contributing factor The controller issued a clearance for the aircraft to taxi through a temporarily closed movement area. |
Aircraft entered closed taxiway
The pilot was aware of the taxiway closures and planned their taxi route to avoid them. However, as they assumed the clearance indicated the works were no longer active, they did not question the clearance.
The pilot reported they did not see the red unserviceability lights before entering the closed section of taxiway and the aircraft struck one of the temporary lights.
Contributing factor On receipt of a clearance that required taxiing through a known temporarily closed area, the pilot did not question the clearance as they assumed the works had ceased. Additionally, they did not observe the identifying closure lights and, during entry to the closed movement area, the aircraft struck a temporary taxiway light. |
Insufficient lighting and markers to denote the closed area
Three lights had been placed across the closed section of taxiway which was 35 m wide. Photographs, taken along the taxiway, showed that with the background lighting, it was difficult to identify the lights, although they were more noticeable close to the closed section. In any event, the lighting in place on the night was insufficient to alert the pilot that the taxiway was still closed. In addition, the markers required to denote the unserviceable area, were not in position.
Contributing factor The lighting in place on the night was insufficient to draw the pilot's attention and avoid entering the temporary unserviceable area. Additionally, the required markers were not in place. |
Continued departure
The pilot was made aware they had entered an unserviceable taxiway, and they waited while the taxiway lights were removed prior to exiting the area. During that time, comments by the works safety officer that they were removing debris from a broken light was rebroadcast on all frequencies, including the one being used by the pilot.
While the controller did not specifically state that there was debris on the taxiway, they did question the pilot about if they wanted to continue. The pilot, after checking with the flight nurse whether they had felt anything, assessed the aircraft had not struck a light and continued the departure. Regardless of whether the aircraft struck the light, due to the possibility of damage, an inspection should have been completed prior to continued flight.
Other factor that increased risk Despite indications that an unserviceability light had been damaged by the aircraft, the pilot assessed that the aircraft had not struck it and continued the flight, without getting an inspection. |
Method of working plan
While the method of working plan stated that the closed movement areas needed to be marked in accordance with the Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019 (MOS) and showed where the markers were to be placed, it did not specify a minimum number to be used. As it was Adelaide Airport’s general practice not to use cones to identify night works, this did not contribute to this incident.
In addition, 3 symbols were used to represent the unserviceability markers and red lights. It is likely that this influenced the Adelaide Airport’s general practise to use 3 lights to identify temporary unserviceable areas, as was the case on the night of the occurrence.
Contributing factor Despite Adelaide Airport’s method of working plan stating that the markers used to identify the closed areas needed to comply with the Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019, it did not specify the number of unserviceability markers required. However, these were regularly not being used to denote the closed area at night. The plan also did not specify the number of lights to be used, and it was the general practise to use 3 red lights. This resulted in reduced prominence of unserviceable movement areas. |
Clarity of regulations
The Civil Aviation Safety Regulations (CASR) Part 139 (Aerodromes) Manual of Standards 2019 (MOS) stated that a minimum of 3 markers were required to denote a temporary unserviceable movement area and while not mandatory, it recommended that markers cover the entire width of the taxiway at 3 m spacing.
The requirements in the MOS for identifying a temporary closed taxiway during daylight hours exceeded the Annex 14 – Aerodromes requirements.
For night closures, the regulations stated that unserviceability lights needed to be placed across the entrance at 3 m spacing but did not recommend that the lights should cover the entire width. While CASA had a requirement for lights to have an intensity that was sufficient to ensure conspicuity against the background which they would normally be viewed, as was the case in this occurrence, background lighting at busy airports can make it difficult to detect unserviceability lights.
Increasing the span of unserviceability lights, in circumstances where there is significant obscuring background lighting, would make a closed area much more distinguishable. As done for the markers, a recommendation would encourage operators to consider their circumstances to assess the number of lights required to clearly identify the area.
In addition, CASA advised that as the MOS did not state that markers were only required during daylight, therefore, they were required at night. Although implied by the MOS, there was no statement that clarified that at night both unserviceability lights and markers were required. This explicit requirement was contained within the wording of Annex 14.
Contributing factor The Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019 section relating to the temporary closure of a taxiway at night did not:
|
Controller continued duty
After the incident took place, while the Air Traffic Service (ATS) controller entered an internal report and entered the incident into the physical tower logbook, they did not believe the incident required contacting the Air Traffic Management Director (ATMD), located in Melbourne. Although, the Airservices Australia’s records showed the controller had completed their annual renewal for the Adelaide tower endorsements, the controller reported they were unaware that a risk assessment was required for them to continue operating.
If contact had been made with the ATMD, the risk assessment would likely have found the controller suitable to continue operating, requiring extra welfare checks and an assessment of pending traffic.
As the risk assessment was not completed, the controller continued operations without additional risk controls in place.
Other finding Following the occurrence, the controller continued operating as the sole tower operator without completing the required risk assessment. If conducted, such an assessment would probably have resulted in the controller completing their duty period with additional risk controls in place. |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the entry to a closed taxiway involving Pilatus PC-12, VH-FXJ at Adelaide Airport, South Australia on 4 November 2024.
Contributing factors
- The controller issued a clearance for the aircraft to taxi through a temporarily closed movement area.
- On receipt of a clearance that required taxiing through a known temporarily closed area, the pilot did not question the clearance as they assumed the works had ceased. Additionally, they did not observe the identifying closure lights and, during entry to the closed movement area, the aircraft struck a temporary taxiway light.
- The lighting in place on the night was insufficient to draw the pilot's attention and avoid entering the temporary unserviceable area. Additionally, the required cone markers were not in place.
- Despite Adelaide Airport’s method of working plan stating that the markers used to identify the closed areas needed to comply with the Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019, it did not specify the number of unserviceability markers required. However, these were regularly not being used to denote the closed area at night. The plan also did not specify the number of lights to be used, and it was the general practise to use 3 red lights. This resulted in reduced prominence of unserviceable movement areas.
- The Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019 section relating to the temporary closure of a taxiway at night did not:
- provide a recommendation that when operating on an aerodrome with significant obscuring background lighting, consideration be given to increasing the span of unserviceability lights, similar to the recommendation provided for markers to cross the entire closed area
- specify that both markers and unserviceability lights were required. (Safety issue)
Other factors that increased risk
- Despite indications that an unserviceability light had been damaged by the aircraft, the pilot assessed that the aircraft had not struck it and continued the flight, without getting an inspection.
Other finding
Following the occurrence, the controller continued operating as the sole tower operator without completing the required risk assessment. If conducted, such an assessment would probably have resulted in the controller completing their duty period with additional risk controls in place.
Safety issues and actions
Temporary unserviceability lighting regulations
Safety issue number: AO-2024-061-SI-01
Safety issue description: The Civil Aviation Safety Regulations Part 139 (Aerodromes) Manual of Standards 2019 section relating to the temporary closure of a taxiway at night did not:
- provide a recommendation that when operating on an aerodrome with significant obscuring background lighting, consideration be given to increasing the span of unserviceability lights, similar to the recommendation provided for markers to cross the entire closed area
- specify that both markers and unserviceability lights were required.
Additional safety action taken by Airservices Australia
As a result of this incident, Airservices Australia released a standardised directive to Adelaide tower to clarify the occurrence management and reporting requirements following this incident. In addition, operational command authority escalation was added to the Airservices focus area questions for initial and renewal assessments completed in October 2024.
Glossary
| AC | Advisory Circular |
| ATMD | Air traffic management director |
| ATS | Air traffic services |
| ATIS | Automatic terminal information service |
| ATSO | Air traffic services officer |
| CASA | Civil Aviation Safety Authority |
| CASR | Civil Aviation Safety Regulations |
| ICAO | International Civil Aviation Organization |
| INTAS | Integrated tower automation suite |
| MOS | Manual of Standards |
| NAAM | National ATS administration manual |
| NOTAM | Notice to airman |
| OCA | Operational control authority |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot and operator
- the controller
- Civil Aviation Safety Authority
- International Civil Aviation Organisation
- Adelaide Airport
- Airservices Australia
- ADS-B flight data
- still and video imagery
- recorded communications.
References
- Civil Aviation Safety Regulations–Part 139 (Aerodromes) Manual of Standards 2019 (MOS)
- Civil Aviation Safety Regulation–Part 91
- International Civil Aviation Organization (ICAO) - Annex 14 Aerodromes
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the pilot and operator
- the controller
- Adelaide Airport
- Airservices Australia
- Civil Aviation Safety Authority
Submissions were received from:
- the operator
- Airservices Australia
- Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Notice to Airmen (NOTAM): a notice distributed by means of telecommunication containing information concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to personnel concerned with flight operations.
[2] Automatic terminal information service: the provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is prefixed with a unique letter identifier and is updated either routinely or when there is a significant change to weather and/or operations.
[3] Runway number: the number represents the magnetic heading of the runway.
[4] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered.
[5] Air Traffic Services Officer
[6] Closed taxiway markings: A yellow cross that is 9 m across, generally painted on the surface of the taxiway.
Occurrence summary
| Investigation number | AO-2024-061 |
|---|---|
| Occurrence date | 04/11/2024 |
| Location | Adelaide Airport |
| State | South Australia |
| Report release date | 24/06/2025 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | ANSP info/procedural error, Taxiing collision/near collision |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Pilatus Aircraft Ltd |
|---|---|
| Model | PC-12/47E |
| Registration | VH-FXJ |
| Serial number | 1541 |
| Aircraft operator | Royal Flying Doctor Service of Australia Central Operations |
| Sector | Turboprop |
| Operation type | Part 135 Air transport operations - smaller aeroplanes |
| Departure point | Adelaide Airport, South Australia |
| Destination | Pinnaroo Aircraft Landing Area, South Australia |
| Damage | Nil |