
Final report
Report release date: 19/05/2026
Investigation summary
What happened
On 5 January 2026, a Helicorp Leonardo Helicopters AW139 with 4 crew on board departed from its Canberra base in the Australian Capital Territory on a medical transport task to the Snowy Mountains, New South Wales. The task was the retrieval of a sick/injured hiker. While in the hover, after commencing to winch the paramedic down to the hiker’s location, the main rotors struck a tree, which had been previously identified by the crew as the nearest obstacle to the helicopter.
What the ATSB found
The crew positioned the helicopter with the nearest obstacle (a tree) in the pilot's blind spot prior to the pilot assuming sole responsibility for clearances to allow the air crew officer and paramedic to prepare for winching. Subsequently, the helicopter started to drift to the left prior to the air crew officer resuming responsibility for clearances.
The pilot did not detect and correct the helicopter’s drift towards its nearest obstacle while in the hover, which resulted in the main rotor striking the tree.
What has been done as a result
Following this occurrence, the operator:
- released an operations manual bulletin to provide additional guidance on helicopter clearance limits and included an increased minimum lateral clearance of 20 ft (6 m) for the main rotors under all conditions
- initiated a working group with the tasking agency to improve their operations
- undertook post-incident assurance activities with the flight crew prior to their return to operations
- conducted an updated refresher session on verbal escalation during sterile cockpit procedures
- included methods and terminology for escalation in its current human factors training program.
Safety message
Always consider and plan for escape path options in mountainous terrain wherever practicable. In preparation to conduct the winch, the crew positioned the helicopter facing downslope, in the opposite direction to the approach. This provided the pilot with an escape path option for the helicopter, which they used immediately after the main rotor strike occurred.
In addition, the use of minimum clearances in confined areas should be limited to those occasions when the nearest obstacle(s) can be actively monitored by appropriately trained crew. If this is not achievable, then use greater margins wherever practicable.
The investigation
| The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On 5 January 2026, at 1616 local time, a Helicorp (Toll Helicopters) Leonardo Helicopters AW139 with 4 crew members on board departed from its Canberra base in the Australian Capital Territory on a medical transport task to the Snowy Mountains, New South Wales. The task was a likely winch retrieval of a sick/injured hiker. The crew consisted of the pilot in the front right seat, air crew officer (ACO) in the front left seat, paramedic in the forward right cabin seat, facing rearwards, and doctor in the forward left cabin seat, facing rearwards.
En route to the reported location, the pilot assessed the helicopter’s performance and estimated that they would be 200 kg overweight for a winching operation. Consequently, the crew decided to conduct a search first, to confirm the hiker’s location and burn fuel, before conducting a power check and deciding if the doctor could remain on board for the winching. About 30 minutes after take-off, the paramedic detached from their harness and transitioned to a wander lead1 to prepare for the winching. The pilot also cleared the ACO to transition from the front left seat to the cabin and onto a wander lead.
On approach to the reported location, the low flying checks were completed, and the ACO opened the right cabin door for the search. The pilot then saw a flare appear below them on the right side of the helicopter and the ACO identified the hiker near a waterfall in a re-entrant,2 which was the reported location. They assessed that the helicopter would need to be flown slowly up the re-entrant towards the waterfall and then turned around prior to winching, to provide an escape route down the valley.
The crew conducted their winch checks and then the pilot conducted the power check and confirmed that the helicopter had sufficient power margin to keep the doctor on board for the winching. The helicopter then descended into the re-entrant and transited up the left side at slow speed (Figure 1). Before they reached the hiker’s location, the pilot momentarily stopped the transit as they experienced a ‘power-suck’3 and assessed that they had a tail wind. When the power stabilised, the pilot turned the helicopter around and reversed the helicopter into the re-entrant for the final 200 m to the hiker’s location.
Figure 1: Entry and exit tracks to the hiker’s location and rotor strike

Source: Toll Group and Google Earth, annotated by the ATSB
After turning the helicopter around, the left cabin door was opened to facilitate the ACO providing obstacle clearances to the pilot who reported that abort options were now down the valley. The crew took about 5 minutes to position the helicopter, assess the power and confirm that they were ready to winch. During this period, the ACO alternated between the open left and right cabin doors and announced clearances to the pilot, identifying the respective door from which they were provided.
The ACO briefed the pilot that the nearest obstacle was 20 ft away in the 8–9 o’clock position (left side) and directed the paramedic to the right cabin door to assess the ground below and plan the winching operation. The pilot subsequently asked if they could descend further and the ACO moved to the left door and instructed the pilot to descend 20 ft and move back 10 ft. This reduced the risk of a conical spin developing, due to the wind conditions in a narrow insertion point. After descending and backing further into the re-entrant, the pilot reported to the crew that they were starting to experience recirculation4, which was increasing the power requirements. Once all indications were normal and within limits, the pilot confirmed the winch operation could proceed. The paramedic and ACO then agreed on their winching location.
Prior to starting the winching, the left door was closed for cabin security. Before the ACO closed the left door, they briefed the pilot that the nearest obstacle was now a tree, 10 ft ‘above and to the left’ (this was 10 ft laterally in the 7–8 o’clock position and above the main rotor disk), and that there were also treetops about 35 ft below on the left. After the ACO closed the left cabin door, they pointed to the nearest obstacle through the window while instructing the doctor ‘that’s yours [name], keep an eye on that’, which the doctor acknowledged.
The ACO asked the pilot if they had a good hover reference, to which the pilot responded in the affirmative. The ACO then announced they were bringing the winch in to get the paramedic ready and that their ‘eyes are inside’, to which the pilot responded, ‘I’ve got the scan’. The ACO and paramedic conducted their pre-winch checks, and the paramedic was brought outside the right door on the winch, at which point the ACO confirmed with the pilot that they were clear to winch. However, before they started to winch, the ACO announced they needed to do the pre-winch brief and aircraft performance brief.
While the ACO was conducting the brief, the doctor was becoming concerned about the obstacle clearance on the left side but did not want to interrupt the ACO during safety‑critical checks. As soon as the ACO completed the briefs and started to winch the paramedic down, the doctor announced they had moved left ‘slightly’, and the ACO immediately cleared the pilot to move right ‘10’. This was followed by escalating calls from the ACO to the pilot to move right. As the pilot attempted to correct to the right, the main rotor struck the tree, and the calls from the ACO immediately changed to ‘move forward’. The pilot then transitioned the helicopter to forward flight while the ACO recovered the paramedic on the winch back into the cabin.
After the helicopter transitioned to forward flight, the pilot conducted a control check, and the ACO detected a clicking noise. The pilot announced that Perisher was the closest pad and requested confirmation of what struck the tree. The ACO and doctor confirmed it was the main rotor that struck the tree in the 7–8 o’clock position and not the tail rotor. The pilot made a PAN call to air traffic control, and the paramedic notified their base of the incident and that they would land at Perisher. The helicopter landed at Perisher at 1737 with minor damage. The hiker subsequently walked out and declined medical assistance.
Context
Personnel information
Pilot
The pilot spent 17 years in Army aviation as a line pilot and instructor. They held an Air Transport Pilot Licence (Helicopter), a class 1 medical certificate without restrictions, and had accumulated 6,880 hours flight experience, which included 2,065 hours on the AW139 with 84 hours in the previous 90 days. They joined the operator in 2016, completed the AW139 type rating in Italy, and started on the helicopter emergency medical service contract in 2017.
Air crew officer
The ACO spent 6 years in Army aviation before joining the operator about 4 years prior to the incident. They had accumulated about 1,700–1,800 hours flight experience, which included 800–900 hours on the AW139. The ACO’s 4 years with the operator included 1 year as a human factors instructor at their previous base.
Retrieval doctor
The doctor started with the emergency medical service 5 years prior to the incident as a registrar. They completed 1.5 weeks of aviation training with the operator, which included winch training and assessment. They conducted cyclic training 3 times per annum, which included human factors and safety management systems discussions with an incident case study. Crew resource management was incorporated in the human factors training.
The doctor reported that the incident flight was their first experience of being asked to monitor an obstacle in a confined area. They were not trained to provide clearances in their aviation training but were taught the safety call ‘climb, climb, climb’ if they had an immediate safety concern. Leading up to the main rotor strike they thought about the safety call but considered it was not appropriate with the obstacles above them and instead alerted the crew to the movement left.
Helicopter information
General information
The helicopter was a Leonardo Helicopters (formerly Agusta Westland) AW139, manufactured in Italy in 2015 and registered in Australia in December 2015. It was powered by 2 Pratt & Whitney Canada PT6C-67C gas turbine engines and fitted with 5 main rotor blades and 4 tail rotor blades.
To simplify the pilot’s instrument scan, a power index (PI) indicator is presented on the primary flight display for each engine. The PI combines the torque, temperature and gas generator speed instruments into a single indicator. While the PI is in the green range, no engine limits are exceeded. Above the green range, there is a yellow cautionary range, which indicates the take-off power range and above that, there are 2 red lines indicating maximum take-off PI and maximum transient PI.
Damage
The operator reported minor repairable damage to 3 main rotor blade tips (Figure 2). In addition, there was minor damage to the horizontal stabiliser and tail boom, which were struck by debris from the tree struck by the main rotor.
Figure 2: Main rotor blade damage (left) and horizontal stabiliser damage (right)
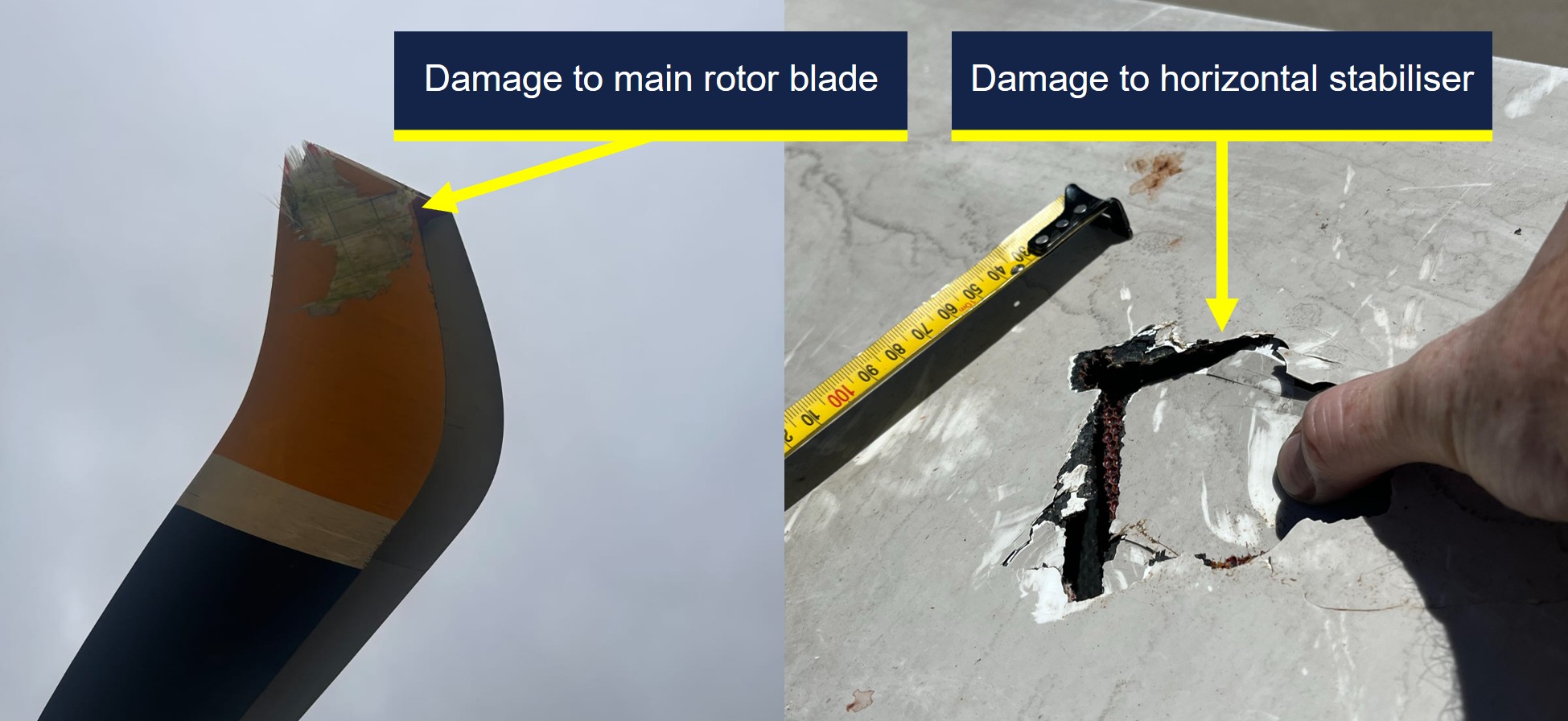
Source: Toll Group, annotated by the ATSB
Recorded data
The aircraft was fitted with a Curtis-Wright Multi-Purpose Flight Recorder (MPFR), which contained the cockpit voice recorder and flight data recorder. The MPFR was provided to the ATSB and was successfully downloaded at the ATSB’s Canberra facilities on 7 January 2026. After download, the MPFR data was uploaded to the Flight Animation Software (FAS) program where the flight data and cockpit voice data were synchronised for analysis.
The FAS program revealed that the PI was fluctuating between the green and yellow ranges while the helicopter was in the hover in preparation for winching. However, the vertical speed was steady with only isolated momentary fluctuations of 50 ft/min rate of climb recorded.
When the ACO cleared the pilot to move right, away from their nearest obstacle, the helicopter rolled level from its left wing low hover attitude, the PI for both engines exceeded the maximum take-off PI red line momentarily and the vertical speed recorded a 100 ft/min rate of climb, followed by the main rotor strike.
The helicopter was also fitted with video-audio recording equipment in several locations, which included the cabin. A copy of the recordings for the accident flight were provided to the ATSB for review and analysis of the sequence of events in the cabin.
Operational information
Operations Manual Volume 2 – Rotary Wing
Volume 2 of the operator’s operations manual provided the rotor clearance requirement of 20 ft (6 m) horizontally from all obstacles. However, the manual also stated that by day only, and once established in the hover, the clearance could be reduced to 10 ft if it allowed for a more suitable winching position.
Operations Manual Volume 6 – Winching Operations
Volume 6 of the operations manual provided the following information for winching operations:
• Once established in the hover the PF [pilot flying] will normally be able to maintain position within the target area. However, there is often a requirement for minor repositioning whilst winching. During this precision manoeuvring the PF is relying on instruction from the ACO to accurately position the aircraft whilst remaining clear of any obstructions.
• A check of the left side of the aircraft must be conducted to identify the closest obstacle and ensure clearances are adequate. If the left door is opened to achieve this clearance, it must be closed prior to committing to the winch. At any time the ACO has their scan / eyes inside or checking the left, they are to advise this and receive acknowledgment from the PF.
• Once the ACO is back on the right side of the aircraft cabin, they are to ask the PF 'HOW IS YOUR HOVER REFERENCE?' If suitable references are available, the PF will respond with ‘HOVER REFERENCES ARE GOOD’ or request manoeuvring to improve references.
• WARNING: If suitable error tolerant hover references cannot be achieved by the PF, winching is not to be commenced.
The winching emergencies section of the manual included the emergency keywords ‘climb, climb, climb’ with the following caveat:
If not appropriate due to obstacles or terrain to call “CLIMB, CLIMB, CLIMB” a call for immediate aircraft movement is to be used in the required direction. For example: “LEFT, LEFT, LEFT”, “RIGHT, RIGHT, RIGHT” OR “MOVE FORWARD NOW.”
Safety analysis
The winch location was in a re-entrant near a waterfall, which required the pilot to turn and reverse the helicopter in for an assessment, before descending to a lower hover height for the planned winching operation. This provided the pilot with an escape route downslope and reduced the risk of a conical spin developing from a high winch but resulted in the nearest obstacle in the 7–8 o'clock position being in the pilot’s blind spot.
This obstacle was a tree with the nearest branch located above the main rotor disk and laterally clear of it by about 10 ft, which complied with the operator’s minimum clearance requirements. However, the proximity and height of the surrounding trees resulted in recirculation disturbing the helicopter from a stable hover position, which increased the control inputs required by the pilot compared with their initial higher hover height.
The ACO provided the pilot with obstacle clearances behind the helicopter until it was time to conduct their pre-winch checks with the paramedic, at which point nobody qualified was available to provide clearances to the rear of the helicopter. While the ACO and paramedic prepared for the winching, the doctor was monitoring their nearest obstacle to the rear left. When the ACO moved onto the pre-winch and aircraft performance briefs, the pilot was aware the ACO had returned to the right door, and the doctor started to sense the helicopter was drifting left towards their nearest obstacle. However, the ACO had not resumed providing clearances and the doctor’s training had reinforced the importance of not interrupting safety‑critical checks.
Due to the risk of a person descending on the winch snagging on the airframe, the ACO would not resume their scan to provide clearances until after the paramedic had descended below the airframe. However, when the ACO started their pre-winch brief at the right door, it was possible that either the pilot anticipated the ACO resuming their scanning role and relaxed their own scan, or that their attention was diverted from their external scan by the briefs, such that they did not detect and correct the helicopter’s drift.
The doctor alerted the crew to the fact that they appeared to be drifting to the left as soon as the ACO started to winch the paramedic down, which triggered a ‘move right’ call from the ACO to the pilot. In response, the pilot applied a small roll input to the right combined with a small increase in collective and the main rotors struck the nearby tree.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the main rotor strike involving Leonardo Helicopters AW139, VH-TJF, 42 km south-east of Corryong Airport, New South Wales, on 5 January 2026.
Contributing factors
- The crew positioned the helicopter with the nearest obstacle (a tree) in the pilot's blind spot prior to the pilot assuming sole responsibility for clearances to allow the air crew officer (ACO) and paramedic to prepare for winching. Subsequently, the helicopter started to drift prior to the ACO resuming responsibility for clearances.
- The pilot did not detect and correct the helicopter’s drift towards its nearest obstacle while in the hover, which resulted in the main rotor striking a nearby tree.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Safety action by Helicorp
The operator released an Operations Manual Bulletin in response to the incident, which addressed the following points:
- increased their rotor clearance limit to 20 ft (6 m) in all circumstances
- provided additional guidance on determining spacing from overhanging obstacles
- provided additional guidance on the requirements for error tolerant references
- emphasised the need to prioritise error tolerant hover reference(s) selection over escape and downwash considerations.
A working group was initiated between the operator and tasking agency to improve interagency operations. Additionally, post-incident assurance activities were undertaken with the flight crew prior to their return to operations and an updated refresher session on verbal escalation during sterile cockpit procedures was conducted. Methods and terminology for escalation have also been included in their current human factors training program.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
- ACT Ambulance Service
- cabin video footage and audio of the incident flight
- operator, its head of aviation safety and quality, and its investigator
- pilot, air crew officer and retrieval doctor of the incident flight
- recorded data from the MPFR unit on the aircraft.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Agenzia Nazionale Per La Sicurezza Del Volo (ANSV, Italy)
- air crew officer
- Civil Aviation Safety Authority
- Leonardo Helicopters
- operator
- pilot
- retrieval doctor.
Submissions were received from:
- air crew officer
- Civil Aviation Safety Authority
- operator
- pilot.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
| 1 | ^ A wander lead is a flexible safety tether used by crew members to maintain a secure connection to the aircraft while allowing them to move freely around the cabin. |
| 2 | ^ A re-entrant appears on the map as a U or V shape in the contour lines, pointing back into a hillside rather than sticking out of the hill (as would a spur). |
| 3 | ^ A sudden increase in the power required to maintain the desired flight path. |
| 4 | ^ Recirculation is a condition in which a helicopter’s rotor system ingests its own downwash, reducing rotor efficiency and degrading lift and control response. |
Occurrence summary
| Investigation number | AO-2026-002 |
|---|---|
| Occurrence date | 05/01/2026 |
| Occurrence time and timezone | 17:25 Eastern Daylight-saving Time |
| Location | 42 km south-east of Corryong Airport |
| State | New South Wales |
| Report release date | 19/05/2026 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Dissemination |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Controlled flight into terrain (CFIT), Forced/precautionary landing |
| Occurrence class | Serious Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Leonardo Helicopters |
|---|---|
| Model | AW139 |
| Registration | VH-TJF |
| Serial number | 31710 |
| Aircraft operator | Helicorp Pty Ltd |
| Sector | Helicopter |
| Operation type | Part 133 Air transport operations - rotorcraft |
| Activity | Commercial air transport-Non-scheduled-Medical transport |
| Departure point | Southcare Base Helicopter Landing Site, Australian Capital Territory |
| Injuries | None |
| Damage | Minor |