
Final report
Report release date: 05/12/2025
Investigation summary
What happened
At 1807 local time on the evening of 1 July 2025, a Royal Flying Doctor Service Beechcraft King Air B200, registered VH-RFD, with 2 pilots and a paramedic on board, taxied at Hobart Airport, Tasmania, for a night flight to Launceston. As the aircraft taxied to conduct a 180° turn using the runway 30 turnaround pad, it struck a taxi light with the right propeller. The aircraft incurred damage to the propeller and a turnaround pad edge taxi light was also damaged.
After recognising the strike had occurred, the pilots reported it to air traffic control, returned to the parking apron and grounded the aircraft.
What the ATSB found
The ATSB found that the pilot flying subconsciously mistook the blue taxiway edge lights and double yellow line on the edge of the turning pad as taxi centreline guidance. This resulted in the pilot deviating from the marked taxiway centreline towards the runway edge light, resulting in the propeller strike.
The ATSB also found that the supervising pilot’s intervention did not occur in time to prompt the pilot flying to adjust the taxi route before impacting the edge light.
Safety message
All pilots are susceptible to human error. This incident highlights that pilots need to be vigilant and maintain an awareness of their location.
The airport environment contains numerous visual aids, markings, signals and signs. Pilots must remain situationally aware of their location, traffic and intended ground tracks to avoid obstacles. When the taxiway is suitable for the aircraft type, it is usually safest to follow the yellow line when taxiing at night, in reduced visibility or at an unfamiliar aerodrome.
Additionally, effective monitoring in a multi-crew environment is also paramount to aircraft safety. Bringing deviations to the early attention of the pilot flying promptly ensures the aircraft remains on a desirable track.
The investigation
| The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
At 1807 local time on 1 July 2025, a Beechcraft King Air B200, registered VH-RFD, operated by the Royal Flying Doctor Service (RFDS) with 2 pilots and a paramedic on board, commenced taxiing at Hobart Airport, Tasmania. The intended destination for this flight was Launceston Airport. It was dark, with little to no moonlight, and good visibility.
The pilot flying (PF) was operating under the guidance of a supervisory pilot (SP), prior to their final line check,[1] which was scheduled in 2 shifts time. The PF occupied the left‑hand side control seat in the cockpit. The SP, who was also designated pilot in command (PIC),[2] occupied the right-hand control seat.
At 1810, the aircraft entered runway 30 to backtrack[3] so that the full runway length could be used for take-off (Figure 1).
Figure 1: Taxi route
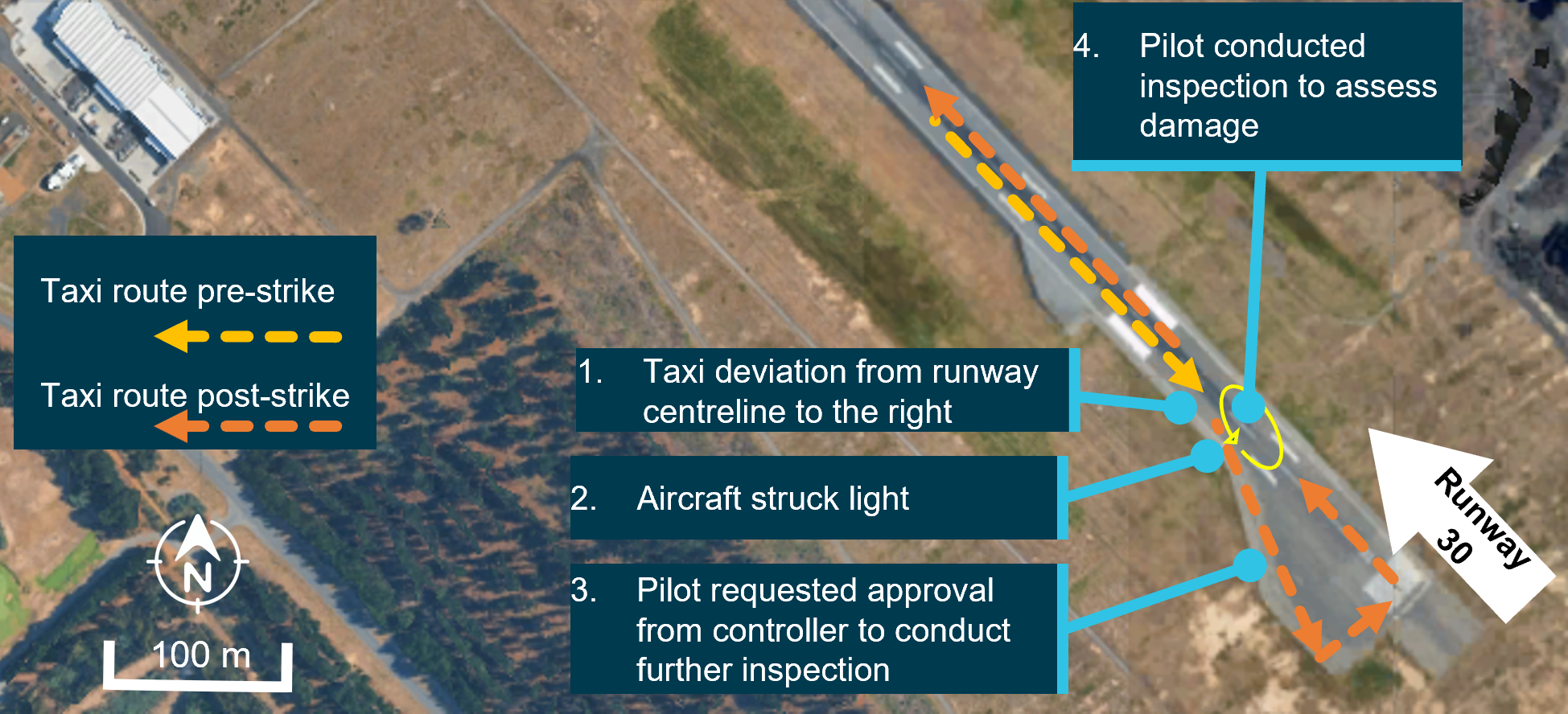
Source: Google Earth, annotated by the ATSB
The pilots reported that a common technique for taxiing and turning the King Air B200 is to make a wide arc turn to reduce stress on undercarriage components.
During taxi, the PF steered the aircraft away from the centreline taxiway ground markings, toward the right runway edge, approximately 100 m prior to the runway threshold (Figure 1, label 1). This manoeuvre was to position the aircraft for a 180° turn via the runway turnaround pad (a wide, paved area that allows room for aircraft to reverse taxi direction).
The pilot reported that they subconsciously mistook the blue taxiway edge lights and double yellow line on the edge of the turning pad as taxi centreline guidance. This subsequently resulted in positioning the aircraft to the far right of the turning pad, aligning the aircraft with the double yellow line runway edge light rather than the single yellow line. A reconstructed visual perspective, replicating what the pilot may have seen is shown in Figure 2.
Figure 2: Reconstructed pilot view, approaching and entering the turnaround pad
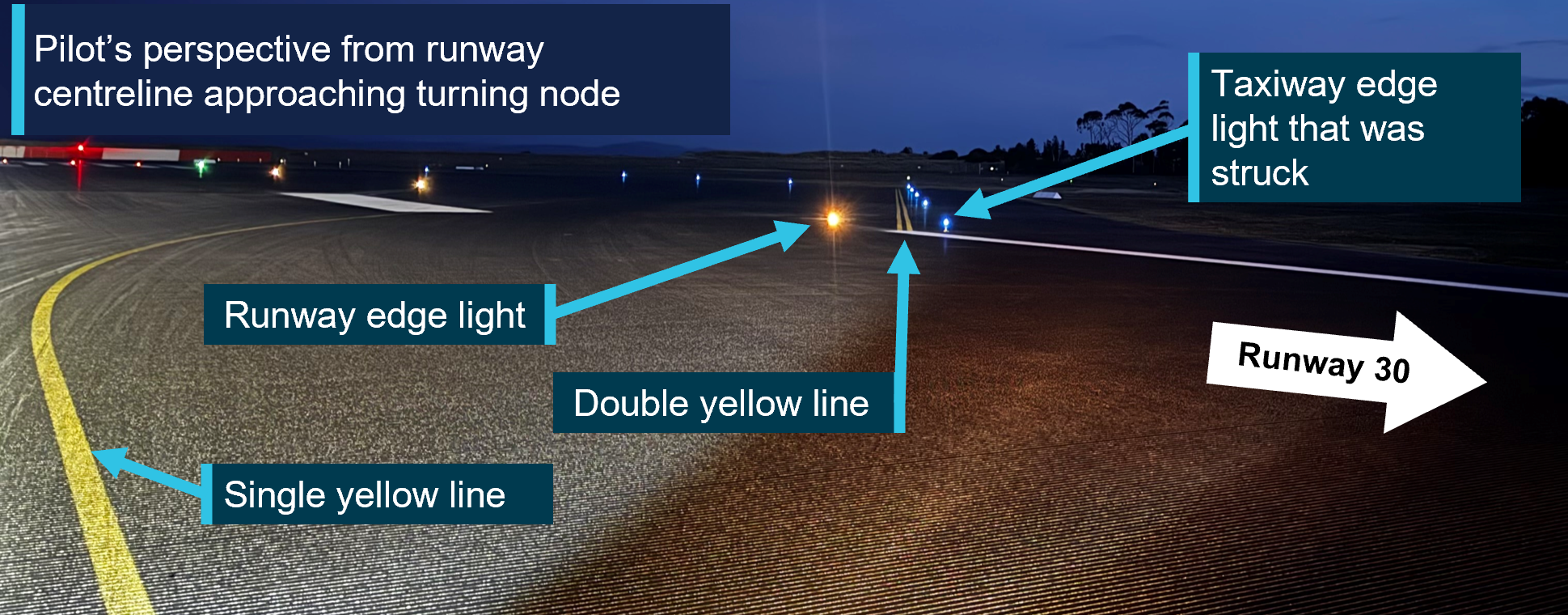
These images were taken post-occurrence. The height of the camera was lower than the pilot’s sightline during the incident. Source: Hobart Airport, annotated by the ATSB
The wide turn taken by the PF was consistent with what was expected by the SP. As the aircraft approached the right side of the turnaround pad, the SP recalled that they were waiting for the PF to turn the aircraft as it came into the proximity of a taxiway edge light. Once the SP identified that the aircraft was close to the edge light, the SP advised the PF. However, before the PF could steer away from the light, the right propeller struck it (Figure 1, label 2).
Suspecting the aircraft had struck the light, the PF requested from air traffic control (ATC) clearance to conduct a further ground inspection to assess for damage (Figure 1, label 3 and label 4).
The pilot then confirmed with ATC that the aircraft had struck the light (Figure 3) and advised that they would need to return to the apron.
Figure 3: Blue pad edge light damage
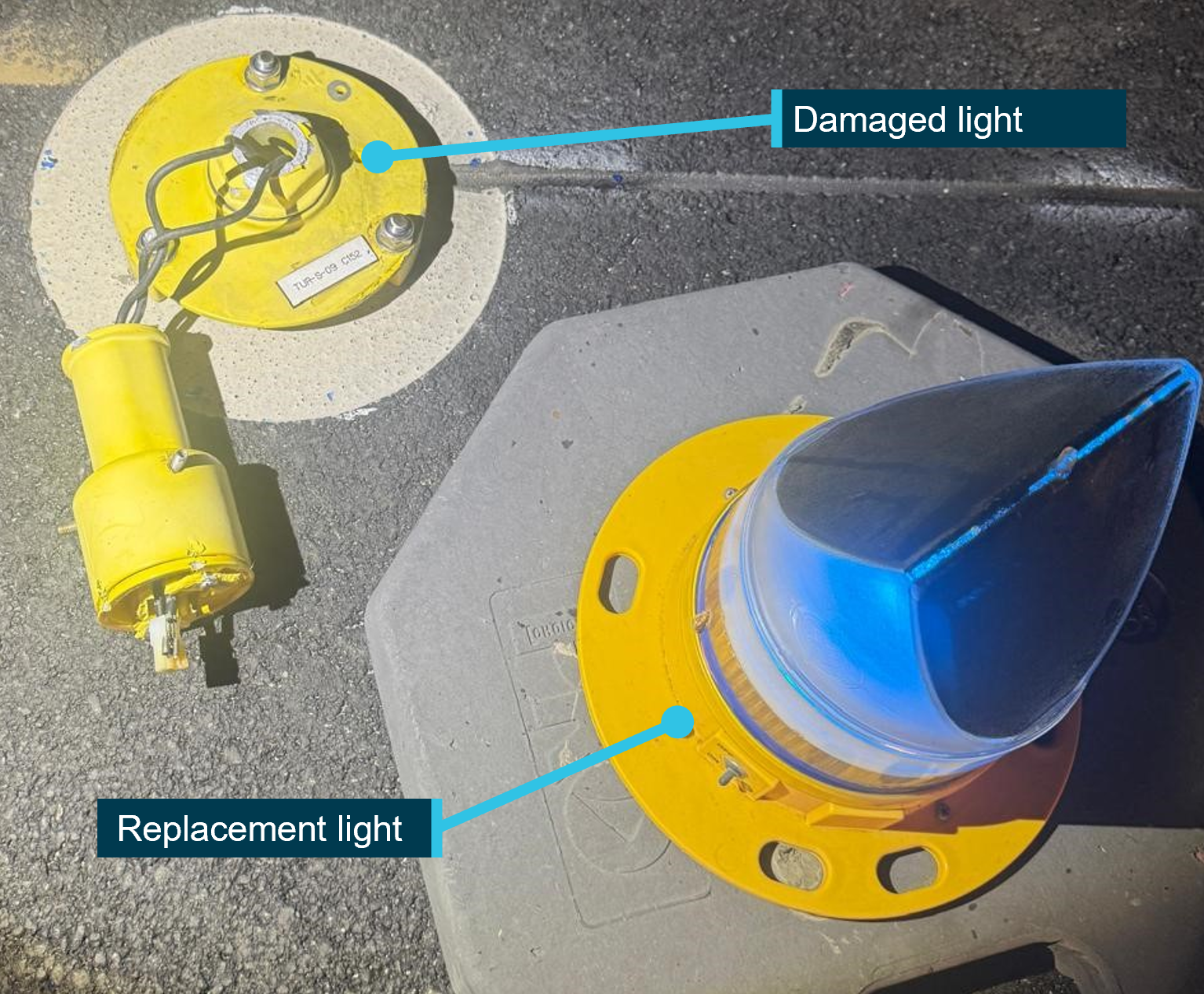
Source: Hobart Airport, annotated by the ATSB
After shutting down the aircraft, the pilots inspected the aircraft and identified damage to the right-hand side propeller (Figure 4).
Figure 4: Propeller damage
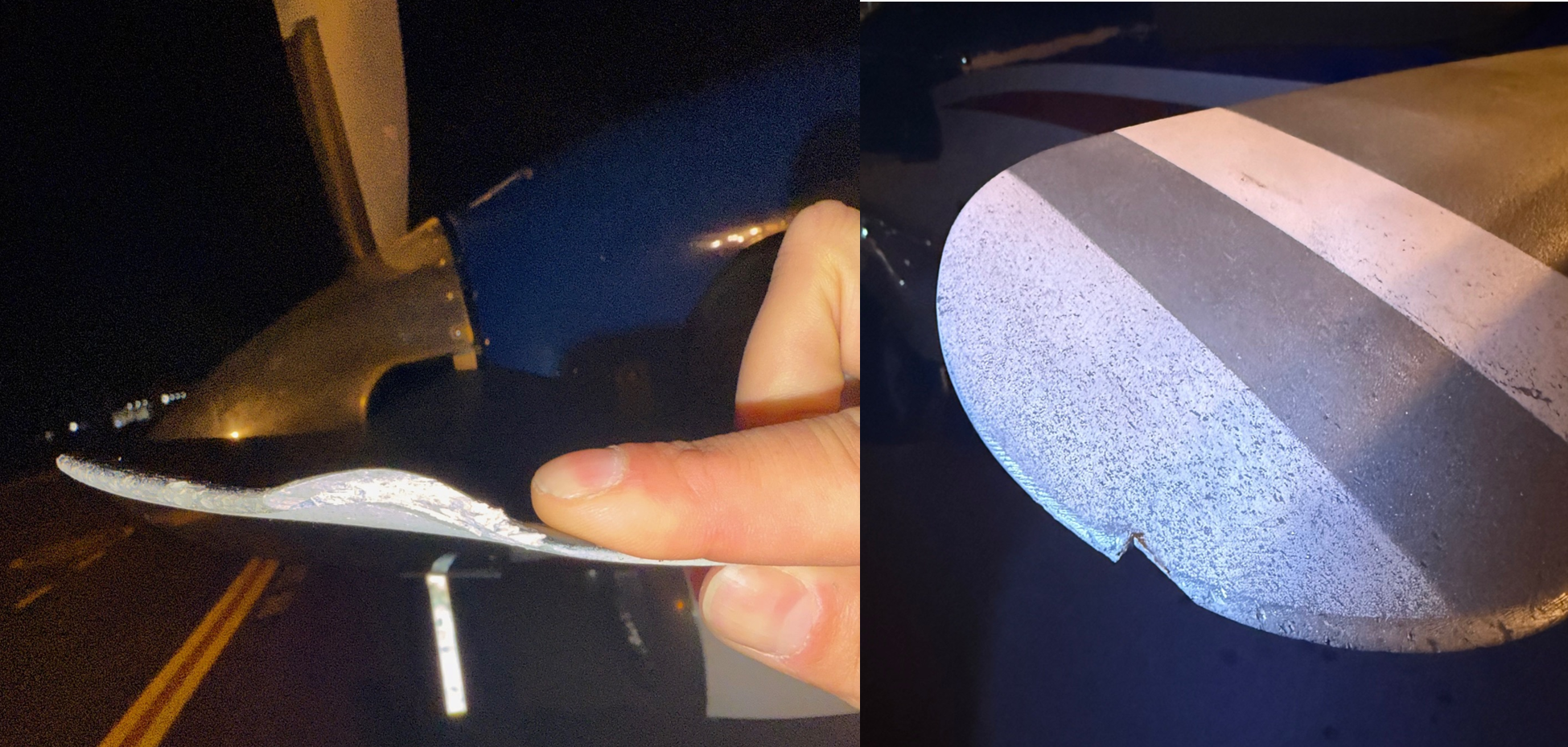
Source: RFDS
Context
Pilot information
Pilot flying
The PF held a commercial pilot (aeroplane) license and a valid class 1 aviation medical certificate. They reported a total flying time of about 4,920 hours with about 76 of those being on the King Air B200, having joined the RFDS in April 2025. They reported completing 5 previous flights to Hobart prior to the occurrence, as part of their line training under supervision. All except one of those flights involved the runway 30 threshold being displaced, and they did not utilise the turnaround pad.
Prior to joining the RFDS, the pilot had held training and examining approvals as well as key management positions at another operator.
Prior to the incident, the SP had assessed the PF as capable and their flying standard was reflective of that of a candidate approaching their final check.
Supervisory pilot
The SP held an air transport pilot (aeroplane) license and a valid class 1 medical. They reported a total flying time of 11,848 hours with 4,876 of these hours being on the King Air B200. They also held a management pilot role.[4]
Aircraft information
The Beechcraft King Air B200 is a pressurised, low-wing, twin turbine-engine aircraft with retractable landing gear. The aircraft had a certified maximum take-off weight of 5,667 kg and could be flown by a single pilot. The aircraft, serial number BL-171, was manufactured in the United States in 2014 and subsequently registered in Australia on 14 August 2014. The Royal Flying Doctor Service of Australia (South Eastern Section) had been the registered operator of the aircraft since August 2014.
Airport information
Hobart Airport is a certified airport consisting of one runway. Runway 12/30 was aligned north-west to south-east and was 2,727 m long and 45 m wide. The aircraft movement areas could accommodate aircraft with a wingspan of up to 36 m (such as a Boeing 737).
There were line markings and lights on the runway and turnaround pad to guide pilots in turning and lining up their aircraft for departure (Figure 5). The markings and design appeared to be consistent with the requirements of the Civil Aviation Safety Authority Part 139 Manual of Standards.
Figure 5: Illustrations (top) and photograph (bottom) of lights and line guidance at the turnaround pad
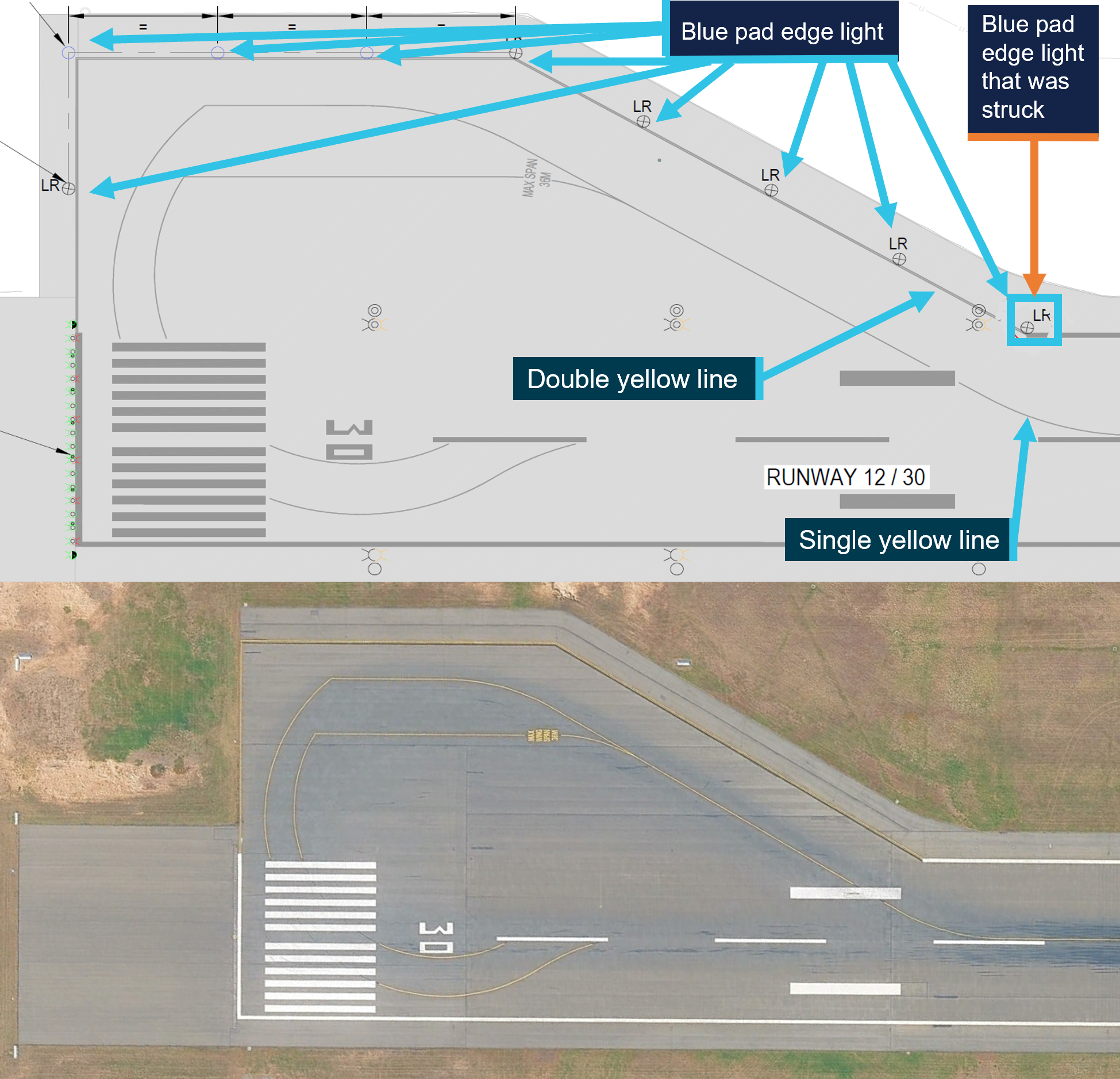
Source: Hobart Airport and Google Earth, annotated by the ATSB
RFDS operational induction
When a new pilot joins the RFDS, the operator carries out a structured induction and training program. Initially, a new pilot undertakes type/class training on the King Air B200 which includes an instrument proficiency check (IPC[5]). Following this training, the new pilot conducts line training flights in the presence of an RFDS supervisory pilot.
The objective of supervised line operations (line training) is to prepare the new pilot for single pilot, unsupervised line operations. The required training outcomes for the new pilot are:
- obtaining the required operational experience
- exposure to and gaining experience of the RFDS’s line operations
- gaining knowledge of the routes and aerodromes used by the AOC.
Whenever an SP occupies one of the pilot seats, they will be the PIC. These policies and procedures are outlined within the RFDS training and checking systems manual.
Training and supervising methodology
Many training methodologies apply the principle of allowing the student to recognise an error and self-correct. This established technique allows the student a chance, and time, to correct themselves, prior to intervention by the instructor or supervisor.
The US Federal Aviation Administration (FAA) Aviation Instructor’s Handbook (2020), which is a recommended reference document for the Civil Aviation Safety Authority’s pilot instructor rating exam, also references this instructional technique. It notes:
Correction of learner errors does not include the practice of taking over from learners immediately when a mistake is made. Safety permitting, it is frequently better to let learners progress part of the way into the mistake and find a way out.
The SP commented that retrospectively, they could have been more assertive and prompter in their intervention once they recognised the proximity of the aircraft to the light.
Safety analysis
Misinterpretation of taxiway/runway visual guidance
While backtracking, the pilot flying (PF) deviated to the right of track in preparation to conduct a wide left turn using the turnaround pad. Making a wide arc turn was a common technique used by pilots for taxiing and turning the King Air B200. As they turned into the turnaround pad, the PF mistakenly manoeuvred the aircraft to align with the blue taxiway edge lights and 2 yellow (edge line) markings. A pilot would normally rely on taxiing guidance of a single yellow line (and green lights), on a taxiway.
The PF was experienced, having held numerous approvals (training and management). However, in this instance, they reported that they subconsciously mistook the taxiway edge lights and double yellow line on the edge of the turning pad as taxi guidance. Observational audit methodologies, such as the Line Operations Safety Audit (LOSA) have demonstrated that crews make on average between one and five errors per flight sector (Thomas & Petrilli, 2004).
Supervisor pilot delayed intervention
The SP monitored the PF’s taxiing path as the aircraft deviated toward the right edge of the runway. This path was initially as expected by the SP reflecting normal operations for turning around using the turnaround pad.
The SP instructed the PF to correct their track when in proximity to the pad edge light, however due to the limited time available and proximity, a strike between the right propeller and taxi light still occurred.
The SP held the belief that the PF was capable, and this assessment may have contributed to delayed intervention, affecting their level of attention when monitoring the taxi path.
The SP adhered to the recognised training techniques in the FAA Aviation Instructor’s Handbook, by allowing the PF a degree of latitude prior to their intervention. However, this action resulted in the SP delaying the intervention and advising the PF of the proximity of the pad edge light, leaving insufficient time to avoid the light.
The SP recognised, retrospectively, that if they had recognised the proximity of the aircraft to the light earlier, they would have been more assertive and more prompt in their intervention.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the propeller strike of a taxiway edge light involving Beechcraft King Air B200C, VH-RFD, at Hobart Airport, Tasmania, on 1 July 2025.
Contributing factors
- The pilot flying misinterpreted the markings and lights at the turnaround pad. This resulted in the pilot taxiing too close to the taxiway edge light, resulting in a propeller striking the light.
- The supervising pilot did not allow enough time to prompt the pilot flying to adjust the taxi route, for the intervention to be effective.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- pilot flying and pilot supervising
- Royal Flying Doctor Service, South Eastern Section
- Hobart Airport
- Civil Aviation Safety Authority
- Airservices Australia
- Bureau of Meteorology
- Flightradar24.
References
Federal Aviation Administration. (2020). Aviation Instructors Handbook. U.S. Department of Transport.
Thomas , M. J., & Petrilli, R. M. (2004). Error Management Training: An investigation of expert pilots’ error management strategies. Adelaide: Centre for Applied Behavioural Science.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- pilot flying
- pilot supervising
- Royal Flying Doctor Service, South Eastern Section
- Hobart Airport
- Airservices Australia
- Civil Aviation Safety Authority.
A submission was received from Hobart Airport.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] A line check is the final pilot’s assessment after line training. After a successful final line check, the pilot is released to a normal line flying operation. See also RFDS operational induction.
[2] The pilot in command (PIC) of an aircraft is the person aboard an aircraft who is ultimately responsible for its operation and safety during flight.
[3] Backtrack. To taxi on a runway-in-use, in the opposite direction to the aircraft’s take-off or landing direction.
[4] Management Pilot means a pilot assigned to management duties
[5] An instrument proficiency check assesses flying skills and operational knowledge, ensuring the capability to exercise the privileges to conduct a flight under the IFR.
Occurrence summary
| Investigation number | AO-2025-034 |
|---|---|
| Occurrence date | 01/07/2025 |
| Location | Hobart Airport |
| State | Tasmania |
| Report release date | 05/12/2025 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Ground strike |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Beechcraft |
|---|---|
| Model | B200C |
| Registration | VH-RFD |
| Serial number | BL-171 |
| Aircraft operator | Royal Flying Doctor Service (South Eastern Section) |
| Sector | Turboprop |
| Operation type | Part 135 Air transport operations - smaller aeroplanes |
| Departure point | Hobart Airport, Tasmania |
| Destination | Launceston Airport, Tasmania |
| Damage | Minor |