
Final report
Report release date: 27/11/2025
Investigation summary
What happened
At about 0600 on 6 March 2025, the second engineer of Spirit of Tasmania I began a routine oil change on one of the ship’s main engine turbochargers. Problems were encountered during the oil change, and it was decided to replace the turbocharger’s bearing housing cover plate. This significant change to the scope of work required access to the top of the engine.
The second engineer and another engineer on duty then carried out the work, which took longer than expected and required both to climb on and off the engine top several times. At 0815, while climbing off the engine, the second engineer slipped and fell heavily, resulting in serious injury.
What the ATSB found
The ATSB investigation found that, while access to the top of the engine was regularly required, there was no access ladder or platform nor was a standard safe route defined or used. Consequently, the injured second engineer used an unsafe access route along the engine rocker covers at the time of the accident.
The investigation also identified that although the shipboard safety management system required that the change of work scope necessitated a review of the Job Safety Analysis (JSA) and/or completing a new prestart safety checklist (Take 5), neither was undertaken due to perceived time pressure and a perception that the work was low risk, resulting in the risk of a fall not being properly considered.
In addition, the ATSB found that the JSA procedure was not effectively implemented on board. This resulted in there being no JSA in place for the work being done at the time of the incident. Further, the JSAs covering other work on top of the engine did not address the risks involved in accessing the engine top.
What has been done as a result
The ship’s managers, TT-Line Company (TT-Line), reacted proactively to the accident and put in place several engineering and procedural measures to reduce the risk of falls from the engine top and general access risks.
TT‑line has provided a removable work platform for safe access to the top of the engines for both sister ships, Spirit of Tasmania I and II. The JSAs related to work on turbochargers and the exhaust manifold have been updated to include the access risk. The updated JSA also includes a restriction on routine maintenance of critical equipment during short duration port calls, reducing time pressure constraints in case of unforeseen problems.
Additionally, modifications have been made to the bearing housing cover plates, reducing the need for personnel to access the engine top for ad hoc repairs.
Safety message
The ATSB has investigated numerous occurrences involving unsafe working practices on board ships. Many of these resulted in serious or fatal injury(s) due to falls from height, machinery or equipment falling, explosions and other hazardous occurrences. A recurring factor in such incidents is the people involved in the work not recognising the hazards involved and/or they considered the work routine and low risk. In addition, risk assessment and mitigation are often not done or ineffective.
This investigation highlights the importance of effective risk controls, which requires staff at all levels on board and ashore to contribute towards the effective implementation of the shipboard safety management system.
The occurrence
At 0600 local time on 6 March 2025, the passenger ship Spirit of Tasmania I berthed in Geelong, Victoria, following a routine overnight voyage from Devonport, Tasmania. The ship was expected to sail at about 0830 on its normal schedule for a double sailing.[1]
After shutting down the main engines at about 0630, the second engineer (the senior engineer on watch), decided to complete a scheduled oil change on one of number 1 main engine’s turbochargers. This regular scheduled maintenance job was performed frequently and usually took one hour, which left sufficient time to prepare the engines for departure.
The job required removing the drain and air plugs from the turbocharger’s bearing housing cover plate to drain the oil (Figure 1), then refitting them and refilling the housing with about 1.5 litres of oil. As there had been issues in the past with the steel plug damaging the thread in the aluminium cover plate, the drain plug was fitted into a steel threaded insert installed in the cover plate, rather than directly screwed into the cover plate. However, when the second engineer removed the drain plug, the insert rotated and started unscrewing from the cover plate. In response, they fixed the insert back into the aluminium cover plate using a specialised adhesive, reasoning that this would hold until the next port call when more time would be available to allow for a permanent repair.
Figure 1: Turbocharger cover plate
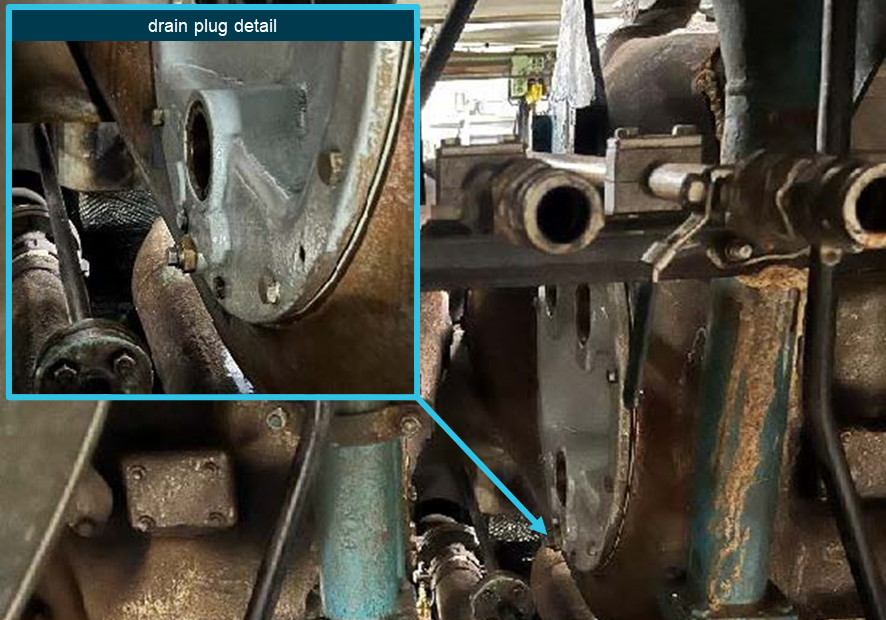
Source: TT-Line, annotated by the ATSB
At around 0700 the first engineer arrived in the engine room and was advised that the insert had been secured with the adhesive applied. Concerned that the drain plug might come undone during operation, the first engineer asked the second engineer to replace the bearing housing cover with a spare. The drain plug problem was known and several spare plates were available to resolve the problem. With the upcoming departure in mind, the second engineer immediately went about this task with the third engineer (the junior engineer on watch) assisting.
While the oil change could be done by a person standing on the deck aft of the engine between the turbocharger bearing assemblies, replacing the housing cover required access from above the engine near the exhaust gas manifold. This location could be accessed by climbing over the rocker covers on the ‘B’ cylinder bank (Figure 2). The cover closest to the turbocharger (B1) had 2 strips of anti-slip material attached to the blue gloss paint (there were no steps or other permanent means of access).
Figure 2: Access to top of engine (looking aft)
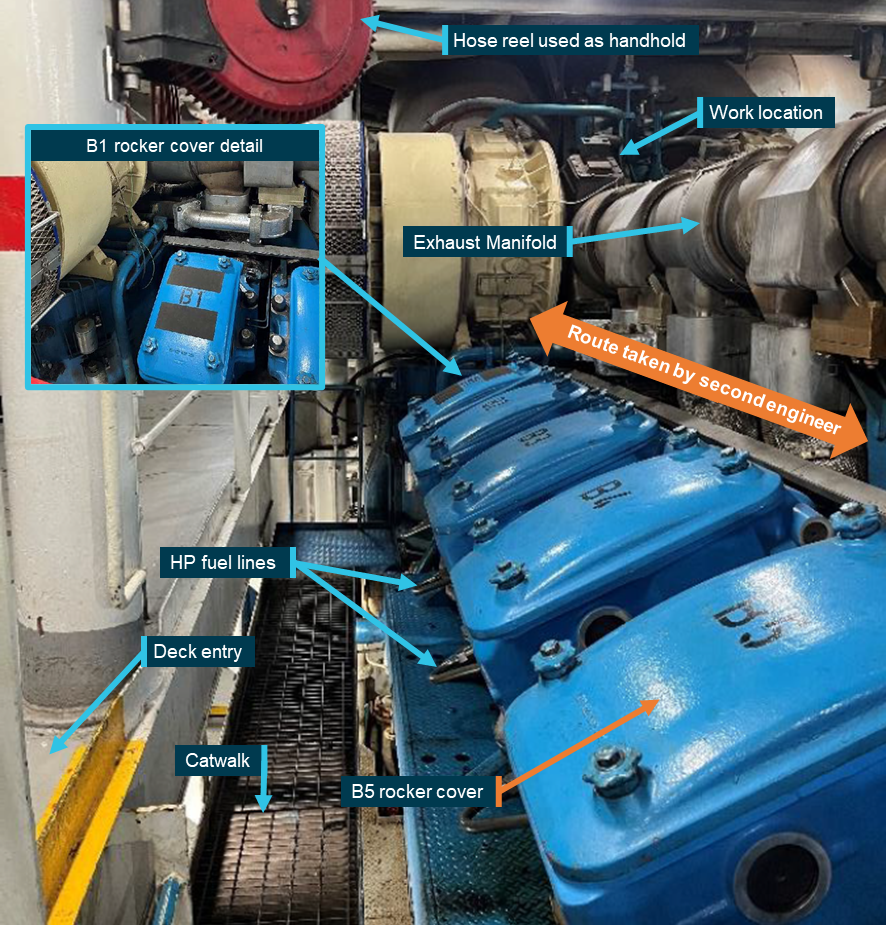
Source: TT-Line, annotated by the ATSB
The second engineer had accessed the same location on top of the engine many times in the past 12 years working on board the ship. The engineer considered the best way to access this location was to step straight from the deck across the lower catwalk onto the B5 rocker cover and then walk along the exhaust manifold (Figure 2). This route avoided the high-pressure fuel pipes at the bottom of the cylinder heads.
The second and third engineers started replacing the cover, with both climbing up and down from the engine by stepping from the deck directly onto the rocker covers and back. After replacing the bearing cover, they found that it was leaking and decided to fit another spare cover. At 0800 their watch ended and the third engineer left the engine room, but the second engineer felt responsible for completing the work and decided to continue working, so that the engine would be available for the scheduled departure at 0830.
At 0816, while working to replace the bearing cover, the second engineer walked aft over the rocker covers, using the exhaust manifold for support (Figure 2). At the B5 rocker cover, the engineer let go of the exhaust manifold and reached across the gap to a swivelling air hose-reel for support but slipped off the rocker cover and struck its corner before falling heavily onto the catwalk grating.
After falling, the second engineer took a short while to check for injuries before standing up. Deciding no major injury had resulted, the engineer completed the remaining work, which involved climbing up and down via the B5 rocker cover to secure components on top of the turbocharger. The engineer then went to the engine control room (ECR) and removed the engine isolation to allow it to be started for departure.
While in the ECR, the second engineer reported their fall to the first engineer who called the ship’s medic to assess the second engineer. The medic’s assessment resulted in a referral to a doctor ashore.
On the following day, 7 March, a doctor diagnosed the second engineer as having suffered a serious knee injury, which required surgery and an extended recovery period of many weeks.
Context
Spirit of Tasmania I
Spirit of Tasmania I (IMO No 9158446) is a passenger/Ro-Ro[2] ship which was built in 1998. It is one of 2 sister ships operated by TT-Line Company (TT-Line), Australia, that provide a daily passenger/vehicle service between Devonport, Tasmania, and Geelong, Victoria.
The ship has an overall length of 194.33 m and a beam of 25.0 m. It can carry a maximum of 1,400 passengers in a variety of cabin and seated accommodation and has 2,565 lane metres of vehicle space.
Depending on demand (passengers, vehicles and cargo), Spirit of Tasmania I and its sister ship operate a single or double sailing schedule. On the single sailing schedule, the ships depart Geelong or Devonport in the evening to complete the voyage the next morning. On double sailings, there is a night‑time as well as a daytime sailing for a 9‑hour voyage, with the ship operating at a higher speed using all 4 of its main engines.
Propulsion
Spirit of Tasmania I’s main propulsion consists of twin controllable pitch propellers (CPP) driven through 2 gearboxes by 4 Wartsila 16ZA40S V-type diesel engines with a total power output of 42,240 kW.
Depending on requirements, the ship can be safely operated with 2, 3 or 4 engines online. This configuration allows the ship to be operated efficiently at both high and low speeds, and engines can be started and clutched into the gearbox with the ship underway.
Engine room crew
At the time of the incident, Spirit of Tasmania I’s engine room crew comprised a chief engineer, first engineer, 2 second engineers, 4 third engineers, 2 electrical engineers and 3 integrated ratings (IR).
The first engineer had worked on board Spirit of Tasmania I and 2 for a total of about 22 years, initially as third engineer for a couple of years and then as a second or first engineer.
The injured second engineer joined the ship 3 days before the incident but had worked on board for the past 12 years, usually as a second engineer and sometimes as the first or third engineer. The second engineer’s work and rest hours leading up to the incident complied with prescribed requirements for seafarers and reported having adjusted to their watchkeeping schedule. The second engineer reported feeling under pressure to replace the cover plate before the ship’s departure to ensure the engine was available as the main engines were their specific area of responsibility.
Watchkeeping
Engine room watches were kept by the second and third engineers and the IRs across a standard watchkeeping schedule of 4 hours on followed by 8 hours off. Each watch comprised a senior and a junior engineer and one IR.
The chief, first and electrical engineers were not assigned to a watch and worked standard daywork hours and other work when required by the ship’s operations. The first engineer’s work mainly involved planning and supervising engine room maintenance.
Maintenance planning
Planned maintenance was based on defined calendar time or running hour intervals with the ships planned maintenance system (PMS) generating a list of scheduled jobs for the week ahead. This list was posted in the engine control room (ECR) for the planning of maintenance work around the ship’s operations.
In addition to watchkeeping duties, each engineer carried out scheduled routine maintenance as per the PMS on their assigned machinery item(s). The second engineer was responsible for the main engines and, with extensive experience in a senior position on board, had significant autonomy to plan and carry out routine work without the first or chief engineer’s direct involvement or supervision.
Incident location
The second engineer fell while working on a main engine and there were many routine maintenance and repair jobs that required crew to access the top of the main engine(s). There were no permanent ladders or access platforms for access. Instead, the crew accessed the engine top by stepping on the rocker covers (Figure 2).
Due to their V-type design, the rocker covers were angled at about 25° from the vertical. Anti-slip tape had been applied to the painted surface of the B1 rocker cover for safer access to the turbochargers (Figure 3).[3]
Figure 3: B1 cylinder rocker cover

Source: TT-Line
According to the first engineer, the top of the engine was accessed by walking along the catwalk adjacent to the cylinder heads and then up and over the B1 rocker cover, holding the pipes there for 3 points of contact. The first engineer also noted that work there often involved leaking cooling water or oil that made the rocker covers slippery and access via the B1 cover provided better footing (anti-slip tape) and handholds while avoiding the potentially hot exhaust manifold.
By contrast, the second engineer regularly used the route that involved walking along the top of the rocker covers while holding exhaust manifold to avoid the fuel pipes below B1 cylinder head and then stepping across the access gap in the railing (Figure 4). The air hose reel near the gap provided a handhold but it also swivelled.
Figure 4: B5 cylinder across catwalk

Source: TT-Line
Recorded video
The engine room was fitted with a closed-circuit television (CCTV) system with cameras in critical areas, including the incident location, to allow for remote monitoring and supervision. The ATSB obtained recorded video footage covering the period of the incident for its investigation analysis.
The video footage showed the second and third engineers accessing the top of the engine a total of 9 times on the accident morning. They stepped directly between the deck and the rocker covers on all occasions, except once when they used the route via the catwalk and climbed up over the B1 rocker cover.
The sequence of the second engineer’s slip and heavy fall was also recorded.
Safety management system
The International Safety Management (ISM) Code provides the international standard for the safe operation of ships.[4] The objective of the ISM Code is the prevention of human injury or loss of life and the avoidance of damage to the environment and property. To achieve this objective, companies are required to develop, implement and maintain a shipboard safety management system (SMS) that provides policies, procedures, instructions and guidance for all shipboard operations.
Spirit of Tasmania I’s shipboard SMS implemented by TT-Line included a ‘vessel operations manual’ for the effective identification and management of hazards to prevent accidents and environmental damage. The manual documented several procedures and processes related to risk management, including:
- hazard identification and risk management
- daily works committee
- Job Safety Analysis
- Take 5.
Risk management
The ‘hazard identifications and risk management’ procedure in the SMS provided guidance in assessing and managing safety risk for all shipboard operations. The procedure assigned responsibilities, documented the hierarchy of risk controls and provided various forms and tools that were to be used to comply with various procedures to manage risk.
Works committee
As part of its safety management, TT-Line had identified the need for high level control of ongoing work across shipboard departments, including engine room operations. This was done through a works committee on each ship. The works committee on Spirit of Tasmania I comprised the chief officer, first engineer and hotel manager as the heads of their respective departments, and the chief integrated rating (CIR)[5], shipwright and the safety and environment officer.
The works committee met every day and compiled a daily work schedule listing all planned work for each department. The committee was required to consider the ‘entire scope of proposed work’, assess the risks involved in each job using the risk assessment form and log the outcome on the daily work schedule. Where work consisted of multiple parts, each part had to be assessed individually. In addition, the committee had responsibility for preventing simultaneous operations conflicting with each other and in managing risk and supervising contractors working on board.
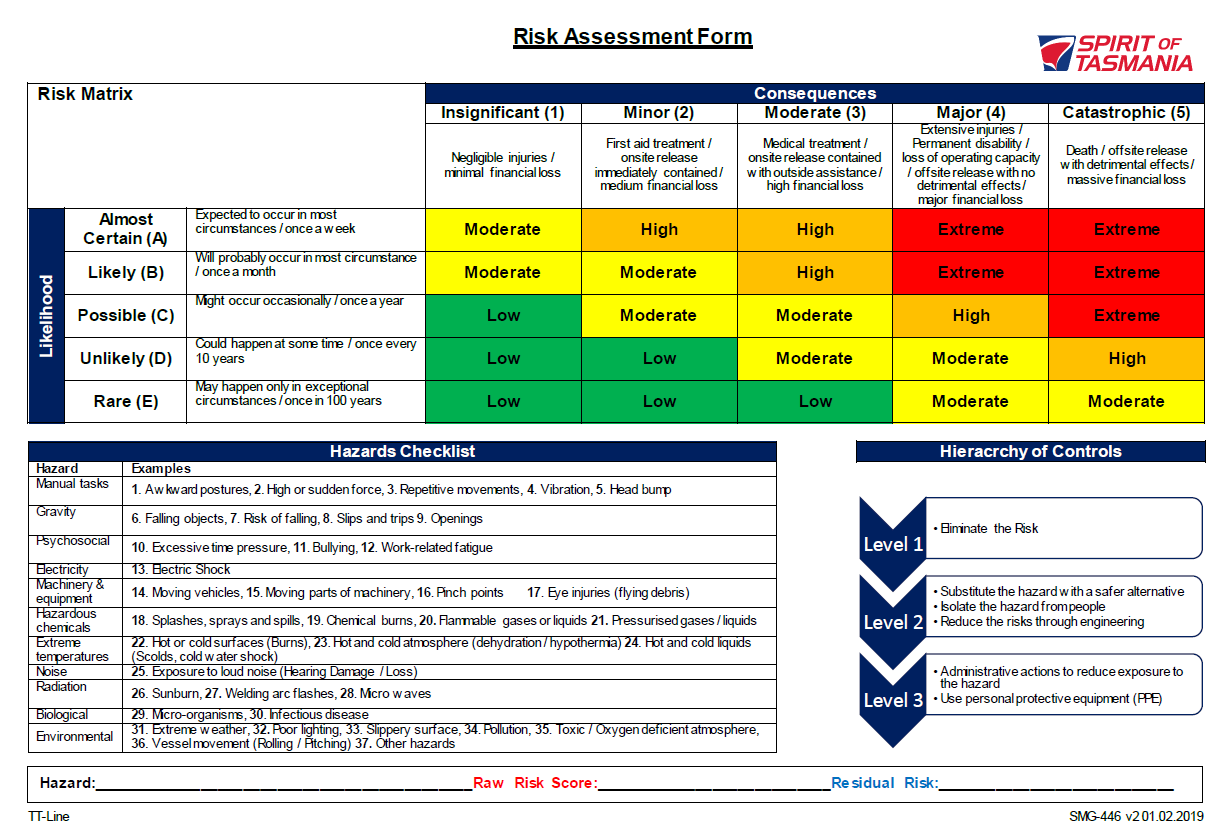
Hazards for each job were to be identified based on a ‘hazard identification table’, which listed the general categories of hazards. Based on these categories, each job was assigned an initial ‘raw risk score’ or rating, which, after application of existing controls and additional personal protective equipment (PPE), resulted in final risk score (that is, the residual risk).
Any jobs with an initial risk score higher than ‘low’ in the risk assessment matrix (Appendix A – Risk Assessment Matrix) required the application of additional controls, including extra PPE, a permit to work or other administrative or technical controls. These controls were then to be documented and implemented through a Job Safety Analysis (JSA).
On 6 March (the accident date), the works committee’s daily work schedule form listed 6 jobs in the engine department, all 6 related to a category of work rather than specific jobs. All planned maintenance work on the engines was captured in one line as ‘Aux eng / ME AMOS routines and service’. The form identified ‘physical’ and ‘mechanical’ hazards under the ‘personal injury/death’ general category. The initial risk score was assessed as 3D or ‘moderate’. To mitigate this risk the form noted that a number of controls were in place, these included the use of personal protective equipment (PPE), lock-out/tag-out (LOTO) procedures and Job Safety Analysis. These reduced the final risk score on the form to 3E or ‘low’.
Job Safety Analysis
Spirit of Tasmania I’s SMS included a procedure for conducting Job Safety Analysis (JSA). This procedure defined the responsibilities for implementation, guidance on risk assessment and mitigations as well as the administrative requirements.
JSAs were normally completed by the works committee in the planning stage of a job during their daily meeting. However, for unexpected work the supervisor in charge would assess the need for a JSA and complete one if required.
Additionally, if during a task a situation occurred that had not been contemplated and planned for in the JSA, the risks were to be reassessed to determine whether a new JSA was required. If the change did not warrant a new or updated JSA, the procedure required that a ‘Take 5’ be completed (see the following section).
The JSA process required breaking down the work into its component steps and assessing the potential hazards involved in each. The initial or ‘raw’ risk score was then calculated by assessing the risk without controls in place. The risks could then be mitigated based on the hierarchy of controls, reducing the final or ‘residual’ risk score to an acceptable level.
After completion, the JSAs were to be approved by either the master, chief engineer, Health Safety & Environment committee[6] or the marine manager ashore. The person supervising the work was then required to ensure that everyone involved was familiar with the JSA and sign the form before starting the work.
Approved JSAs were filed electronically and a JSA for the same (or effectively the same) job that was regularly performed could be re-used without further approval. Any changes to such JSAs, however, required another approval process.
A JSA covering the initial oil change had identified ‘slips and fall’ as a hazard but was mostly concerned with the cleanup of oil spills. As the oil change could be completed from deck level access the engine top was not required.
While both the first and second engineers stated that a JSA covering the exchange of the cover plate ‘should’ have been filed, no attempt was made to review this JSA. In any case, there was no such JSA in the files.
Two JSAs had been documented for work that required access to the top of the main engine. One JSA covered replacement of the ‘turbo exhaust gasket’ and the other covered the exchange of ‘exhaust expansion bellows’. Both JSAs identified the risk of falls when applying force to undo fasteners while standing on the engine (as opposed to the risks involved in getting to and from the top of the engine). The control measures to mitigate the risk when removing fasteners were ‘tools in good order’, ‘maintain good footing’ and ‘clean up any spills’.
Take 5
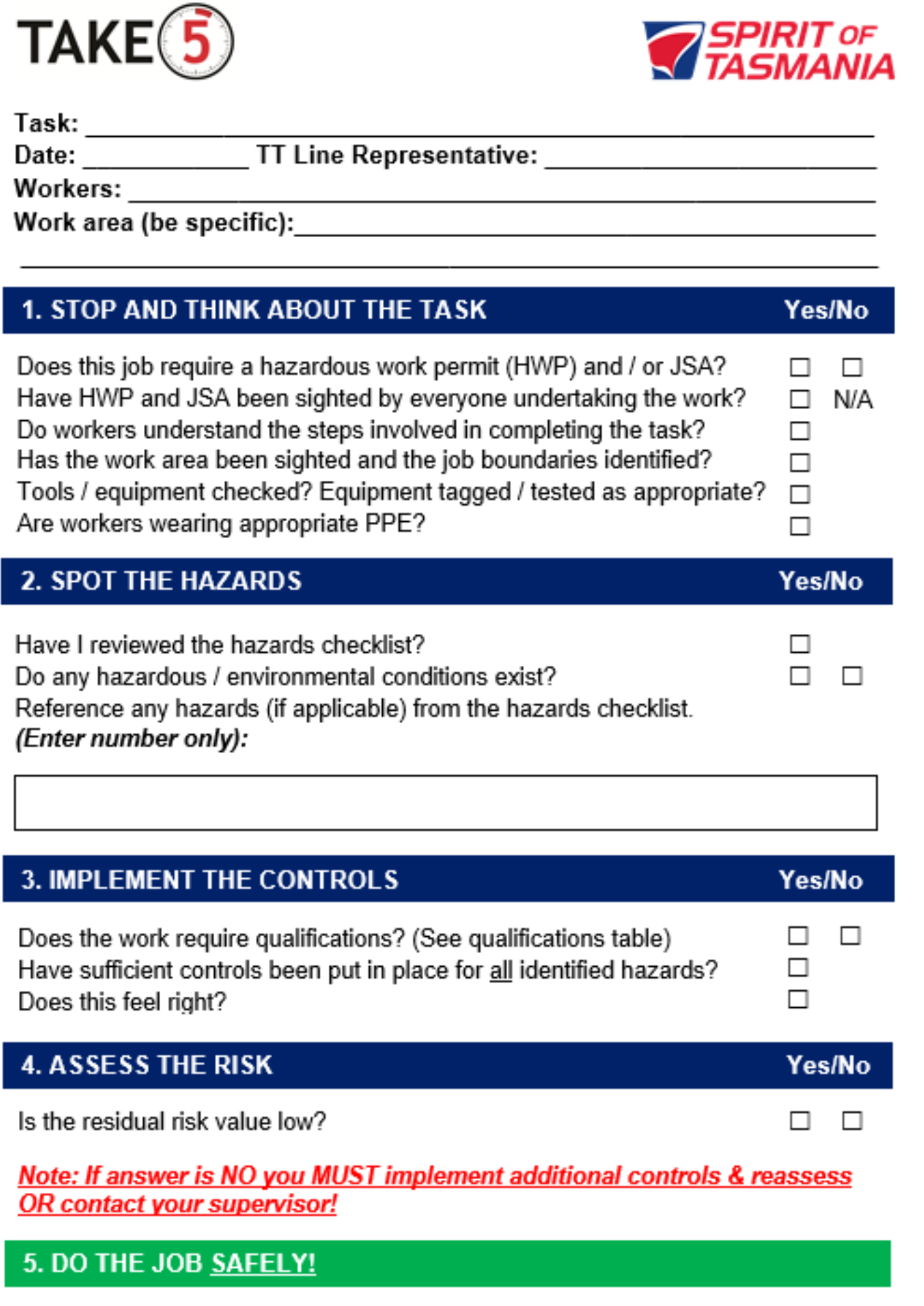
The ‘Take 5’ checklist (Appendix B – Take 5 checklist) provided an additional layer to mitigate risk. This lower level control was implemented at the worksite, with all the crew involved discussing the requirements of the job to ensure a shared mental model and as a final check of the hazards/risks that were unforeseen during the JSA planning process. This process was intended to complement any works committee standard protocols already in place, including but not limited to formal risk assessments, JSAs, and hazardous work permits.
The checklist was required to be used for all on board work other than a limited number of specified jobs deemed to be ‘standard shipboard practice’, which for the engineering department were defined as ‘standard engineering watchkeeping routines’.
The Take 5 process specified the following 5 steps:
Stop and Think about the Task: When a “no” response is not shown on the checklist, it indicates that the work can only proceed if the “yes” response is ticked. A question is only not applicable (N/A) if that response is shown.
Section 2 – Spot the Hazards: All workers must assess the worksite together to identify any hazards. To facilitate this, workers should utilise the hazards checklist on the reference page. The corresponding number for each hazard must be entered in the space provided in section 2 of the Take 5 checklist.
Section 3 – Implement the Controls: Any qualifications required to undertake the work should be checked according to the qualifications table on the information page. Control measures then need to be implemented to mitigate all hazards identified in section 2.
Section 4 – Assess the Risk: The risk should be assessed using the risk matrix on the reference page. The residual risk value must be Low for any given hazard. If the residual risk is moderate, additional controls should be implemented, and the risk reassessed. If the residual risk is high or extreme or you are in doubt, you must seek assistance from a TT‑ Line supervisor.
Section 5 – Do the Job Safely: Once the Take 5 checklist has been completed, work can proceed if assessed as safe to do so.
The procedure stated that the checklists were to be retained on board for one month, and that supervisors should randomly review 5 of them every month to verify compliance. After one month, the checklists were to be retained in the company’s records ashore for at least 6 months.
No Take 5 form covering the work was found and interviews with the involved crew confirm that a Take 5 was not completed before the replacement of the cover plate.
Previous incidents
In 2011, an engineer was seriously injured after falling through an open grating in the engine catwalk in the engine room of Spirit of Tasmania I. The ATSB investigation into that incident concluded that the personnel involved had not taken the time to (informally) assess the risks involved, which meant that no barriers were in place.
In 2022, a contractor working in the ship’s engine room was seriously injured due to the uncontrolled movement of a suspended load. The work was being supervised by the ship’s engineers under the shipboard SMS procedures, which were later amended to reflect the lessons learned. That incident was investigated by WorkSafe Victoria.
Safety analysis
Work site
Access
Although access to the top of the engine was regularly required for maintenance and was not straightforward, a dedicated ladder or platform was not fitted to provide safe access. Instead, the aft most rocker cover (B1) had been fitted with anti-slip material, which some crewmembers considered the ‘normal’ route to climb on or off the engine (Figure 2).
However, other crewmembers used different access routes which they considered better, convenient or safer. There were no standard procedures or practices to control access via a defined route(s). Consequently, different routes were used with the one used at the time of the accident having a high fall risk.
Contributing factor A standard safe route to access the top of the main engine was not defined or used. As a result, crewmembers used different routes, with the injured engineer using an unsafe route. |
Risks
Recorded video footage from the morning of 6 March shows that the 2 engineers on watch climbed on or off the engine a total of 18 times. On 16 occasions, they did so by walking along the rocker covers and stepping over the catwalk (Figure 2). Both engineers climbed up via the B1 rocker cover on one occasion.
Access via the B1 rocker cover had the advantage of the anti-slip tape on the cover and the cooling water pipes there providing a handhold for three points of contact. This reduced but did not eliminate the risk of a slip and fall.
On the other hand, walking along the gloss painted, inclined rocker covers did not provide safe footing which meant a high risk of slips and falls. While the exhaust manifold provided a handhold, a good handhold was not available when stepping across to (or from) the deck. Further, the higher drop from the B4-5 covers to the catwalk increased the risk of injury, which was realised when the engineer slipped and fell.
Contributing factor After working on top of the main engine, the second engineer walked along its rocker covers before stepping across to the opening in the railing, slipping off the cover and falling, resulting in serious injury. |
Risk controls
Work scope change
Spirit of Tasmania I’s shipboard safety management system (SMS) procedures required any significant change in the scope of the work being carried out to be reassessed for additional hazards. Such reassessment could result in changes to the applicable risk controls. In general, this would lead to either updating the existing job safety analysis (JSA) or, if that was not deemed necessary, conducting another ‘Take 5’.
On 6 March, the oil change being carried out was rescoped and the job was changed to the replacement of the bearing housing covers. This significant change in scope should have resulted in the engineers conducting another Take 5 before starting the job. This Take 5 would have provided the opportunity to assess safe access to the top of the engine, which in turn would have flagged the need for a JSA.
The engineers were aware of the need to conduct a Take 5. While it was possible to depart with number 1 engine off-line, the second engineer felt self-imposed pressure to complete the work before the planned departure. This probably resulted in the engineers that were replacing the cover not conducting a Take 5. The first engineer’s perception was that it was low risk work because it was regularly done and therefore they had not considered that another risk assessment or JSA was necessary.
Contributing factor Although the engineers knew that replacing the bearing housing cover was a change to work scope and that this required reviewing the existing Job Safety Analysis and/or conducting a Take 5, neither was undertaken due to perceived time pressure and a perception that the work was low risk. Consequently, the risk of slips and falls involved in the work was not properly considered. |
Job Safety Analysis
The evidence showed that main engine turbocharger bearing housing cover plates had been regularly replaced for many years. Replacing the cover plates meant accessing the top of the engine and SMS procedures required appropriate risk controls in place, based on a risk assessment documented in a JSA. All JSAs were to be filed in an electronic system for later use.
However, no JSA for replacing cover plates was found in the system. Both engineers that replaced the cover plate stated that a JSA ‘should’ have existed but made no attempt to access it. Regardless, a JSA to safely complete this job was not in place at the time of the incident. Further, given the absence of a JSA in the system, it is very likely that this job was undertaken many times in the past without proper consideration of the involved risk.
The ATSB investigation also reviewed risk assessments for various jobs involving work on top of the engines that were filed in the ship’s records. In every case, the risk was assessed as ‘medium’, which required a corresponding JSA to be completed, identifying the risk controls specific to the job, including those relevant to accessing the engine top. There were 3 JSAs for work on the turbocharger and exhaust system. Each identified slip and trip hazards when dismantling parts while standing on top the engine. Measures to mitigate these hazards focused on cleaning up spills and maintaining footing when using force to undo fasteners (bolts). None of the JSAs identified the hazards and risks involved in accessing the top of the engine.
Other factor that increased risk Spirit of Tasmania I’s safety management system procedure for Job Safety Analyses (JSA) was not effectively implemented. As a result, the JSA required for replacing the main engine turbocharger bearing housing cover plate was not in place. In addition, JSAs covering other work on top of the engine did not address the risks involved in accessing the work site. (Safety issue) |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the serious fall injury in the engine room of Spirit of Tasmania I, Geelong, Victoria, on 6 March 2025.
Contributing factors
- A standard safe route to access the top of the main engine was not defined or used. As a result, crewmembers used different routes, with the injured engineer using an unsafe route.
- After working on top of the main engine, the second engineer walked along its rocker covers before stepping across to the opening in the railing, slipping off the cover and falling, resulting in serious injury.
- Although the engineers knew that replacing the bearing housing cover was a change to work scope and that this required reviewing the existing Job Safety Analysis and/or conducting a Take 5, neither was undertaken due to perceived time pressure and a perception that the work was low risk. Consequently, the risk of slips and falls involved in the work was not properly considered.
Other factors that increased risk
- Spirit of Tasmania I’s safety management system procedure for Job Safety Analyses (JSA) was not effectively implemented. As a result, the JSA required for replacing the main engine turbocharger bearing housing cover plate was not in place. In addition, JSAs covering other work on top of the engine did not address the risks involved in accessing the work site. (Safety issue)
Safety issues and actions
Job safety analysis implementation
Safety issue number: MO-2025-002-SI-01
Safety issue description: Spirit of Tasmania I’s safety management system procedure for Job Safety Analyses (JSA) was not effectively implemented. As a result, the JSA required for replacing the main engine turbocharger bearing housing cover plate was not in place. In addition, JSAs covering other work on top of the engine did not address the risks involved in accessing the work site.
Safety action not associated with an identified safety issue
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, it has carried out to reduce the risk associated with this type of occurrence in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence. |
Additional safety action by TT-Line Company
| Action number: | MO-2025-002-PSA-02 |
| Action organisation: | TT-Line Company |
| Action status: | Closed |
In order to address the tendency for the Turbo Charger (TC) drain plug to become damaged during removal for oil change, TT-Line implemented a redesign and modification of the internal thread, which should eliminate the need for urgent replacements of the turbocharger bearing cover plate.
Glossary
| CCTV | Closed-circuit television |
| CIR | Chief integrated rating |
| CPP | Controllable Pitch Propeller |
| HS&E | Health Safety & Environment Committee |
| IMO | International Maritime Organization |
| IR | Integrated rating |
| ISM | International Management Code for the Safe Operation of Ships and for Pollution Prevention, 1995, as amended |
| JSA | Job Safety Analysis |
| SMS | Safety management system |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the chief, first and second engineers of Spirit of Tasmania I
- TT-Line Company (TT-Line)
- WorkSafe Victoria.
References
International Maritime Organization. (1995). International Management Code for the Safe Operation of Ships and for Pollution Prevention (ISM Code) as amended, IMO, London.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the master of Spirit of Tasmania I
- the chief, first and second engineers of Spirit of Tasmania I
- TT-Line
- Australian Maritime Safety Authority (AMSA)
A submission was received from:
- TT-Line
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Risk Assessment Matrix
Appendix B – Take 5 checklist
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] The Spirit of Tasmania passenger/Ro-Ro ships operate either on a single (overnight) sailing or double sailing, on which they provide both a day and a night‑time voyage between Geelong and Devonport.
[2] Ro-Ro or ‘Roll-on Roll-off’ ships carry wheeled cargo that is loaded and unloaded via ramps onto vehicle decks.
[3] Anecdotal accounts from the crew indicated that the anti-slip tape was applied after a previous fall but the ATSB found no record of that incident or any information about the application of the anti-slip tape.
[4] International Maritime Organization, 2018, International Management Code for the Safe Operation of ships and for Pollution Prevention (ISM Code) as amended, IMO, London.
[5] The chief integrated rating is the lead rating on board, comparable to the function of Bosun on international ships.
[6] TT-Line procedures included a Health Safety and Environment committee, to satisfy the requirement for a Health and Safety committee under the “Occupational Health and Safety (maritime industry) Act of 1993.
Occurrence summary
| Investigation number | MO-2025-002 |
|---|---|
| Occurrence date | 06/03/2025 |
| Location | Geelong |
| State | Victoria |
| Report release date | 27/11/2025 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Marine |
| Marine occurrence category | Injury |
| Occurrence class | Accident |
| Highest injury level | Serious |
Ship details
| Name | Spirit of Tasmania 1 |
|---|---|
| IMO number | 9158446 |
| Flag | Australia |
| Destination | Port of Geelong, Victoria |