
Final report
Report release date: 26/09/2025
Investigation summary
What happened
On 6 May 2025, the oil tanker Wisdom Venture was drifting off Sydney, New South Wales, when the engineering team commenced maintenance on the main deck steam valve for the cargo heating system. The valve had been leaking from the bonnet joint gasket.
Following isolation of the system, the team removed the valve bonnet. During this process, residual hot condensate was suddenly released, resulting in burn injuries to 3 crew members.
First aid was administered on board, and the injured personnel were subsequently evacuated to shore for medical treatment.
What the ATSB found
The ATSB found that prior to commencing maintenance work on the cargo heating system main deck steam valve, the crew did not allow adequate time for the steam system to cool. In addition, the verification system to ensure that the steam line was fully depressurised was not used. This was most likely due to the time pressures to reintroduce heating to the main engine fuel system.
The ATSB also found that a drain line in the warm-up bypass line had been permanently modified without formal approval or documentation. This change was not incorporated into a risk assessment and no formal review was conducted. This undocumented change likely introduced a system vulnerability that undermined the effectiveness of the steam system isolation.
Additionally, the modification was not identified in the chief engineer’s handover process, leaving the incoming engineering team unaware of the altered configuration and associated risks. It was also not identified during routine technical inspections or superintendent riding visits. This resulted in the ship manager’s management of change process not being applied.
What has been done as a result
Following the incident, the ship manager advised that the drain line on Wisdom Venture has been returned to its original design configuration. A fleetwide campaign has also been initiated to identify any unauthorised modifications to shipboard piping systems. Where such modifications are identified, internal investigations will be conducted.
To raise awareness of the risks associated with undocumented engineering changes, the incident will be included in pre-joining briefings for senior engineering staff and discussed during crew seminars. Ship staff will also be reminded that all modifications must be undertaken in consultation with the office and in accordance with the company’s management of change process.
Finally, to improve oversight and strengthen management of change procedural compliance, the superintendent’s inspection report will be amended to include verification of any shipboard system modifications not reflected in the ship’s design drawings. These actions are intended to ensure that future modifications to critical systems are properly assessed, documented, and communicated.
Safety message
The incident highlights the critical importance of adhering to established safety and management of change procedures. Where changes are to be made to a system, these need to be recorded and the processes to identify the risks need to be followed to ensure there are no unintended consequences.
In addition, operators are reminded that maintenance involving steam systems must allow sufficient cooling time and include visual confirmation of isolation. Reliance solely on pressure indicators is not sufficient to ensure safe working conditions.
The occurrence
On 6 May 2025, the Aframax[1] oil tanker Wisdom Venture was drifting off Sydney, New South Wales, while awaiting berthing instructions. The ship had arrived from Geelong, Victoria, on 20 April 2025 and, due to prevailing weather conditions, the master kept the main engine on 10 minutes notice to maintain safe positioning during the drift.
The ship had a cargo of about 14,610 t of marine fuel oil, which required heating. At about 1300 local time,[2] the chief engineer led the engineering team to commence planned maintenance on the cargo heating system main deck steam valve (see the section titled Cargo heating system), which had been leaking from the bonnet joint gasket. The maintenance task required the cargo heating system to be shut down.
The team, which consisted of the second engineer, a fitter and an oiler, conducted a toolbox meeting and implemented isolation procedures (see the section titled Safety management system), including shutting steam supply valves, draining the steam line by opening the drain valve, and confirming zero pressure on the fitted gauge on the steam line before and after the pressure‑reducing valve. The team then began removing the valve bonnet with the aid of a chain block.
At approximately 1400, while lifting the bonnet, residual hot condensate was suddenly released, splashing onto nearby team members. The second engineer sustained first‑ and second‑degree burns. The fitter and the oiler sustained first‑degree burns.
The injured personnel were immediately transferred to the ship’s medical room, where first aid was administered, including cold water treatment, antiseptic cream and pain relief medication. The master notified the ship’s onshore management and medical advisory service and contacted Sydney vessel traffic services (VTS)[3] to arrange medical evacuation.
At about 1500, the ship proceeded to the Sydney pilot boarding area. The injured personnel were then disembarked to a shore medical launch for hospital treatment at about 1918.
Context
Wisdom Venture
The Aframax oil tanker Wisdom Venture was owned by Acclaim Shipping Limited, operated by Wah Kwong Ship Management (Hong Kong) and registered in Hong Kong. The ship was classed with Lloyd’s Register.
Crew
At the time of the incident, Wisdom Venture had a crew of 24 personnel, and all were appropriately qualified and endorsed for the positions they held.
The master had over 12 years of watchkeeping experience, including 6 years on oil tankers and about 2.5 years as master. The chief officer had about 8.5 years of oil tanker experience. The second and third officers each had several years of relevant service.
The chief engineer had about 9.5 years of experience on oil tankers, including 2.5 years in the role of chief engineer. The incident occurred during a scheduled crew change, and the chief engineer was in the process of being relieved. The relieving chief engineer had 4 years of experience as chief engineer. They joined the ship on 17 April 2025 in Geelong, to conduct a parallel handover with the outgoing chief engineer.
The second engineer had approximately 7.4 years of experience. The third and fourth engineers each held officer of the watch (engine) certificates of competency. An electro‑technical officer (ETO), certified for both oil and chemical tankers, was also on board at the time of the incident.
All officers had completed advanced tanker safety training and demonstrated strong English proficiency. Most had prior experience on similar ships and had completed multiple tenures.
Environmental conditions and operations while drifting
Between 20 April and 6 May 2025, Wisdom Venture drifted off the coast of Sydney, while awaiting berthing instructions. During these periods, the ship maintained position within designated drifting zones, outside port limits. Environmental conditions were generally calm, with recorded speeds over ground ranging from 0.5 to 5.4 knots. The ship’s main engine was routinely placed on 10 minutes standby notice and was periodically started to reposition or adjust drift trajectory.
Engine control was frequently shifted between the engine room and bridge, with telegraph tests and main engine tests conducted before each use. These operations were logged with precise positional data, indicating careful monitoring and control during drifting phases.
During the drifting period, the engineering team, under the direction of the chief engineer, initiated several maintenance tasks. These included:
- major maintenance on a main engine unit
- replacement of main engine fuel valves
- overhauling of diesel generator engine cylinder heads and pistons
- rectification of a steam leak from the bonnet flange joint of the cargo heating system main deck steam valve, located in the engine room.
Steam system purpose and configuration
Wisdom Venture operated a high- and low-pressure steam system (Figure 1) that supported a range of essential onboard functions. The steam was generated through 2 auxiliary boilers and an exhaust gas boiler (when the main engine was in operation). The exhaust gas boiler could be connected to either of the auxiliary boilers via a circulating pump, allowing for flexible integration of waste heat recovery. Each auxiliary boiler was fitted with a main steam stop valve at the steam outlet, directing steam from either boiler into the main steam line located in the engine room.
Downstream of these main steams stop valves, the steam line divided into 2 branches supplying:
- high pressure steam (0–1.6 MPa) for the cargo and ballast pumping plant
- low pressure steam (0–0.9 MPa) for the auxiliary systems.
On the day of the accident, the cargo and ballast pumping system were not in use.
Figure 1: Simplified diagram representing the steam system
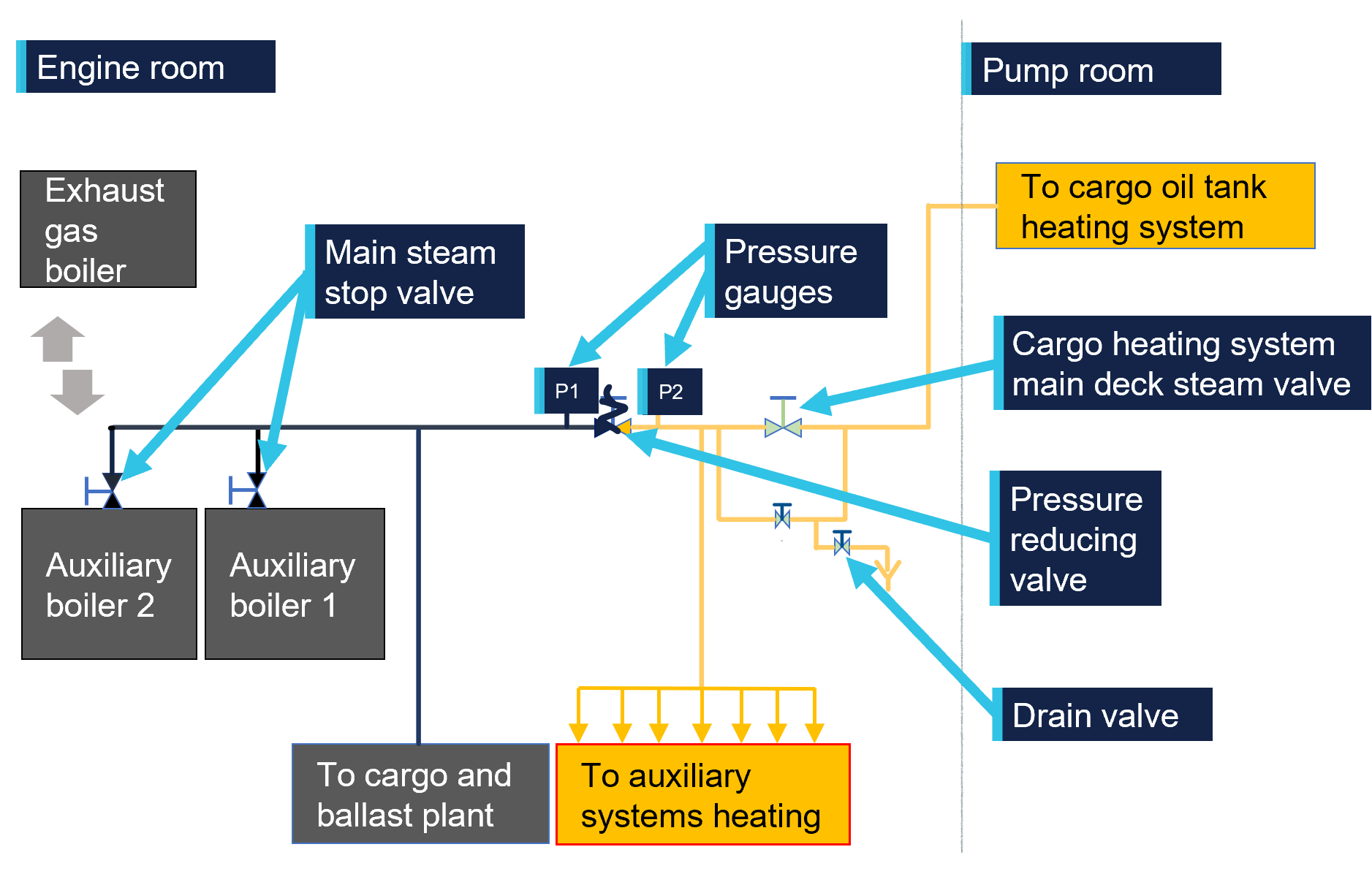
P1: Pressure gauge before the reducing valve (high pressure side)
P2: Pressure gauge after the reducing valve (low-pressure side)
Black line shows high pressure steam. Yellow line shows low pressure steam. Exhaust gas boiler could be connected to any one of the auxiliary boilers through a water circulating pump. Source: ATSB
Auxiliary heating system
The high-pressure steam for the auxiliary systems passed through a pressure‑reducing valve. To verify the correct operation of the valve, pressure gauges were fitted both before and after it. This arrangement enabled monitoring of pressure differential and ensured the valve was functioning within its designed parameters. It also allowed the crew to see if there was pressure in the auxiliary system.
Following pressure reduction, the steam line, located in the engine room, branched out to supply heating to various auxiliary systems including:
- marine fuel oil
- purifiers
- engine room tanks
- hot water circulating system
- accommodation.
The steam line then continued to the valve for the cargo heating system.
Fuel oil heating
The ship’s main engine, generator engines and auxiliary boilers were configured to operate using either marine fuel oil (MFO) or marine gas oil (MGO). MFO required heating to reduce its viscosity and enable effective atomisation and combustion. Without sufficient heating, MFO becomes too viscous for reliable operation.
Where the heating steam was required to be fully shut down for maintenance, the normal practice was to switch the engine fuel supply system to MGO as it does not require heating and can be used directly. However, transitioning from MFO to MGO necessitated purging the fuel system of residual MFO. This process resulted in the loss of a large quantity of MGO, with implications for fuel efficiency, environmental management and operational planning.
When required for short periods of time, the steam system could be shut down, however, it took a considerable amount of time for the system to cool fully before maintenance could be carried out. Additionally, the heating system could only be safely shut down for a limited window, estimated to be less than 30 minutes, before fuel viscosity would begin to affect engine performance (see the section titled Process on the day). This constraint was evident during the shutdown process on 6 May 2025, where fuel temperature alarms were triggered as the heating system remained offline beyond this window.
Cargo heating system
The cargo heating system was designed to keep viscous liquids like marine fuel oils at the right temperature so they could be pumped easily when the fuel was being offloaded. To do this, the system used low-pressure steam, through a network of pipes in the cargo hold. The cargo fuel was required to be kept within a heat range and was not required to be running continuously.
Low pressure steam passed through the main deck steam valve (Figure 1 and Figure 2), the last valve in the steam line in the engine room, which led to the deck and the cargo heating system. This valve was the main steam isolation valve for the cargo heating system. It was closed when cargo heating was not required and played a critical role in making sure the system could be safely shut down for maintenance and isolating the deck heating system during emergencies.
Figure 2: Cargo heating steam main line in engine room
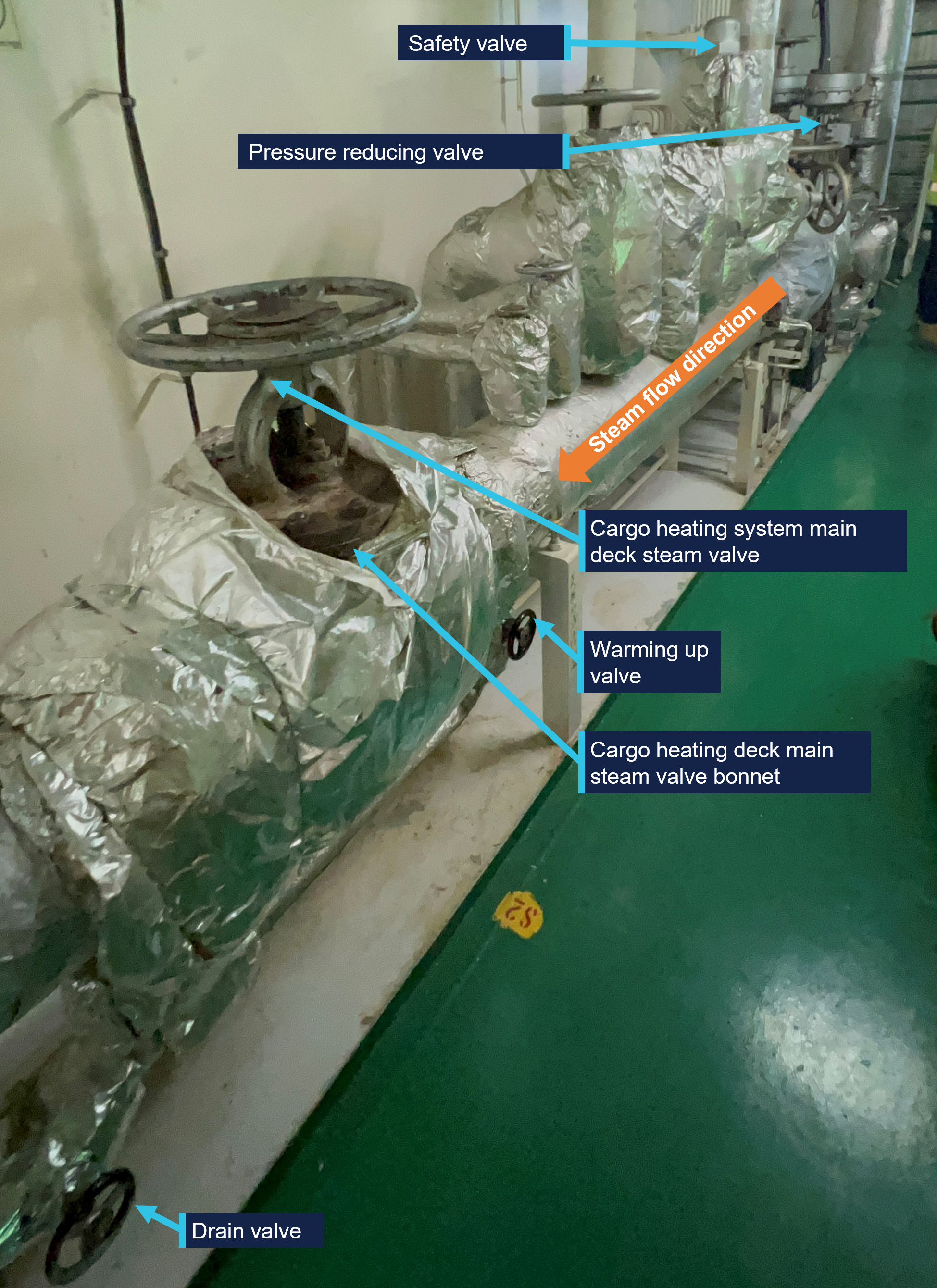
Source: ATSB site photograph
Cargo heating procedure
Prior to introducing steam for the cargo tank heating system, the main deck steam valve remained closed while preparatory actions were undertaken. To mitigate the risks of thermal shock and water hammer through the cargo heating system, steam was slowly introduced through a warming-up line, a line which bypassed the main deck steam valve. Until the system was at working temperature, steam would condense, producing boiling water, which drained through drain valves throughout the system. This included a drain line, on the warming-up line, which led to an engine room floor drain hopper. The presence of condensate was verified by visual inspection of the drain at the outlet.
Throughout the heating process, system temperature and pressure were continuously monitored. Once it was established that the system was warmed and condensate was no longer being drained, steam was gradually introduced to the cargo heating system through the main deck steam valve. Once the valve was fully opened and system stability was confirmed, the warming-up system was isolated, and the drain valve was closed.
System modification
During the site inspection, the ATSB identified a permanent modification to the drain line from the warming-up line (Figure 3). It was reported that the modification was to save water by redirecting condensate away from the open drain hopper (which led to the engine room bilges) and returning the water to the boiler feedwater system.
Figure 3: Drain line modification
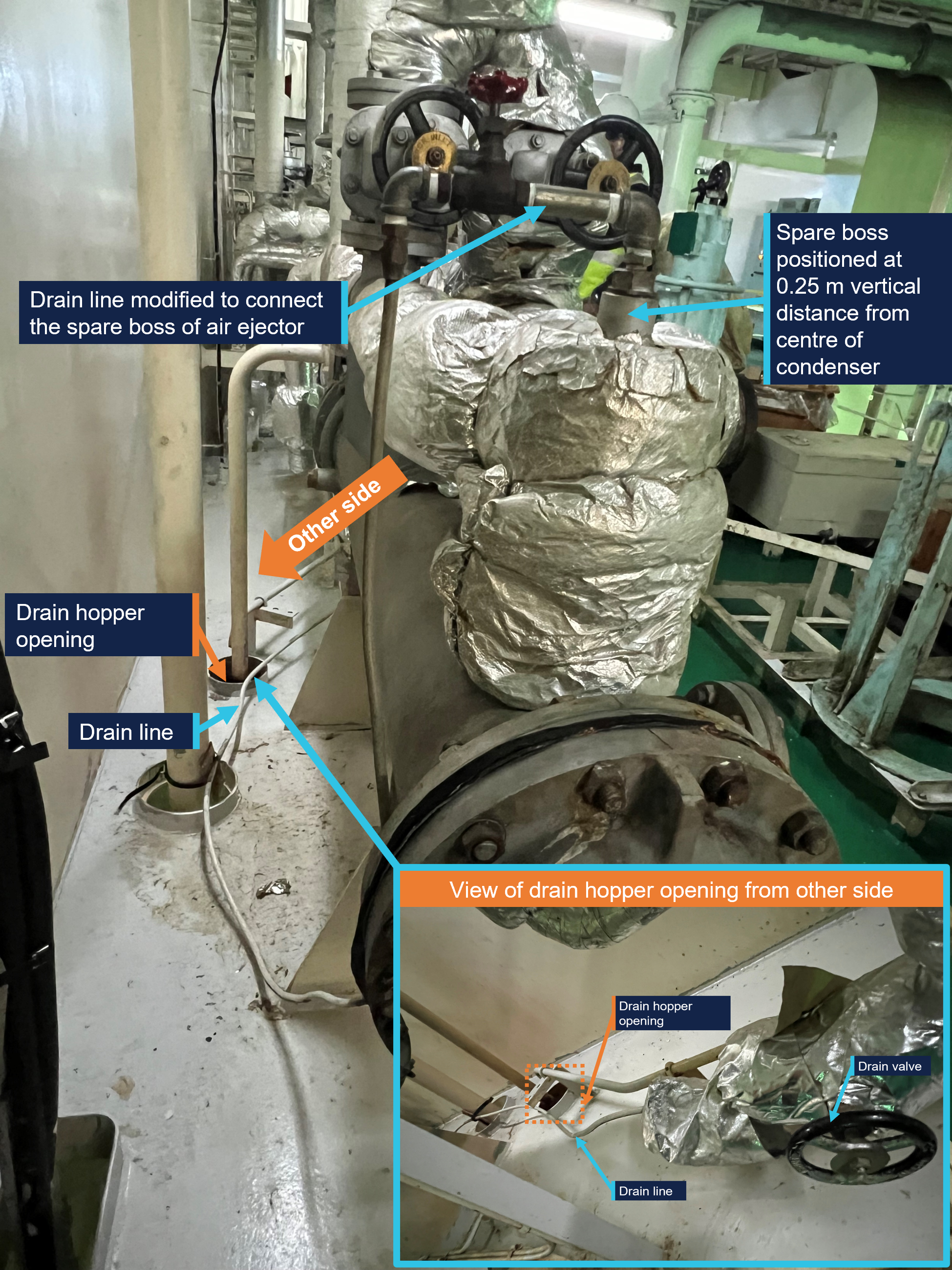
Source: ATSB site photograph
The modification connected the drain line to a spare boss[4] on the condenser for the air ejector. The condenser was at approximately the same vertical elevation as the stop valve, with the boss about 0.25 m above the condenser. The connection was established using a fabricated pipe assembly comprising unions, elbows and a bronze union bonnet globe valve.
Process on the day
On 5 May 2025 at 1200, in preparation for planned maintenance on the main deck steam valve, the cargo heating was stopped.
On 6 May 2025 at 1200, in accordance with the ship’s safety management system (SMS) (see the section titled Safety Management System), the master and chief engineer issued the following permits:
- Cold work permit: authorised the overhaul activity under controlled conditions, confirming personnel briefing, hazard isolation, and personal protective equipment (PPE) compliance.
- Risk assessment: identified potential generic hazards including steam backflow, equipment malfunction and confined space risks, with mitigation measures documented and endorsed.
- Isolation permit: outlined the lockout/tagout procedure to prevent unintended release of hazardous energy. Isolation points included:
- auxiliary boiler main steam and warm up valves shut before and after the operation
- valves before and after pressure regulating in closed position
- line drained and kept open.
They were executed by the team, which consisted of the second engineer, a fitter and an oiler.
Despite preparations to isolate the steam system, the shutdown was carried out without switching the fuel systems for the main engine, auxiliary engine, and auxiliary boilers (each of which required heating) to alternative fuel that did not rely on steam heating.
The auxiliary boiler alarm monitoring system reflected the system’s abnormal status during the steam isolation and restoration process. The system was shut down at 1347, triggering an alarm. A temporary recovery was observed at 1452, followed by a second abnormal alarm at 1454, with full recovery noted at 1457. These timestamps indicated the duration of the steam system isolation and restoration, and the periods during which the auxiliary boiler steam system was not operational.
At 1430, fuel oil inlet temperature alarms were triggered for the main engine, indicating that the marine fuel oil temperature had dropped to 105°C. At 1450, similar alarms were triggered for the marine fuel oil system for the diesel generator. These alarms reflected inadequate heating across the fuel systems, which impacted operational readiness. The steam system was turned back on at approximately 1452, restoring the necessary heating and resolving the abnormal conditions.
Prior to the removal of the main deck steam valve bonnet holding nuts, steam pressure was confirmed to be zero on the pressure gauges fitted on the steam line, both before and after the pressure‑reducing valve. The crew advised that both pressure gauges were indicating zero before they commenced work.
Post-incident interviews revealed that the modified drain line had not been disconnected for visual inspection, and the warming-up line valve remained closed during the depressurisation process.
Safety management system
The ship’s safety management system (SMS) incorporated a permit to work (PTW) system to manage non‑routine and potentially hazardous tasks. The PTW system required formal authorisation prior to commencing work such as hot work, electrical maintenance, enclosed space entry, or operations involving pressurised systems, including steam. Before issuing a permit, responsible officers were required to complete supporting activities, including system isolation (where required), verified through an isolation certificate.
Isolation procedures
Isolation was required when work involved:
- breaching pipeline systems or opening pumps
- working on electrical or pressurised systems
- conducting maintenance in enclosed spaces or on cargo systems.
The isolation procedures ensured that all energy sources were identified, isolated, and verified to be in a zero‑energy state before work commenced. This included mechanical, electrical, hydraulic, pneumatic, thermal, and chemical energy. The process then required that lockout/tagout (LOTO) procedures were used to secure and label isolation points, with clear signage such as ‘Do not operate – work in progress’.
The isolation permit process included:
- planning and identifying all lockout/tagout points
- notifying affected personnel
- physically locking and tagging energy sources
- verifying isolation through testing
- continuous supervision and documentation.
Risk assessment
The SMS required that risk assessments be conducted by appropriately experienced personnel, with specialist input sought where necessary. This process was intended to identify and mitigate hazards associated with the task, including risks such as energy release, system pressurisation, or ignition sources.
The company’s risk assessment form was the designated tool for documenting this process and supporting safe operational decision‑making.
Training and awareness
The SMS emphasised the importance of ensuring that all personnel involved in potentially hazardous work were adequately trained and aware of the procedures and risks associated with its tasks.
Chief engineer’s handover
The SMS outlined a structured handover process for the chief engineer to ensure continuity and operational safety. As part of this process, a disembarking chief engineer was required to provide the incoming chief engineer with a comprehensive briefing on the status of all machinery and systems under their responsibility, including any modifications or deviations from standard configurations. The handover was recorded in the handover checklist and verified during joint inspections.
The ATSB could find no records of the identified modification being recorded in the records of previous chief engineers’ handover checklists.
Technical visits
The SMS mandated that each ship was inspected by a technical superintendent at least twice per year, with no more than 6 months between visits. These inspections were conducted using structured checklists and were intended to assess the operational condition of machinery, safety systems and compliance with maintenance standards.
During the visit, the superintendent:
- verified the status of the planned maintenance system (PMS)
- evaluated the readiness of critical systems, such as steam lines
- reviewed any modifications or deficiencies
- documented observations and discussed them with shipboard management
- established timelines for corrective actions
- provided onboard training and conducted appraisals of senior officers.
These visits were required to support alignment with company standards and continuous improvement in technical and safety performance.
The ATSB did not identify any records of the identified modification in the technical visit records.
Management of change procedures
The ship manager had established a management of change (MoC) process to ensure that any modification to shipboard systems, design, procedures or equipment was assessed, authorised and implemented in a controlled manner.
Fleet superintendents were required to conduct scheduled riding visits during which they:
- evaluated operational performance
- reviewed risk management checklists
- identified undocumented or emerging risks
- initiated the MoC process where changes were observed or proposed.
Engineering changes, as defined in the health, safety, and environmental (HSE) manual, included any modification to the ship’s structure, onboard systems, or control equipment that could affect operational integrity. Such changes were subject to formal risk assessment and required approval at the appropriate level of authority, depending on the scope and potential impact.
The MoC process mandated the use of a specific form to:
- document the change
- assess associated risks
- define mitigation measures.
Risk assessments were integral to the MoC process and were to be conducted in accordance with company procedures. These assessments involved identifying hazards, estimating the likelihood and consequences of its occurrence and implementing controls to reduce risk to an acceptable level. Fleet superintendents were expected to provide technical input, particularly in cases involving non‑routine repairs or modifications following equipment failure.
The ATSB identified 2 recorded MoC for the engineering department since the ship’s delivery:
- fuel compliance modification, MoC dated 8 January 2019
- exhaust gas cleaning system (EGCS) installation during dry dock, MoC dated 22 July 2022.
No other records of engineering‑related changes were available for review.
Post‑incident inspection
Following notification of this incident, the Australian Maritime Safety Authority (AMSA) attended the ship at Gore Bay terminal, Sydney, on 8 May 2025 to conduct an inspection. AMSA’s inspection concluded that isolation procedures had been followed, and appropriate personal protective equipment (PPE) was used. However, their investigation also stated that the piping arrangement allowed a section to remain enclosed without a drain, which likely led to vacuum formation and the subsequent release of condensate when the valve was opened.
During the port state control inspection, AMSA identified 2 deficiencies. The first related to the port side boiler pressure easing gear, which could not be operated from a safe position. The second involved crew unfamiliarity with the oily water separator, where the oil content monitor drain valve had been left open during testing. Both deficiencies were required to be rectified prior to the ship’s departure.
Safety analysis
Introduction
This safety analysis examines the key factors that contributed to the burn injuries aboard the Aframax oil tanker Wisdom Venture during maintenance on the cargo heating system main deck steam valve. It focuses on procedural lapses, undocumented system modifications, and inadequate verification practices that increased the risk of injury to crew members.
Incomplete isolation check
At the time of the incident, the ship was drifting with the main engine operating on marine fuel oil, which requires continuous heating to maintain viscosity. Most likely due to the amount of fuel required to be purged, the decision was made not to switch the engine fuel to marine gas oil prior to conducting the maintenance activity. In those circumstances, the heating system could only be shut down for a limited window, estimated to be less than 30 minutes, before fuel viscosity would begin to affect engine performance. This time constraint likely reduced the cooling time the crew allowed prior to removal of the valve bonnet.
The warming-up valve remained closed during depressurisation, and the crew relied solely on pressure gauge readings located before and after the steam pressure‑reducing valve to verify if the system had cooled sufficiently. Additionally, not opening the warming‑up line removed the opportunity for the pressure to stabilise on either side of the main deck steam valve, prior to commencing the maintenance work.
In addition, engineering crew members did not disconnect the modified steam drain line that had been permanently re‑routed to the air ejector condenser. This modification resulted in condensate remaining in the drain line as there was not sufficient pressure to overcome the head of pressure to the connection to the condenser.
In combination, this configuration did not allow for a positive visual confirmation that the line was free of steam or condensate. Consequently, when the valve bonnet was removed, residual hot condensate was released, resulting in significant burn injuries to 3 crew members.
Although the required cold work permit, isolation permit and risk assessment were completed, the documentation did not identify or address the operational risk associated with the modified drain line configuration. The absence of a verification step to confirm the line was fully depressurised meant that the isolation process was incomplete, and the potential for residual hot condensate discharge was not adequately mitigated.
Contributing factor Prior to commencing maintenance work on the main deck steam valve, the crew did not allow adequate time for the steam system to cool. In addition, the verification system to ensure that the steam line was fully depressurised was not used. This was most likely due to the time pressures to reintroduce heating to the main engine fuel system. This resulted in the release of residual hot condensate when the valve was opened, and injuries to 3 crewmembers. |
Undocumented drain line modification
Engineering drawings available on board clearly depicted the original configuration of the drain line, which discharged into an open hopper leading to the engine room bilges. However, during the ATSB’s on board inspection, investigators identified that the drain line had been permanently re‑routed to discharge into the steam side of the air ejector condenser system. This modification did not align with the original design intent and was not reflected in any schematics or technical documentation.
Interviews with both the outgoing and incoming chief engineers confirmed that the modification predated their tenures and had not been formally recorded or communicated during handovers. In addition, no references to the change were found in recent handover notes, and no supporting documentation was available to explain the rationale or timing of the modification.
This meant that a permanent modification was implemented without supporting documentation or formal engineering review. Additionally, the modification was not incorporated into any risk assessment or technical records, and no evidence was found to indicate that it had been subject to formal inspection or verification. This undocumented change introduced a system vulnerability that compromised the effectiveness of the steam system isolation.
On board the Wisdom Venture, a permanent modification to the steam drain line was implemented without documentation. During the modification process, the change was not incorporated into a risk assessment and no formal review was conducted. This undocumented change likely introduced a system vulnerability that undermined the effectiveness of the steam system isolation. (Safety issue) |
Unidentified engineering change
No documentation was found to indicate approval from the ship’s manager, classification society, or flag state for the modifications to the cargo heating system drain line. In addition, technical inspection records from the ship manager did not reference the modification, and condition reports rated the steam system as being in ‘good’ condition without noting any deviations.
The absence of observations, or non‑conformances, for this change suggests it was not detected during routine technical inspections or superintendent riding visits. This resulted in the Wah Kwong Ship Management (Hong Kong) management of change (MoC) framework, which required that any modification involving system layout changes be subject to formal risk assessment and documentation, not being effectively applied.
This unidentified modification highlights the importance of robust inspection protocols and documentation practices to ensure system integrity and compliance with approved design standards.
Other factor that increased risk A modification to the cargo heating main steam system drain line was not identified during multiple company superintendent’s visits. This resulted in the Wah Kwong Ship Management (Hong Kong) management of change framework, which required that any system modifications be subject to formal risk assessment and documentation, not being effectively applied. (Safety issue) |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the crew injuries during maintenance involving oil tanker, Wisdom Venture, about 60 km east of Sydney, New South Wales, on 6 May 2025.
Contributing factors
- Prior to commencing maintenance work on the main deck steam valve, the crew did not allow adequate time for the steam system to cool. In addition, the verification system to ensure that the steam line was fully depressurised was not used. This was most likely due to the time pressures to reintroduce heating to the main engine fuel system. This resulted in the release of residual hot condensate when the valve was opened, and injuries to 3 crewmembers.
- On board the Wisdom Venture a permanent modification to the steam drain line was implemented without documentation. During the modification process, the change was not incorporated into a risk assessment and no formal review was conducted. This undocumented change likely introduced a system vulnerability that undermined the effectiveness of the steam system isolation. (Safety issue)
- A modification to the cargo heating main steam system drain line was not identified during multiple company superintendent’s visits. This resulted in the Wah Kwong Ship Management (Hong Kong) management of change framework, which required that any system modifications be subject to formal risk assessment and documentation, not being effectively applied. (Safety issue)
Safety issues and actions
Undocumented drain line modification
Safety issue number: MO-2025-004-SI-01
Safety issue description: On board the Wisdom Venture, a permanent modification to the steam drain line was implemented without documentation. During the modification process, change was not incorporated into a risk assessment and no formal review was conducted. This undocumented change likely introduced a system vulnerability that undermined the effectiveness of the steam system isolation.
Unidentified engineering change
Safety issue number: MO-2025-004-SI-02
Safety issue description: A modification to the cargo heating main steam system drain line was not identified during multiple company superintendent’s visits. This resulted in the Wah Kwong Ship Management (Hong Kong) management of change framework, which required that any system modifications be subject to formal risk assessment and documentation, not being effectively applied.
Glossary
| AMSA | Australian Maritime Safety Authority |
| EGCS | Exhaust gas cleaning system |
| MFO | Marine fuel oil |
| MGO | Marine gas oil |
| MoC | Management of change |
| MPa | Megapascal |
| PMS | Planned maintenance system |
| PTW | Permit to work |
| SMS | Safety management system |
| VTS | Vessel traffic service |
Sources and submissions
Sources of information
The sources of information during the investigation included the:
- ship manager and the ship staff of ship Wisdom Venture
- ship manager’s safety management system
- shipboard checklists
- alarm logs
- medical treatment records.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- ship manager, master, chief engineer, fitter and oiler
- Australian Marine Safety Authority
- Hong Kong shipping registry
- Lloyd’s register of shipping.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] A tanker, usually between 80,000 and 120,000 dead weight tonnes.
[2] Local time was Eastern Standard Time (EST), which is Coordinated Universal Time (UTC) +10 hours.
[3] The Port Authority of New South Wales operates a 24-hour Vessel Traffic Service (VTS), with call sign ‘Sydney VTS’.
[4] A ‘spare boss’ refers to an unused pre-installed or moulded connection point or fitting on a pipe or pressure vessel.
Occurrence summary
| Investigation number | MO-2025-004 |
|---|---|
| Occurrence date | 06/05/2025 |
| Location | Near Sydney |
| State | New South Wales |
| Report release date | 26/09/2025 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Marine |
| Occurrence class | Accident |
| Highest injury level | Serious |
Ship details
| Name | Wisdom Venture |
|---|---|
| IMO number | 9773741 |
| Flag | Hong Kong |
| Departure point | Port of Geelong, Victoria |
| Destination | Gore Bay, New South Wales |